
Abstract
Introduction
Osteoarthritis of the knee (OA knee) is a common geriatric disease that require total knee arthroplasty. Periprosthetic fracture is one of the common complications, which is strongly related to metabolic bone disease.
Materials and methods
We conducted a prospective study on 291 outpatients with OA knee between November 2020 and April 2021. Baseline characteristics, dual-energy X-ray absorptiometry and blood test results were analysed using logistic regression analysis and expressed as odds ratio, 95% confidence intervals and P-values.
Results
Overall metabolic bone diseases were found in 82.91% of patients. Vitamin D insufficiency (53.38%) was the most prevalent, followed by osteopenia (44.38%), impaired renal function (26.69%), and osteoporosis (17.45%). Risk factors of vitamin D insufficiency are age ≥71 years (OR 0.33, P = 0.003) and bilateral affected side (OR 1.99, P = 0.007). For osteopenia and osteoporosis, risk factors were age, body mass index, affected side, and chronic kidney disease (P < 0.05).
Discussion
In the aspect of Vit D insufficiency, age>70 and bilateral OA knee were significantly related in many ways, such as reduction in cutaneous synthesis and daily exposure to sunlight and various diseases, including CKD and GI malabsorption. The risk factors of osteopenia and osteoporosis can be explained throughout several mechanisms. For instance, abnormality in hormone and cytokines metabolism will lead to the increase in adipocyte differentiation and fat accumulation. And that situation may lead to the decrease in osteoblast differentiation and increased osteoclast activity which could lead to negative impact on bone strength.
Conclusions
Metabolic bone diseases were common in most patients with OA knee, and the insufficiency in amount of vitamin D(serum 25-hydroxyvitamin D), osteoporosis, and osteopenia conditions were mainly identified. These preventable conditions have risk factors that are mostly correctable These preventable conditions have risk factors that are mostly correctable, for example gain more outdoor activities, consume vitamin D supplement or start osteoporosis treatment program. Further analysis is necessary to establish solid evidence in the comparison of risk factors between the OA and non-OA groups.
Introduction
Osteoarthritis of the knee (OA knee) is a common geriatric condition characterized by pain and limited range of motion, significantly impacting daily activities. Currently, treatments have advanced to delay knee degeneration by utilizing injectable hydrogel microspheres to mitigate degradation and promote cartilage regeneration. Ultimately, many patients may require total knee arthroplasty (TKA) in the end.1,2 Periprosthetic joint fracture is one of the common post-TKA complications, obtaining a concerning prevalence of 0.3%–2.5%. 3 Considered as a risk factor of periprosthetic fracture, metabolic bone disease was found to be strongly related to fractures due to the fragility of the bone. 4 Furthermore, bone marrow density (BMD) increase has been found in patients with OA knee, suggesting a degenerative change in morphology; for example, osteophyte degeneration can lead to improper BMD calculation. Currently, the relationship between OA and BMD remains inconclusive.5-8
One of the factors related to achieving a good outcome in TKA is bone minerals, which are composed of several basic chemicals, such as calcium, vitamin D, and phosphorus. Those component function with hormones, including parathyroid hormone, glucocorticoid, and sex hormones(estrogen and progesterone) to regulate the bone cycle. Imbalance of minerals and hormones could cause bone structure weakening, which can be referred to as metabolic bone disease; thus, patients suspected with this disease should be screened and worked up to receive proper treatment. 9
Some of the metabolic bone diseases that are often found in older patients include osteopenia/osteoporosis, hypocalcemia, and hypovitaminosis D. By definition from the World Health Organization osteopenia is defined by bone densitometry at neck of femur and lumbar spine as a T score −1 to −2.5 and osteoporosis is defined by bone densitometry as a T score below −2.5. 10 Metabolic bone diseases need to be corrected to achieve a better outcome in patients with OA knee regardless the radiographic classification (Kellgren-Lawrence (KL)); however, these conditions are frequently neglected by physicians when treating outpatients with OA knee, 11 which could lead to devastating outcomes after surgery. For example, intraoperative periprosthetic fractures may occur, which may end up requiring more complex surgery along with the use of a bone graft, whether it is an autologous bone graft or a metal-organic framework-based biomaterial bone graft. 12 In this study, we aimed to evaluate the prevalence of common metabolic bone diseases in outpatients with nonoperative OA knee and its correlation with this geriatric disease.
Materials and Methods
The ethics committee of our institute approved our study protocol. We conducted a prospective study on 281 outpatients with OA knee who visited at our hospital between November 2020 and April 2021. The inclusion criteria were OA knee diagnosis, ages of above 55 years for females and above 60 years for males and permanent residence in Bangkok area. Conversely, the exclusion criteria were previous calcium/vitamin D treatment, fragility fracture history, previous spine or hip surgery, metastasis cancer, smoking, steroid use, inflammatory joint disease, bedridden status/inability to walk, and no consent for study participation. We excluded ten patients because of rheumatoid arthritis (3 cases), previous spinal fixation (4 cases) and steroid use (3 cases). Ultimately, 281 patients were eligible for the analysis. (Figure 1). Flow diagram of the present study.
We collected metabolic bone disease–related data, including abnormal dual-energy X-ray absorptiometry scanning that performed at left neck of femur and lumbar spine (abnormal BMD T sore < −1 SD) in. The patient lies beneath the X-ray source of a C-arm, which releases photons at two different energy levels that are unique to soft tissue and cortical bone. In order to evaluate bone mass per unit volume, the attenuations from these high- and low-energy photon emissions are detected above the body and merged to provide a planar image. And the blood test results are indicating serum vitamin D insufficiency (serum 25-hydroxyvitamin D <32 ng/mL), hypocalcemia (calcium <8.6 mg/dl), impaired renal glomerular infiltration rate (GFR <60 mL/min/1.73 m2), hyperparathyroid hormone level (PTH >65 pg/mL), and hyperalkaline phosphatase level (ALP >104 U/L). The relationship between common metabolic bone diseases and OA knee was determined by regression analysis.
Patient’s Demographic Data.

ASA, American Society of Anesthesiologists. Data presented as number (%) mean +/− standard deviation (SD).
Results of Outcome’s Demographic Data.
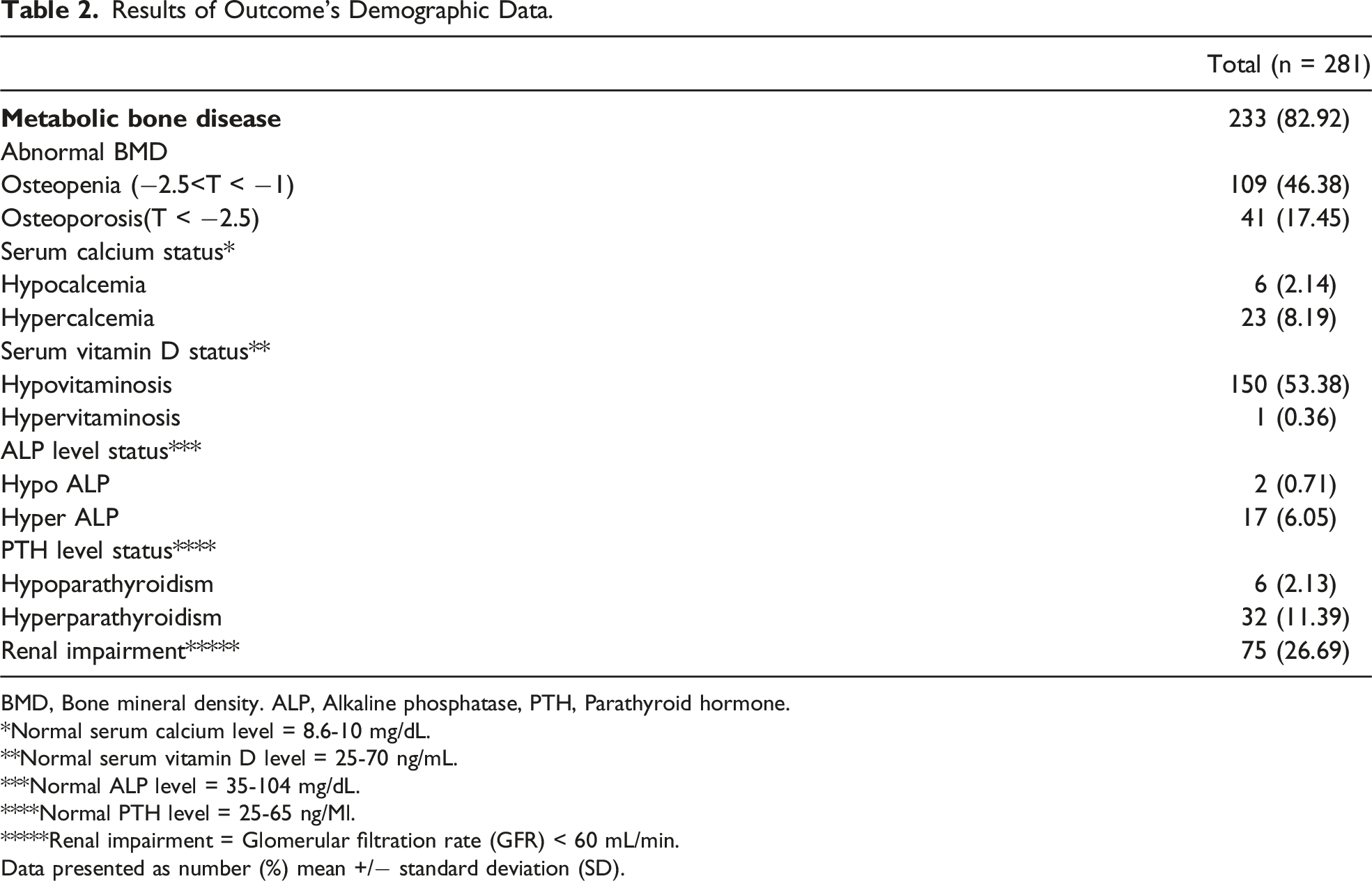
BMD, Bone mineral density. ALP, Alkaline phosphatase, PTH, Parathyroid hormone.
*Normal serum calcium level = 8.6-10 mg/dL.
**Normal serum vitamin D level = 25-70 ng/mL.
***Normal ALP level = 35-104 mg/dL.
****Normal PTH level = 25-65 ng/Ml.
*****Renal impairment = Glomerular filtration rate (GFR) < 60 mL/min.
Data presented as number (%) mean +/− standard deviation (SD).
Statistical Analysis
Results, including the patient characteristics, are expressed as mean ± standard deviation or median and range. Categorical variables were compared using Chi-squared test or Fisher’s exact test. Related factors were determined by logistic regression analysis, and the results are expressed as odds ratios (ORs), 95% confidence intervals (CIs) and P-values. All statistical data were analyzed using STATA version 15 (StataCorp, College Station, TX, USA). A P-value of <0.05 was considered statistically significant.
Results
According to our demographic data study (Tables 1 and 2), most patients were female (82.92%), aged 61-70 years (44.48%) and were presented with Kellgren–Lawrence (KL) grades 3-4 (91.46%). Overall metabolic bone diseases were found in 82.91% of patients (233/281). In particular, vitamin D insufficiency (53.38%, 150/281) was the most prevalent, followed by osteopenia (44.38%, 109/235), impaired renal function (26.69%, 75/281), osteoporosis (17.45%, 41/235), hyperparathyroidism (11.39%, 32/281), hypercalcemia (8.19%, 23/281), and hyperalkaline phosphatase (6.05%, 17/281). Furthermore, the risk for metabolic bone disease were significantly found in patients with hypertension (OR 0.46, 95% CI 0.22-0.91, P = 0.027).
Parameter of Serum Vitamin D Status.

BMI, Body Mass Index. ASA, American Society of Anesthesiologists. Normal serum vitamin D level = 25-70 ng/mL. Data presented as number (%) mean +/− standard deviation (SD). *P < .05 considered statistically significant.
Univariate Regression Analysis of Abnormal Vitamin D Group.

ASA, American Society of Anesthesiologists. Normal serum vitamin D level = 25-70 ng/mL. *P < 0.1 considered statistically significant. CI, Confident Interval.
Multivariate Regression Analysis of Abnormal Vitamin D Group.
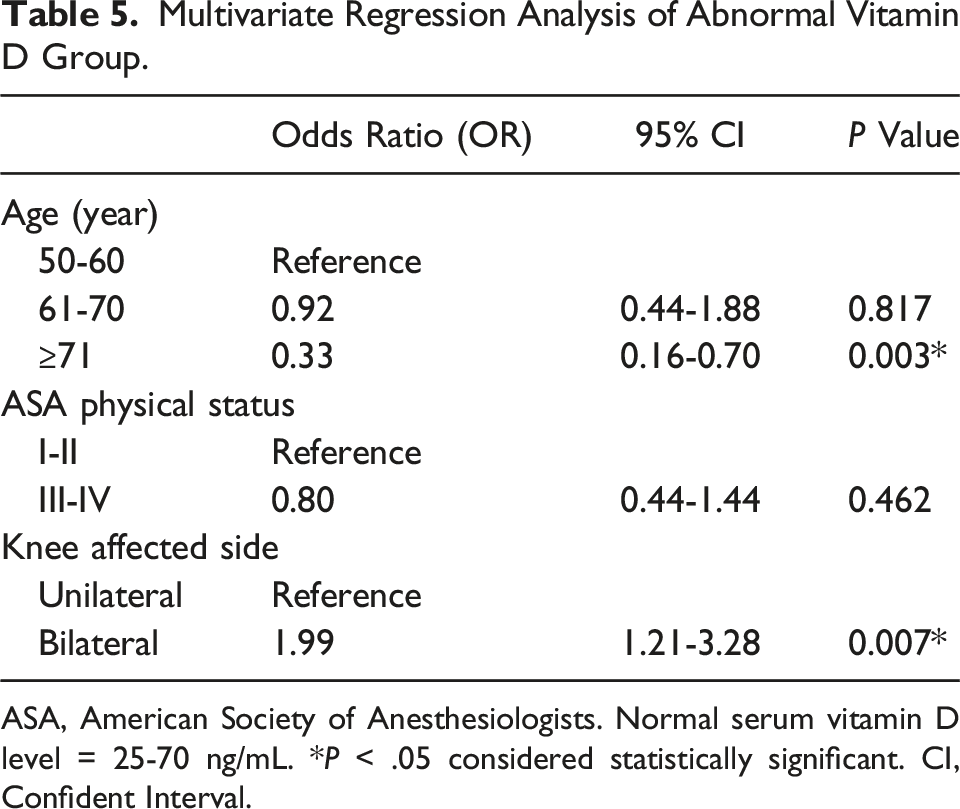
ASA, American Society of Anesthesiologists. Normal serum vitamin D level = 25-70 ng/mL. *P < .05 considered statistically significant. CI, Confident Interval.
Risk Factors of Osteopenia and Osteoporosis Patients.

BMD, Bone Mineral Density. BMI, Body Mass Index. ASA, American Society of Anesthesiologists. Data presented as number (%) mean +/− standard deviation (SD). *P < .05 considered statistically significant.
Univariate Regression Analysis of Osteopenia and Osteoporosis Patients.

BMI, Body Mass Index. *P < 0.1 considered statistically significant. CI, Confident Interval.
Multivariate Regression Analysis of Osteopenia and Osteoporosis Patients.

BMI, Body Mass Index. *P < 0.05 considered statistically significant. CI, Confident Interval.
Discussion
Metabolic bone diseases are the disorders of bone strength usually caused by abnormalities of minerals (eg, calcium or phosphorus), vitamin D, bone mass or bone structure. Many of our patients with OA knee had metabolic bone diseases (82.92%). Our results showed that hypertension was a significant risk factor related to metabolic bone disease, possibly attributed to the fact that hypertension has obtained the highest prevalence (58%) in several populations compared with other chronic diseases. 13 In patients with hypertension, it can lead to kidney damage by causing progressive thickening of the arteries and arterioles within the kidney parenchyma. This occurs as a consequence of a pathogenetic cascade involving atrophy of vascular smooth muscle cells and increased endothelial leakiness. 14 Excessive urinary calcium excretion occurs; consequently, secondary parathyroidism is induced to increase the serum calcium level by releasing calcium from the bone, thereby accelerating osteoporosis. 15
The most common metabolic bone disease found in the OA knee clinic at our hospital was vitamin D insufficiency (53.38%), followed by osteopenia (46.38%), renal impairment (26.69%), and osteoporosis (17.45%). In vitamin D insufficiency, age of ≥71 years and bilateral OA knee were the significant risk factors (Table 6). Older people are prone to vitamin D insufficiency in many ways, such as reduction in cutaneous synthesis and daily exposure to sunlight and various diseases, including chronic renal failure and gastrointestinal malabsorption. Concurrence of bilateral OA knee symptom such as pain could make patients unable to perform regular daily activities efficiently or expose themselves to adequate sunlight, resulting in vitamin D insufficiency later on.16-18 Additionally, there are interesting factors regarding the balance of bacteria in the gut which can further enhance the absorption of vitamin D. 19
Moreover, the risk factors of osteopenia and osteoporosis were age of 71 years or more, BMI above 30 kg/m2, CKD, and the affected left side (Table8). The age factor conforms to the Compendium of Osteoporosis (IOF 2019), which states that bone mass peaks at mid-20s in both sexes and that it gradually declines with age in males and plateaus, followed by an accelerated period of bone loss for several years after the menopause, in females. In 2010 in the US, osteopenia and osteoporosis occurred in 52.2% and 29.74% of females and 45.83% and 7.1% in males, both at the age of ≥71 years. 20 Regarding BMI, patients with obesity are at risk for osteopenia and osteoporosis as a result of several mechanisms, including increased adipocyte differentiation and fat accumulation, decreased osteoblast differentiation and bone formation, and increased osteoclast activity and bone resorption, which are the consequences of abnormalities in hormones (leptin, estrogen, and adiponectin) and cytokines (tumor necrosis factor-α and interleukin-6).21,22 CKD also has an important negative impact on bone health; in fact, this condition is termed by the Kidney Disease Improving Global Outcome as chronic kidney disease–mineral and bone disorder (CKD-MBD). Patients with OA knee accompanied with CKD stages 3a–5D have low BMD and reduced mechanical strength, leading to a strikingly elevated risk of fractures (1.5- to twofold higher than in the general population).23-27 Normally, we assess BMD at the left neck of the femur to minimize time, medical costs, and radiation exposure associated with radiography. 28 Measuring at the nondominant hip is preferred on the basis of the assumption that the nondominant side is less physically active and thereby exposed to less stress and impact, resulting in lower BMD. 24 Many studies confirmed the relationship between lower BMD and ipsilateral OA knee. For instance, Anand et al showed that the mean BMD in the ipsilateral neck femur of patients with OA knee at grades 1, 2, 3, and 4 was 0.95 ± 0.13, 0.92 ± 0.17, 0.75 ± 0.17, and 0.49 ± 0.07 g/cm2, respectively, indicating a progressive decline, which showed a P-value of <0.0001.29-33
Limitation
This study has several limitations. First, owing to the coronavirus 2019 pandemic policy of reducing the congestion of patients in each hospital department, the number of patients that could apply for BMD testing was only 236 out of 281 patients, accounting for 84% of the overall population. Second, we had no control group (patients without OA) to compare with to strongly identify the relationship of the factors with OA of the knee. Third, the activity level and home diet could not be accurately evaluated and standardized because of the individualization among patients. Further analysis is necessary to establish solid evidence in the comparison of risk factors between the OA and non-OA groups.
Conclusions
Metabolic bone diseases were commonly found in most of the patients with OA knee, and vitamin D insufficiency, osteoporosis, and osteopenia conditions were mainly identified. These preventable conditions have risk factors that are mostly correctable, for example gain more outdoor activities, consume vitamin D supplement or start osteoporosis treatment program. Given that these conditions can affect bone strength, they should be given attention to avoid yielding a negative impact on the treatment outcome of patients with OA knee.
Footnotes
Acknowledgements
The authors are deeply grateful to all members of the Department of Orthopedics of Vajira Hospital, Navamindradhiraj University, Vajira research unit for all co-operation, assistance, data collection, statistical analysis and funding in this study. We would also like to thank Satit Thiengwittayaporn, Asso Prof. And Natthapong Hongku. MD. for suggestions and the new point of view and method in conducting this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research Facilitation Division, Faculty of Medicine Vajira Hospital, Navamindhradhiraj University.