
Abstract
Enhanced recovery is now a standard model of care in most UK elective surgical units. For hip and knee arthroplasty this approach typically includes opioid-sparing anesthesia (OSA), local infiltration analgesia (LIA), and day of surgery mobilization. There is evidence that these interventions shorten hospital stay and improve outcomes, without increasing complications or readmissions. These interventions may also benefit patients undergoing surgery for femoral neck (hip) fractures. This group of patients are frail and elderly, and are at high risk from surgery, anesthesia, and opioid and bed rest-related complications. Hip fractures are also a major public health concern. They are common, expensive to treat, and associated with poor outcomes. Despite this there are no published descriptions of the use of OSA and LIA to enable day of surgery mobilization in patients with hip fractures. We present 3 patients who underwent hip fracture surgery according to an enhanced recovery protocol that incorporated all 3 interventions. In each case day of surgery mobilization was achieved safely and comfortably, without requirement for strong opioids postoperatively. The cases demonstrate that these interventions can be well tolerated by patients with hip fracture, including those with impaired mobility or cognitive function. The protocol is compatible with all common operations for hip fracture, and with spinal or general anesthesia. It is inexpensive and requires minimal expertise. It may have the potential to improve care and shorten hospital stay, while reducing cost. Further investigation is required.
Keywords
Introduction
Enhanced recovery is a perioperative management approach which aims to improve outcomes by reducing the physiological impact of surgery. Specifically, it aims to minimize pain, opioid requirement, and the duration of fasting and bed rest. 1 In accordance with the Department of Health recommendations for elective surgery, it is now a standard model of care in most UK health care trusts. 1,2 There is increasing evidence that it reduces hospital stay and improves patient satisfaction, without an increase in complications or readmissions. 3 –5
Enhanced recovery protocols for elective hip and knee arthroplasty typically include opioid-sparing anesthesia (OSA), local infiltration analgesia (LIA), and mobilization from the day of surgery. 3,6 OSA is the anesthetic practice of minimizing opioid side effects, using short-acting preparations such as fentanyl and/or nonopioids such as pregabalin, ketamine, and magnesium sulfate. LIA is the infiltration of large volume, dilute local anesthetic with adrenaline into the surgical wound intraoperatively, with the aim of providing prolonged analgesia. Unlike regional nerve blockade, LIA does not cause clinically relevant motor nerve inhibition, and therefore should not delay mobilization. In contrast to strong opioids, it provides highly effective analgesia on movement. 7
Opioid-sparing anesthesia , LIA, and day of surgery mobilization may also address many of the problems faced by patients with femoral neck (hip) fracture. These patients have an average age of 81, a median American Society of Anesthesiologists (ASA) grade of 3, and are confined to bed by their injury preoperatively. 8,9 Their risk of complications is higher than that of elective arthroplasty patients, who are typically younger, fitter, and have the additional benefit of being mobile preoperatively.
Despite these considerations, there are no published descriptions of these interventions in combination for hip fracture. This may relate to the prevailing orthopedic view that day of surgery mobilization would not usually be tolerated by these patients. Current standard practice for hip fracture care, consistent with national guidelines, includes strong opioids as the mainstay of analgesia, conventional spinal or general anesthesia with or without regional nerve blockade, and mobilization on the day after surgery. 10
The purpose of this report is to demonstrate that OSA and LIA can enable day of surgery mobilization in a comfortable and well-tolerated manner, despite the frailty and advanced age of patients with hip fracture. It also demonstrates that these interventions may make postoperative strong opioids unnecessary.
This is of particular interest because hip fractures constitute a major public health burden, which may be alleviated by enhanced recovery interventions. They are the commonest fractures requiring admission to UK hospitals, expensive to manage, and associated with poor outcomes. 9,11 More than 60 000 patients were treated in 2012, 97% by operation, and at a cost of £1.5 billion. 12 Mortality at 30 days is 8.2%, and rises to 30% at 1 year. 9 –12
We present 3 patients managed with a hip fracture enhanced recovery protocol, which was designed jointly by orthopedic surgeons and anesthetists, and includes OSA, LIA and day of surgery mobilization (Figures 1 and 2). As the cases demonstrate, it is applicable to all patients with hip fracture, including those with dementia and compromised mobility. It is compatible with all standard hip fracture operations, and with general or spinal anesthesia.

Ward protocol.

Theater protocol.
Case Presentations
Case 1
An 84-year-old lady presented with a displaced intracapsular hip fracture after a fall. She had previously been independently mobile without aids, fully self-caring, and lived with her granddaughter. She had asthma, hypertension, hypothyroidism and bilateral knee osteoarthritis. She was assessed as ASA grade 3.
For analgesia (Table 1) she received 10 mg intravenous (IV) morphine on route to A + E. Following her x-ray a fascia iliaca compartment block (FICB) was performed with 30 mL of levobupivacaine 0.25%, using the “double pop” technique. 13 She received 1 dose of oramorph 10 mg preoperatively, and paracetamol and tramadol 4 times a day throughout her stay.
Case 1 Analgesic Summary.
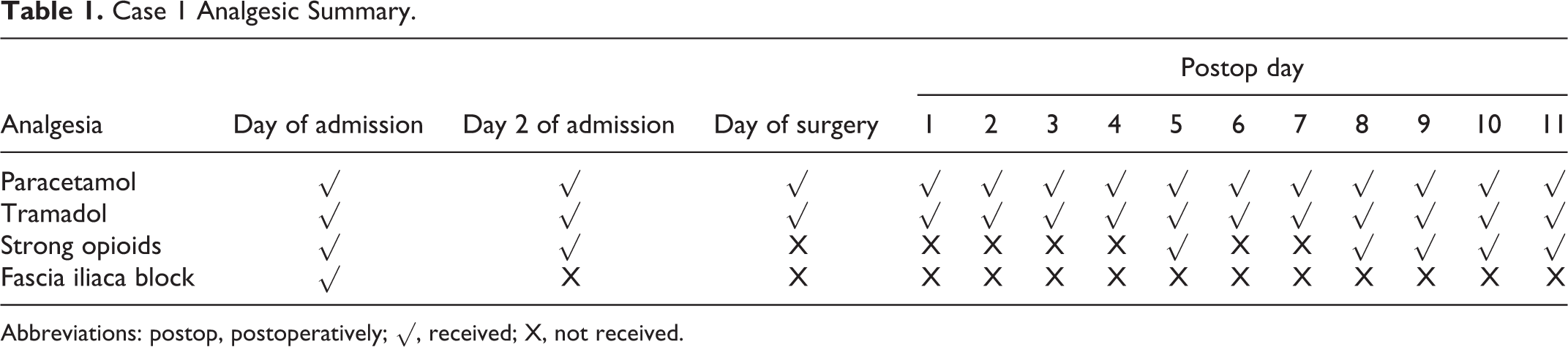
Abbreviations: postop, postoperatively; √, received; X, not received.
For the first 36 hours of her admission she was treated with IV fluid and antibiotics for a urinary tract infection with an associated persistent pyrexia.
She then underwent cemented bipolar hemiarthroplasty under a spinal anesthetic with 2 mL heavy marcaine. Intraoperatively she received midazolam 2 mg, and metaraminol 1 mg. During wound closure a 100-mL LIA mixture of levobupivacaine and adrenaline was injected into each layer, over approximately 2 minutes. The safe LIA dose was calculated according to patient’s weight (see protocol Figure 2).
Three hours post return to the ward she was alert and comfortable, with negligible pain on active hip flexion and no residual motor weakness. She was mobilized fully weight bearing to the end of her bed with a walking frame under nurse supervision, and sat in her bedside chair.
On postoperative day 1 she mobilized 20 m with a walking frame, and progressed to 25 m with crutches by day 4. On day 5 she complained of increased hip pain for which she received oramorph 10 mg. This dose was repeated on 4 occasions. She nevertheless remained mobile with crutches, and repeat x-ray showed no abnormality.
On day 6 she was discharged from physiotherapy, having passed the stairs assessment. On day 11 she was discharged home with temporary social care, which was discontinued as planned at 6 weeks.
Case 2
An 88-year-old man presented with a valgus-impacted intracapsular hip fracture after a fall at his residential home. He had insulin-controlled type 2 diabetes, ischemic heart disease, warfarinized atrial fibrillation, chronic renal impairment, dementia, coronary artery bypass grafting, and a permanent pacemaker. Previously he had mobilized with 1 stick. He was assessed as ASA grade 3.
For analgesia (Table 2) he received 3 mg IV morphine on route to A + E. He was prescribed paracetamol 1 g 4 times a day on arrival, and codeine 30 to 60 mg 4 times a day on postoperative day 2. He received both as prescribed until discharge.
Case 2 Analgesic Summary.

Abbreviations: postop, postoperatively; √, received; X, not received.
aIntraoperative fentanyl 50 μg × 1 dose.
The next day he underwent cannulated screw fixation under a sevoflurane general anesthetic. Intraoperatively he received ketamine 15 mg, fentanyl 50 μg, midazolam 1 mg, magnesium sulfate 5 mg in 50 mL at 25 mL/h, ondansetron 4 mg, dexamethasone 8 mg, tranexamic acid 1 g, metaraminol 0.5 mg, and LIA.
At 3 hours postreturn to the ward he was alert and comfortable, with no pain on active hip flexion. He was mobilized fully weight bearing to the end of his bed with a walking frame under nurse supervision, and sat in his bedside chair.
The next day he was transferred to his chair with a standing hoist, but was not mobilized because of an episode of hypotension of 76/40, which resolved over the subsequent hour. His creatinine rose to 163 μmol/L from 126 preoperatively, but improved to 130 before discharge.
On day 2 he mobilized 10 m with a walking frame under supervision, and progressed to 30 m by day 4. He was discharged to his residential home on day 7 postoperatively, and had regained his preinjury mobility function at 1 month.
Case 3
A 72-year-old lady presented with an intertrochanteric hip fracture after a fall. She had been independently mobile without aids, and lived with her husband in a private house. She had tablet-controlled type 2 diabetes, angina, and left knee osteoarthritis. She was assessed as ASA grade 4.
For analgesia (Table 3) she received 5 mg IV morphine on route to A + E, and a “double pop” FICB with 30 mL of levobupivacaine 0.25% after x-ray. She received 3 doses of oramorph 10 mg preoperatively, 5 doses of tramadol 100 mg postoperatively, and paracetamol 1 g 4 times a day throughout her stay.
Case 3 Analgesic Summary.
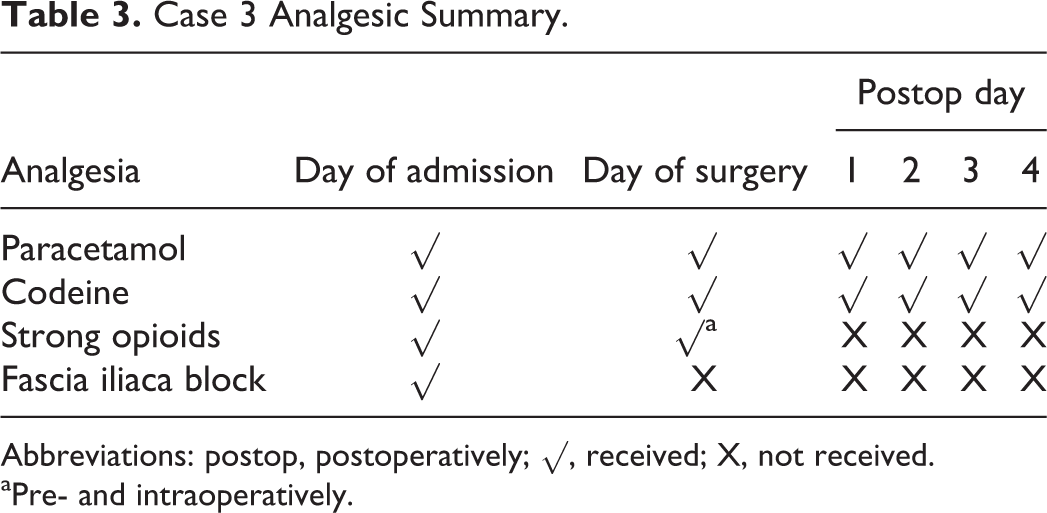
Abbreviations: postop, postoperatively; √, received; X, not received.
aPre- and intraoperatively.
The day after her admission she underwent dynamic hip screw fixation under a sevoflurane general anesthetic. Intraoperatively she received propofol 100 mg, fentanyl 100 μg, ketamine 30 mg, diclofenac 75 mg, paracetamol 1 g, ondansetron 8 mg, tranexamic acid 1 g, and LIA.
Three hours postreturn to the ward she was alert and comfortable, and able to actively flex her hip without pain. She was keen to use the bathroom rather than a commode, and at her own request mobilized the extra 5 m beyond the end of her bed and back under nurse supervision. She tolerated this comfortably, and then sat in her chair.
The next day she mobilized 10 m with a walking frame under supervision. Her hemoglobin was 8.5g/dL, from 9.2 preoperatively. This was treated with a 2-unit blood transfusion because of her ischemic heart disease.
She was mobilized by the nurses over the weekend on days 2 and 3, and was discharged home on day 4, having been assessed by the physiotherapists as independently mobile with a walking frame.
Complications
None of the patients experienced complications in addition to those described. There was no postoperative nausea or vomiting. There were no metalwork, wound or respiratory complications, episodes of cognitive deterioration, venous thromboemboli, pressure sores, or falls. None required urinary catheterization. Discharge in each case was earlier than the previous average acute length of stay at our institution of 20.4 days, by 7, 12 and 15 days respectively. At the time of writing, more than 4 months postoperatively, all are independently mobile and living in their preinjury residences. None have been readmitted to hospital.
These cases are representative of our experience. Patients are more alert, less nauseated, and have more effective and prolonged analgesia on movement than those treated with a conventional anesthetic, even where this includes a regional nerve block. Although strong opioids are prescribed PRN to all patients, they are infrequently required. Patients do appear to benefit from weak opioids such as codeine and tramadol, which can commonly cause opioid side effects. In our experience requirements for these are much reduced however, as are associated side effects.
Discussion
There have been few studies of enhanced recovery principles applied to hip fractures. The case–control study by Macfie assessed the impact of an FICB, early anesthetic assessment, carbohydrate loading, minimized preoperative fasting, and (unspecified) early mobilization following hip fracture, but did not use OSA or LIA. It demonstrated a nonsignificant reduction in complications, with no improvement in length of stay or mortality. 14 A randomized control trial by Oldmeadow compared outcomes after early (1-2 days) and late (3-4 days) mobilization following hip fracture surgery. Early mobilization was associated with a significant improvement in walking distance and transfer independence at 7 days, and nonsignificant improvements in length of stay, and direct discharge home. 15
The combination of LIA and day of surgery mobilization has shown convincing benefit in elective hip and knee arthroplasty. A case–control study of LIA with postoperative top-ups and day of surgery mobilization by Malviya demonstrated significantly improved mortality, and length of stay, with a nonsignificant reduction in complications. 3 A case series of LIA with top-ups and day of surgery mobilization by Kerr achieved low pain scores despite minimal use of strong opioids, and achieved discharge within 2 overnight stays in over 75% of the cases. 7 A randomized control trial by Larsen used day of surgery mobilization without LIA, and demonstrated significantly improved length of stay and quality of life at 3 months. 16
The potential advantages of effective analgesia without strong opioids are numerous. Patients are more likely to avoid cognitive deterioration, maintain a satisfactory oral intake, comply competently with physiotherapy, and be at less risk of falls. Mobilization from the day of surgery is likely to reduce the risk of respiratory complications, venous thromboembolism, pressure sores, muscle deconditioning, and urinary retention.
Contraindications to day of surgery mobilization include pain, severe drowsiness, symptomatic hypotension, patient refusal, and acute clinical deterioration. These are encountered relatively infrequently in our experience. LIA should be avoided within 6 hours of a nerve block, but has no specific contraindications. We therefore use LIA in all cases, primarily as analgesia, and secondarily to assist day of surgery mobilization.
Other advantages of this protocol are that it is inexpensive, practical, inclusive, and requires minimal expertise. It adds negligible operating time, and can save anesthetic time by obviating the need for regional nerve blockade.
Conclusion
Opioid sparing anaesthesia, LIA, and day of surgery mobilization are well tolerated by patients with hip fracture, and potentially address their needs very well. The presented protocol is inexpensive, practical, inclusive, and requires minimal expertise. It may be improved by the inclusion of an FICB upon radiographic diagnosis. It has the potential to improve care while reducing cost. Further research is needed to establish the safety and effectiveness of these interventions, and assess any impact on complications, length of stay, and mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.