
Abstract
Introduction
Although the overall quality of medicine has improved in recent decades, the functional capacity in many hip fracture patients remains insufficient. The goal of the present study was to identify significant predictors of Instrumental Activities of Daily Living (IADL) measured by the Lawton-Brody scale at 3- and 6-month follow-up in patients with hip fractures admitted to a hospital.
Methods
This observational cohort study included 191 patients with acute hip fractures. IADL was measured at baseline and after 3 and 6 months using the Lawton-Brody scale. Multivariable logistic regression analysis was carried out using pre-fracture functional status, sociodemographic variables, hand grip strength (HGS), surgical procedure, complications, and length of hospital stay, Short Physical Performance Battery, and Barthel Index (BI) on the fifth postoperative day as potential predictors for IADL after a hip fracture surgery.
Results
The mean age of the participants was 80.3 ± 6.8 years, and 77.0% of our cohort were women. Multivariate regression analysis revealed that pre-fracture functional status and early functional recovery were independent predictors of IADL after hip fracture surgery.
Conclusions
Clinicians should take steps to improve functional outcomes by changing how patients are rehabilitated in the first days after hip fracture surgery, especially for the group of patients with a lower functional status before the fracture.
Keywords
Introduction
Hip fracture is a severe complication of falls and osteoporosis in older adults, and can be fatal for older people, resulting in impaired function, increased morbidity, dependence, institutionalization, and mortality. The impact of hip fractures on the health care system is especially significant because of the ageing population worldwide. 1 There were 1.6 million hip fractures in the year 2000, and this number is expected to increase to 4.5-6.3 million by 2050. 2
Regardless of improvements in surgical procedures and post-acute care, outcomes of hip fracture patients often remain unsatisfactory. 3 Hip fractures are followed by a significant decline in functional capacity for both the basic and instrumental activities of daily living, 4 and according to published data about 40% of patients are discharged directly to long-term care facilities or nursing homes rather than their pre-fracture place of residence. 5 Between 20% and 60% of patients who were independent in self-care activities, such as washing and dressing before the fracture require assistance to do these tasks after 1 year. 1
Various scoring systems are available for assessing the functional outcome after hip fracture, where Barthel Index (BI) and Lawton-Brody scale are most commonly used and considered the most comprehensive.6-8 The BI assesses the level of autonomy and independence and focuses on the basic Activities of Daily Living (ADL), such as mobility function, continence, and self-care. 9 However, ADL assessment has a floor effect, as it is insensitive to variations in low levels of disability and minor disability frequently does not translate into the limitations in the basic ADL. 10 On the other hand, the Lawton-Brody scale is more specific, assesses the more complex Instrumental Activities of Daily Living (IADL) necessary for living in the community, demands a greater ability to make decisions and solve everyday problems, and has been used extensively.11,12 Previous research has shown that IADL can be more complex and valuable in assessing patients’ well-being compared to basic ADL. 11
Multiple factors affect the functional outcome of patients with hip fractures. 13 Various predictors of functional outcomes in hip fracture patients were identified in the literature.7,14-22 It is well known that age, comorbidity, functionality, and cognition were factors for which most studies indicated a significant effect.7,22-24 New quality research suggested hand grip strength (HGS) as a relatively new predictor of functional outcome after hip fracture.14,15 Moreover, there are only a few studies that showed the predictive value of intrahospital recovery in relation to later functional outcome after hip fracture surgery.21,25 However, none of these articles used the Lawton-Brody scale as a measure of the functional outcome.14-21 There is a lack of studies examining predictors of IADL measured by the Lawton-Brody scale, despite its potential advantage in assessing a wide range of daily life skills. Additionally, impairments and limitations in IADL performance can serve as early indicators of decline in ADL function and independent living.11,12 This emphasizes the importance of using this scale as well as knowing its predictors, to provide timely support to older people through intervention on these variable predictors. 11
The current study aims to identify predictors of IADL measured by Lawton Brody scale 3 and 6 months after hip fracture surgery.
Materials and Methods
Study Design
This prospective, observational cohort study included hip fracture patients over 64 years of age who were admitted to the University-associated orthopedic hospital in Belgrade, Serbia, between March 2017 and February 2018. Exclusion criteria were: pathologic fractures, major concomitant injuries, multiple traumas, malignant diseases, inability to walk before fracture, and nonoperative treatment resulting from high surgical risk. Patients with severe cognitive impairment or hand weakness as a consequence of previous neurologic disorders or hand injuries were also excluded.
In total, 551 patients with hip fracture were examined for eligibility, and 191 patients were eligible and included in this study. All patients gave written informed consent to participate in the study.
Authors followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines when preparing the manuscript. The STROBE checklist is available as Supplemental Material 1.
Baseline Evaluation
First, all subjects were evaluated through standardized patient interviews regarding sociodemographic variables (age, sex, marital status, pre-injury living conditions, and level of education). In addition, we recorded comorbidity and cognitive level, body mass index (BMI), pre-fracture functional status, health-related quality of life, presence of anemia and delirium on admission, and examined HGS within 24h of admission. We also recorded perioperative variables during the primary hospital stay, such as waiting time for surgery, surgical method, type and duration of anesthesia, presence of postoperative complications, and length of stay (LOS). Also, early recovery was assessed on the fifth day after surgery.
We used the Charlson comorbidity index (CCI) to categorize comorbidities 26 and divided the patients into 3 groups: without and mild, with CCI scores of 1-2; moderate, with CCI scores of 3-4; and severe, with CCI scores ≥5. The cognitive level was assessed with the Short Portable Mental Status Questionnaire (SPMSQ). 27 The 10-item questionnaire classifies the patient’s cognitive level depending on the number of correct answers as lucid (8-10), mild to moderate cognitive dysfunction (3-7), and severe cognitive dysfunction (0-2).
We evaluated the pre-fracture functional status using the Lawton-Brody scale which refers to 2 weeks before the injury, based on the patient’s memory. The Lawton-Brody scale evaluates IADL across 8 domains: using the telephone, shopping, food preparation, housekeeping, laundry, transportation, medication, and finances. Competence is rated according to descriptions of the person’s level of involvement/ability in each activity. The scale assigns a score from 0 to 8; the highest score indicates the best functional capability. 28 Patients were divided into 2 cohorts according to the median value of the Lawton-Brody scale, where values from 0 to 5 were considered low functioning, and values from 6 to 8 were considered high functioning.
General health-related quality of life was measured with the EQ5D scale, which consists of a five-level response for 5 domains related to daily activities, mobility, self-care, usual activities, pain and discomfort, anxiety, and depression. 29 Responses to the health status classification system are converted into an overall score using a published utility algorithm for the UK population. 30 We divided the participants into 2 groups (with or without anemia), depending on hemoglobin levels and based on the recommendations of the World Health Organization. 31 The presence of delirium was examined by the Confusion Assessment Method (CAM). 32
HGS was measured using a JAMAR hand dynamometer (Model BK-7498, Fed Sammons Inc, Brookfield, III). Handle position 2 was used for measuring HGS. This has been assumed to be the most reliable and consistent position and is the position advocated for routine use. 33 Patients were in the supine position and encouraged to exhibit the greatest possible force. 34 The best recorded of 3 attempts of maximal voluntary contraction performed at 1-minute intervals of the dominant hand was considered for analysis. HGS measurements less than 16 kg in women and 27 kg in men were considered cut-points for the diagnosis of sarcopenia according to the revised EWGSOP2 criteria. 35
We assessed the early recovery of patients on the fifth day after surgery. The Barthel index measured performance in basic activities of daily living; its score ranged from 0 (total dependence) to 100 (total independence). 9 We also used the Short Physical Performance Battery (SPPB) to assess in-hospital mobility. This is a widely used scale exploring the reduction of physical performance in older people, particularly muscle strength of lower extremities, during a standing balance test, a walk test, and a chair sit-stand test. Total SPPB scores (range, 0-12) were calculated by summing up the 3 individual scores, each ranging from 0 (unable to complete the test) to 4. 36
In all patients early assisted ambulation was encouraged on the first postoperative day with weight-bearing as tolerated, and all patients followed a standardized postoperative rehabilitation program.
Outcomes
Functional status after 3 and 6 months were evaluated using the Lawton-Brody scale. The information was collected by phone interview. Data from patients who died or were lost before the first and second follow-up were excluded from the study. For the analysis of the Lawton-Brody scale 3 months postoperatively, the sample size included 160 patients (22 (11.5%) died, 9 (4.7%) were lost to follow-up). Analysis of outcomes 6 months after the fracture was performed on 154 patients (27 (14.1%) died, 10 (5.3%) were lost to follow-up). Figure 1 summarizes the flow of patients during the period of this investigation. The flow of patients during the period of the investigation.
Statistical Analysis
Continuous variables are presented in terms of mean values with SD or median and interquartile range depending on the Kolmogorov-Smirnov test of distribution normality. Categorical values are summarized as absolute frequencies and percentages. To compare patients with 2 different categories of functioning a t-test was performed for the continuous variables and a Chi-square test for nominal variables.
To detect potential and independent predictors of recovery expressed as Lawton-Brody scale after 3 and 6 months, univariate and then multivariate linear regression with collinearity diagnostic (VIF method used; variables with VIF >4 were excluded from multivariate models) was used. Both multivariate models were adjusted for age and gender.
Friedman and Wilcoxon signed-rank tests were used to compare numerical outcomes with normal distribution at several time points.
The significance level for all statistical tests was set at .05. All analyses were performed using the SPSS Inc. Released in 2008. SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc.
Results
Socio-Demographic and Baseline Pre- and Perioperative Characteristics of the Participants.

aValues are given as the mean with the standard deviation.
bValues are given as the number of patients with the percentage in parentheses. CCI - Charlson Comorbidity Index; SPMSQ - Short Portable Mental Status Questionnaire; BMI - body mass index; HGS - handgrip strength; SPPB - Short Physical Performance Battery.
The average value of the Lawton-Brody scale for IADL 2 weeks before the hip fracture in our patients was 6. At 3 months, the average value of the Lawton-Brody scale was 3, and after 6 months, the average value of this scale was 5. IADL decreased significantly (P < .01) between preoperative and 3-month follow-up and increased significantly (P < .01) between 3- and 6-month follow-up. IADL did not return to pre-injury levels. Figure 2 shows the course of IADL measured by the Lawton-Brody scale. Course of IADL measured by the Lawton-Brody scale.
Univariate and Multivariate Analysis of Variables Associated With Lawton IADL 3 months After Fracture.

Adjusted for age and gender. CCI - Charlson Comorbidity Index; SPMSQ - Short Portable Mental Status Questionnaire; BMI - body mass index; IADL - Instrumental activities of daily living; HGS - handgrip strength; SPPB - Short Physical Performance Battery.
Univariate and Multivariate Analysis for Variables Significantly Associated With Lawton IADL 6 months After Fracture.
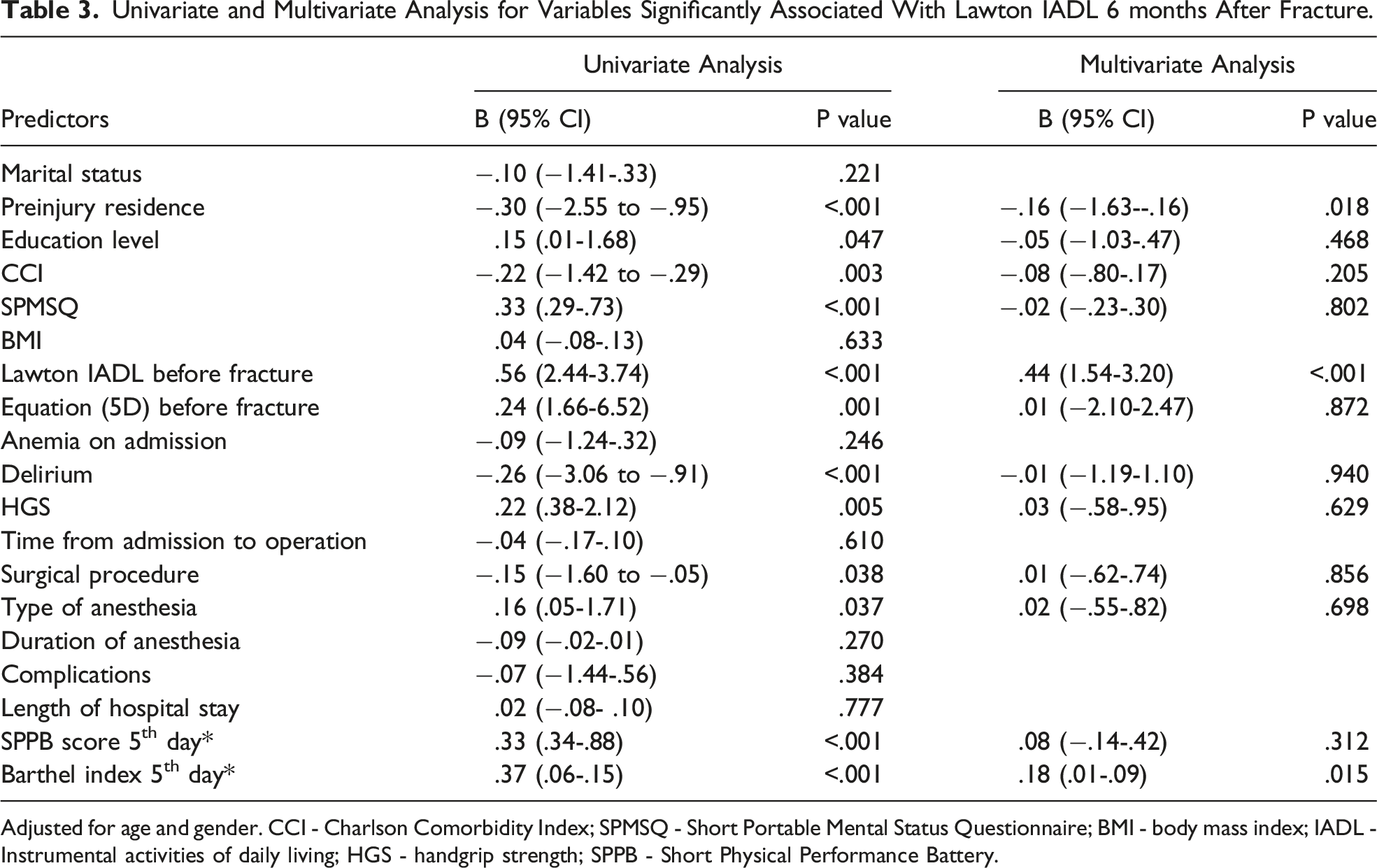
Adjusted for age and gender. CCI - Charlson Comorbidity Index; SPMSQ - Short Portable Mental Status Questionnaire; BMI - body mass index; IADL - Instrumental activities of daily living; HGS - handgrip strength; SPPB - Short Physical Performance Battery.
Adjusted multivariate regression analysis revealed that only pre-fracture functional status (Lawton-Brody IADL scale) and early functional recovery (BI on the fifth postoperative day) were independent predictors of IADL at 3 and 6 months after hip fracture for both genders and in all age groups. This means that patients with low Lawton-Brody scale score pre-fracture, as well as patients with lower BI values on the fifth postoperative day, achieved statistically significant lower Lawton-Brody scale values 3 and 6 months after hip fracture surgery. Also, HGS was at the border of statistical significance for IADL 6 in the first step in the logistic regression, but the significance was lost in the multivariate model.
Discussion
Our study included 147 women and 44 men over 65 who underwent surgical treatment after a hip fracture at the University orthopedic hospital in Serbia. It showed that hip fracture patients with a low pre-fracture Lawton-Brody scale and patients with a lower BI on the fifth postoperative day were significantly less independent regarding IADL after 3- and 6-month post-surgery. Furthermore, our findings provide evidence that pre-injury functional status and early functional recovery are strong, consistent, and independent predictors of medium- and long-term functional outcome of patients with hip fracture.
The results of our investigation are consistent with data from previous studies confirming pre-fracture functional status as the most significant determinant of function at follow-up.13,23,24,37-49 It strongly supports the fact that patients who are more physically active before the fracture may have less difficulty regaining function. Therefore, efforts to prevent functional decline in older people at elevated risk of hip fractures through physical activity and adequate nutrition should be increased. 50
Early functional recovery in our study, measured by BI on the fifth postoperative day, also showed a significant predictive role of later functional outcome. To our knowledge, there is little data in the available literature on the predictive value of early functional recovery after hip fracture surgery relative to later functional outcomes.21,25 Beloosesky et al found that FIM score 1-week post-op, combined with upper limb functioning and age, can predict motor functioning 6 months post-fracture measured by Functional Independence Measure (FIM). 21 Ingemarsson et al showed that the Timed Up and Go Test (TUG) balance test 7 days after hip fracture surgery, combined with the level of independence and frequency of walking outdoors before the fracture, was a strong predictor for both the walking ability and activity level 1 year after hip fracture. 25 Definition of walking and activity level as outcome variables were constructed in their study, based on clinical experience and the literature, 25 unlike our study, which used the Lawton-Brody scale as a standardized measure of functional outcome. Given the above, early functional recovery should be imperative, and emphasis should be placed on early postoperative rehabilitation. Accordingly, Dyer et al assumed that the key focus of rehabilitation should include early mobilization and functional exercises with higher doses of mobility training. 51
A recent systematic review by Xu et al. identified HGS as a relatively new predictor of poor functional outcomes in hip fracture patients. 14 HGS is recommended as a measure of choice for assessing overall muscle strength for diagnosing sarcopenia and frailty. 52 Our investigation also showed HGS at the border of statistical significance for IADL 6 in the first step in the logistic regression, but the significance was lost in the multivariate model. Many recent studies reported a significant predictive value of HGS concerning later functional status, but they were methodologically different from our investigation.16,17,20 Thingstad et al. used gait speed as a functional outcome. 16 Di Monaco et al measured HGS in the post-acute rehabilitation setting and used BI as an outcome measure assessed both on discharge and at the 6-month follow-up, reporting their results only on women. 17 Both studies analyzed handgrip strength as a continuous variable, while our study used cutoff points to define clinically relevant weakness based on HGS according to the EWGSOP2 criteria. 35 Also, previous research by Selakovic et al. indicated that HGS and several other prognostic factors could independently predict short- and long-term ADL. 20 We believe a more complex interaction between HGS and BI on the fifth postoperative day influences Lawton-Brody scale 3- and 6-month post fracture, while the Lawton-Brody scale pre-fracture serves as a ceiling for recovery measured by this scale, but this theory should be further investigated. Certainly, in older patients with hip fractures, early HGS evaluation might provide important prognostic information regarding the patient’s future functional trajectory. 18
Interestingly, the Short Physical Performance Battery (SPPB, see Tables 2 and 3) test as a second indicator of the functionality on the fifth postoperative day did not show significant predictive value relative to later functional status in our study, although previous studies have shown that SPPB score could predict mobility-disability, nursing home, and hospital admission.53,54
Differences in proven predictors of functional outcomes between mentioned studies (16, 24, 25, 36-49), including our research, may be explained by choosing patients with different preinjury characteristics (functionality levels and comorbidity) and by the diversity of variables considered potential predictors. Populations of these studies were heterogeneous, and there was also considerable diversity regarding the assessment used to rate functional outcomes. The most prevalent functional assessments used in these studies were FIM,39,41,42,44,46,48 BI with various modifications,37,40,47,49 and Katz ADL.24,38,42 Only a small number of these studies have used the Lawton-Brody scale assessing functional outcome after hip fracture, as in our study.24,37,45 Lin et al listed the ability to do housework, marital status, and use of a walking aid before fracturing as predictors of IADL 1 year after fracture. 45 Ganczak et al. reported that pre-fracture IADL, besides age and intellectual functioning, was a predictor of return to a pre-fracture IADL score at 3 and 6 months after hip fracture surgery. 24 However, only Gonzales-Zabaleta et al confirmed the predictive value of the Lawton-Brody scale before the fracture in the Lawton-Brody IADL prediction 90 days after the fracture, 37 which is similar to our result. This indicates that the Lawton-Brody scale may be, in many cases, more useful in assessing functional recovery than scales that assess other aspects of functional recovery (including ADL), although there is a lack of studies in the available literature that examined the prediction of IADL after hip fractures.24,37,45 IADL function is usually lost before ADL in older adults, and assessment of IADL may identify incipient physical and cognitive decline in people who might otherwise appear capable and healthy. 55 Further, people are social beings, and they are not only interested in performing basic activities of daily living, but also in interacting with other people.
There are several strengths of our study. First, to the best of our knowledge, this is the first study to assess early postoperative BI in predicting Lawton-Brody IADL in patients 3 and 6 months after hip fracture surgery. Second, our study proves mentioned prognostic value in the acute setting for both gender and all ages. Our results have some clear clinical implications. First, there is a great need to identify hip fracture patients at increased risk for a worse outcome. By identifying predictors of poor functional outcomes after hip fracture surgery, health care providers can establish preventive measures and tailor an individualized treatment plan to improve functional outcomes. Clinicians also can adopt a stratified care approach by prioritizing those at substantial risk of poor functional outcomes for more intensive rehabilitation. 6
Study Limitations
There are also some limitations to our study. First, the outcome of our study was assessed with only self-reported information collected by phone interviews. This may lead either to overestimating or underestimating the ability to perform the activity. Second, the pre-fracture functionality scale is based on memory, so reliability is questionable, although the results show consistent association between the pre- and post-fracture scores. Patients were collected only from 1 single center, and almost 20% of patients were lost to follow up, while other confounding factors, such as nutritional and vitamin D status, should also be studied in the future. Also, 1 of the significant limitations of this study could be the high exclusion rate due to the exclusion criteria.
Conclusions
In this study, we showed that preoperative IADL and early functional recovery measured with BI play the crucial role in predicting IADL after hip fracture, but also HGS probably plays a role. All these facts can help us in planning rehabilitation, but also harmonize the expectations of patients and their families with the realistic goals of rehabilitation. Clinicians should take steps to improve functional outcomes by changing how patients are assessed and rehabilitated in the first days after hip fracture surgery, especially for patients with a lower functional status before the fracture. Uncertainty about the most effective rehabilitation may also be due to a limited understanding of the nature of prognostic factors, and future studies should investigate the relationships between prognostic factors and their interaction.
Supplemental Material
Supplemental Material - Pre-Fracture Functional Status and Early Functional Recovery are Significant Predictors of Instrumental Activities of Daily Living After Hip Fracture: A Prospective Cohort Study
Supplemental Material for Pre-Fracture Functional Status and Early Functional Recovery are Significant Predictors of Instrumental Activities of Daily Living After Hip Fracture: A Prospective Cohort Study by Ivan Selaković, Stefan Mandić-Rajčević, Anđela Milovanović, Sanja Tomanović-Vujadinović, Sanja Dimitrijević, Milica Aleksić, and Emilija Dubljanin-Raspopović in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partially funded by the support of the Faculty of Medicine University of Belgrade, Project Contract Number 451-03-47/2023-01/200110. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.