
Abstract
Objective:
Hand anthropometry, grip strength, and manual dexterity are fundamental to the safe and the effective performance of dental procedures. While these factors are individually important, their interrelationships in dental students remain insufficiently explored. This study aimed to examine the correlation of hand anthropometric dimensions with grip strength, and manual dexterity among dental students, and to evaluate their potential implications for dental education and ergonomic instrument design.
Methods:
This cross-sectional study included 100 dental students. Thirty hand anthropometric dimensions were measured using a digital caliper and measuring tape. Power grip strength was assessed using a Jamar hydraulic dynamometer, and fine grip strength (tip pinch and key pinch) using a hydraulic pinch gauge. Manual dexterity was evaluated with the Roeder Hand Aptitude Test. Descriptive statistics, independent t-tests, and Pearson correlation analyses were performed.
Results:
All hand anthropometric dimensions showed significant positive correlations with power and fine grip strength, with the strongest associations observed for palm width and hand length. Male students demonstrated significantly higher grip strength than female students across all grip types (p < 0.001). No significant sex-based differences were observed in manual dexterity. Most anthropometric dimensions were not significantly associated with manual dexterity, except for width-related measures (palm width, width across four fingers, and wrist width) in the more complex washer-and-nut task.
Conclusion:
Hand anthropometric dimensions are strong predictors of grip strength but have limited influence on manual dexterity. These findings suggest that while grip strength is largely determined by physical characteristics, manual dexterity is more dependent on motor coordination and practice. The results support the importance of ergonomics-based dental education and the consideration of hand-size variability in the design of dental instruments.
Introduction
Dentistry is a profession characterized by prolonged static postures, repetitive hand movements, and sustained precision tasks, which contribute to a high prevalence of work-related musculoskeletal disorders (MSDs). Epidemiological evidence indicates that approximately 70%–80% of dental professionals experience MSD symptoms during their careers. 1 These disorders commonly affect the neck, shoulders, upper limbs, and hands, leading to reduced clinical performance, diminished career longevity, and impaired quality of life.2–4 Inadequate application of ergonomic principles in dental practice, particularly in relation to hand–instrument interaction, has been identified as a key contributing factor to these disorders. 5
The hands serve as the primary functional interface in dental practice, enabling the execution of precise, repetitive, and force-controlled tasks. Effective dental performance requires the integration of grip strength, fine pinch control, manual dexterity, hand–eye coordination, and tactile sensitivity. 6 Common dental procedures—such as scaling, tooth preparation, and restorative treatments—demand sustained precision grip and repeated pinch forces, often over extended periods. When hand strength or anthropometric compatibility with dental instruments is insufficient, muscular fatigue may increase, task efficiency may decline, and the risk of upper-limb MSDs may be elevated.5,7,8
Hand grip strength is widely used as an objective indicator of hand muscle function and overall upper-limb strength. It is influenced by biological sex, body size, and hand anthropometric characteristics, including hand length, hand breadth, and finger dimensions.9–11 In the dental profession, repetitive forceful gripping and pinching have been identified as occupational risk factors for musculoskeletal symptoms affecting the hands and forearms. 12 From an ergonomic perspective, understanding the relationship between hand anthropometry and grip strength is essential for optimizing dental instrument design and reducing excessive force requirements and muscular strain during clinical tasks.13,14
Manual dexterity represents another critical component of dental competence, reflecting the ability to perform coordinated and precise movements under fine motor control. Unlike grip strength, dexterity is closely associated with neuromuscular coordination and motor learning acquired through repeated training. 15 Previous studies examining the relationship between hand anthropometry and manual dexterity have reported inconsistent findings, suggesting that anatomical dimensions alone may not fully explain dexterous performance.16,17 Recent evidence indicates that targeted strength and proprioceptive training can improve both grip strength and manual dexterity in healthy adults, 18 highlighting the functional interplay between physical capacity and motor control.
Despite the importance of hand function in dentistry, population-specific anthropometric data for dental students remain limited in many regions, including Iran. Given that hand anthropometric characteristics vary by ethnicity, biological sex, and lifestyle, the direct application of data derived from other populations may be inappropriate for local ergonomic design and educational planning. 19 Furthermore, few studies have simultaneously examined hand anthropometry, grip strength (including power and fine pinch), and manual dexterity within a single population of dental students.
Therefore, the present study aimed to investigate the relationships between hand anthropometric dimensions, grip strength, and manual dexterity among dental students. By clarifying how anatomical characteristics relate to hand performance function, this study provides evidence relevant to dental education, ergonomic instrument design, and the understanding of biomechanical factors associated with work-related MSDs in dental professionals.
Methods
Study design, setting, and participants
This cross-sectional study was conducted among undergraduate dental students at the Faculty of Dentistry, Urmia University of Medical Sciences, Iran, between 2019 and 2020. A total of 100 students were recruited by using simple random sampling.
The inclusion criteria were: (1) enrollment as a dental student, (2) absence of current pain or diagnosed MSDs affecting the upper limbs, and (3) willingness to participate in this study. The exclusion criteria included a history of upper limb surgery, an acute injury to the hand, wrist, or forearm within the previous 6 months, and any neurological or musculoskeletal condition that could affect in hand function.
All participants provided written informed consent prior to data collection. The study protocol was approved by the Research Ethics Committee of Urmia University of Medical Sciences (Ethics Code: IR.UMSU.REC.1398.494).
Sample size
The sample size was calculated based on anthropometric study guidelines using the ISO 15535:2006 standard. The calculation was based on the coefficient of variation obtained from a previous similar study, a relative precision of 5%, and a 95% confidence level. Based on these parameters, the minimum required sample size was estimated to be 64 participants. To increase statistical power and account for potential variability, 100 dental students were ultimately included.
Data collection and anthropometric measurements
Demographic data including age, biological sex, height, and weight were recorded for each participant. Thirty hand anthropometric dimensions, including finger lengths, finger breadths, hand breadth, hand length, hand depth, wrist breadth, and joint circumferences, were measured for the dominant hand (Figure 1). The measurement protocol was based on standard anthropometric guidelines commonly used in research of hand ergonomics. 20 Prior to data collection, all raters received standardized training on the anthropometric measurement protocol, including identification of anatomical landmarks and correct use of measurement instruments. Training was conducted using reference guidelines and pilot measurements under supervision. To ensure measurement accuracy and consistency, initial practice measurements were compared and discussed among raters, and any discrepancies were resolved through consensus before formal data collection began. Throughout the study, all measurements were performed according to the same standardized procedure.

Hand dimensions; 1 = fingertip to root digit 1 (FR1), 2 = fingertip to root digit 2 (FR2), 3 = fingertip to root digit 2 (FR3), 4 = fingertip to root digit 4 (FR4), 5 = fingertip to root digit5 (FR5), 6 = breadth at first joint of digit 1 (BF1), 7 = breadth at first joint of digit 2 (BF2), 8 = breadth at first joint of digit 3 (BF3), 9 = breadth at first joint of digit 4 (BF4), 10 = breadth at first joint of digit 5 (BF5), 11 = breadth at second joint of digit1 (BS1), 12 = breadth at second joint of digit 2 (BS2), 13 = breadth at second joint of digit 3 (BS3), 14 = breadth at second joint of digit 4 (BS4), 15 = breadth at second joint of digit 5 (BS5), 16 = circumference at first joint of digit 1 (CF1), 17 = circumference at first joint of digit 2 (CF2), 18 = Circumference at first joint of digit 3 (CF3), 19 = circumference at first joint of digit 4 (CF4), 20 = circumference at first joint of digit 5 (CF5), 21 = circumference at second joint of digit 1 (CS1), 22 = circumference at second joint of digit 2 (CS2), 23 = circumference at second joint of digit 3 (CS3), 24 = circumference at second joint of digit 4 (CS4), 25 = circumference at second joint of digit 5 (CS5), 26 = hand breadth (HB), 27 = hand length (HL), 28 = hand breadth at knuckle digit 1 (HBK), 29 = hand depth at knuckle digit 1 (HDk1), 30 = wrist breadth (WB).
Linear dimensions (lengths, breadths, and depths) were measured using a digital caliper (ASIMETO, Series 307, Germany) with a resolution of 0.01 mm and an accuracy of ±0.03 mm. Circumferential measurements were obtained using a flexible plastic measuring tape. All measurements were recorded in millimeters (mm).
To ensure measurement reliability, all measurements were conducted by trained assessors following a standardized protocol. Prior to data collection, assessors were trained in anthropometric measurement techniques, and calibration of instruments was verified.
Grip strength measurements
Hand grip strength was assessed for the dominant hand using standardized procedures recommended by the American Society of Hand Therapists and Mathiowetz et al.19,21
Power grip strength was measured using a hydraulic hand dynamometer (Jamar, Model 5030J1, Sammons Preston, Bolingbrook, IL, USA). Participants were seated with the shoulder adducted, elbow flexed at 90°, forearm in a neutral position, and wrist in slight extension. Participants were instructed to squeeze the dynamometer with maximum effort for approximately 3–5 s for each trial. Measurements were recorded in newtons (N).
Fine grip strength was assessed using a hydraulic pinch gauge (SAEHAN SH5005, SAEHAN Corporation, Masan, South Korea). Two types of pinches were measured:
Tip pinch (thumb to index finger).
Key pinch (lateral pinch between thumb and index finger).
Each measurement was repeated three times, and the mean value was used for analysis. A one-minute rest period was provided between trials to minimize muscle fatigue.
Manual dexterity assessment
Manual dexterity was assessed using the Roeder Hand Aptitude Test, a standardized instrument designed to evaluate the speed and coordination of hand and finger movements. The test includes tasks that require the manipulation and assembly of small components, such as rods, caps, washers, and nuts, using both hands.
Participants were instructed to complete each task as quickly and accurately as possible in accordance with the test manual. Performance was evaluated based on task completion time, with shorter times indicating better manual dexterity. No additional instruments were used beyond the standardized components of the Roeder test. 22
Statistical analysis
Data analysis was performed using SPSS software (version 16; IBM Corp., Armonk, NY, USA). Descriptive statistics, including means, standard deviations, and selected percentiles, were calculated for anthropometric dimensions, grip strength measures, and manual dexterity scores.
Independent t-tests were used to compare variables between male and female students. Pearson correlation coefficients were calculated to examine the relationships between hand anthropometric dimensions, grip strength, and manual dexterity. A p-value of less than 0.05 was considered statistically significant.
Results
A total of 100 dental students participated in this study, including 49 males and 51 females. The mean height and weight of participants were 169.8 ± 9.15 cm and 70.30 ± 12.08 kg, respectively. These variables were reported descriptively to characterize the study population and were not included in the percentile-based anthropometric analyses.
Hand anthropometric dimensions
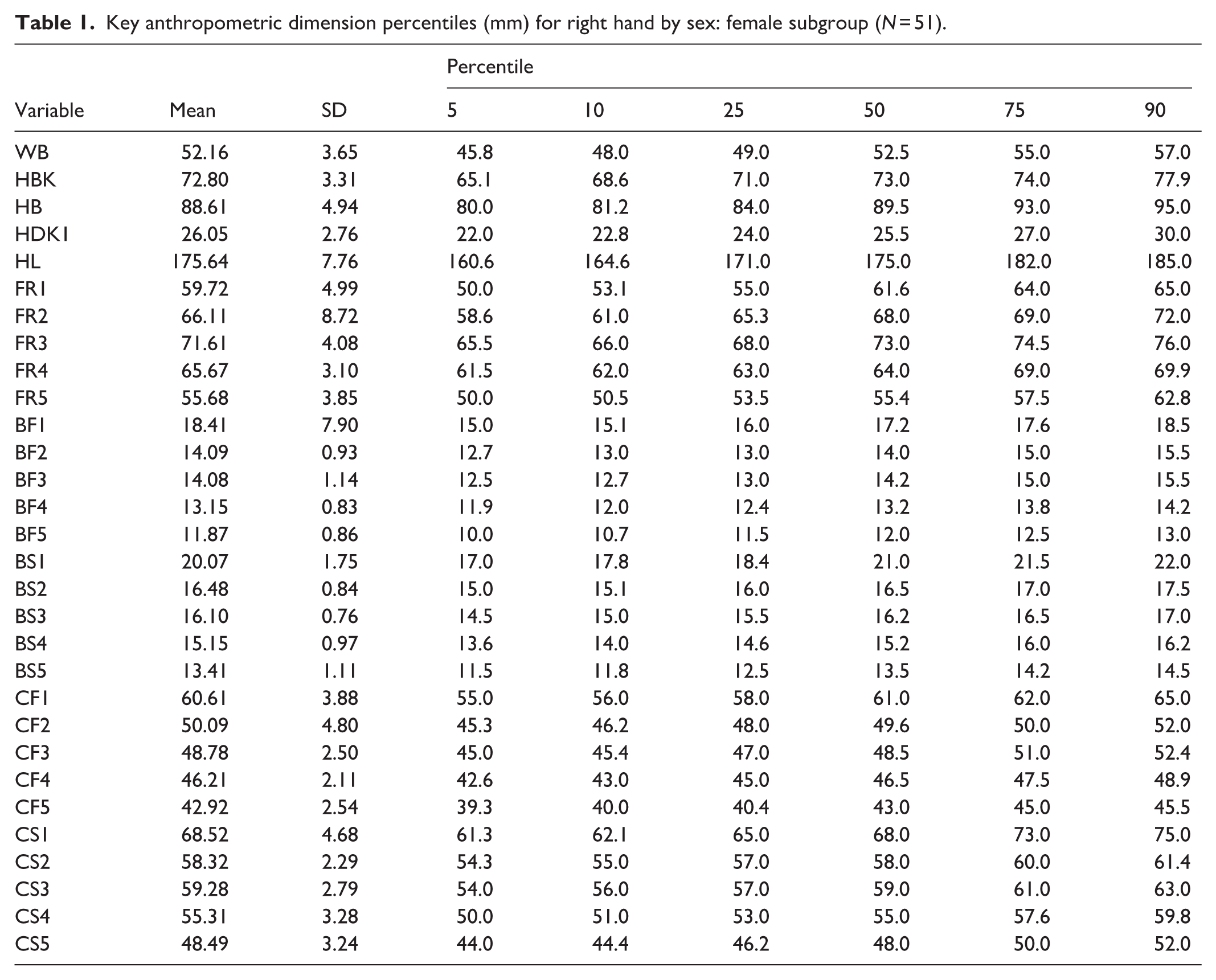
Thirty anthropometric dimensions of the dominant hand were measured. Descriptive statistics, including mean, standard deviation, and selected percentiles for male and female students, are presented in Tables 1 and 2.
Key anthropometric dimension percentiles (mm) for right hand by sex: female subgroup (N = 51).
Key anthropometric dimension percentiles (mm) for right hand by sex: male subgroup (N = 49).

Independent t-test analysis revealed statistically significant differences between male and female students for all measured hand anthropometric dimensions (p < 0.05), with males exhibiting larger values across all dimensions.
Grip strength
Three types of grip strength were assessed: power grip, tip pinch, and key pinch. Descriptive statistics for grip strength measures stratified by biological sex are presented in Table 3.
Descriptive statistics of manual dexterity during grip strength, stratified by gender.

Male students demonstrated significantly higher grip strength than female students for all three grip types. Independent t-test results showed statistically significant differences for tip pinch (T = 7.081, df = 98, p < 0.001), key pinch (T = 10.920, df = 68.217, p < 0.001), and power grip strength (T = 12.957, df = 62.646, p < 0.001). These comparisons are summarized in Table 5.
Manual dexterity
Manual dexterity was assessed using two tasks: working with rods and caps, and working with washers and nuts. Descriptive statistics for both tasks are presented in Table 4.
Descriptive statistics of manual dexterity scores (time-based), stratified by task and sex.

The mean (±SD) completion time for the rods-and-caps task using both hands was 20.30 ± 2.90 (Table 4). However as shown in Table 5, no statistically significant difference was observed between male and female students for this task (T = 0.364, df = 98, p = 0.717).
Sex-based comparison of hand grip strength and manual dexterity: Levene’s test and t-test results.
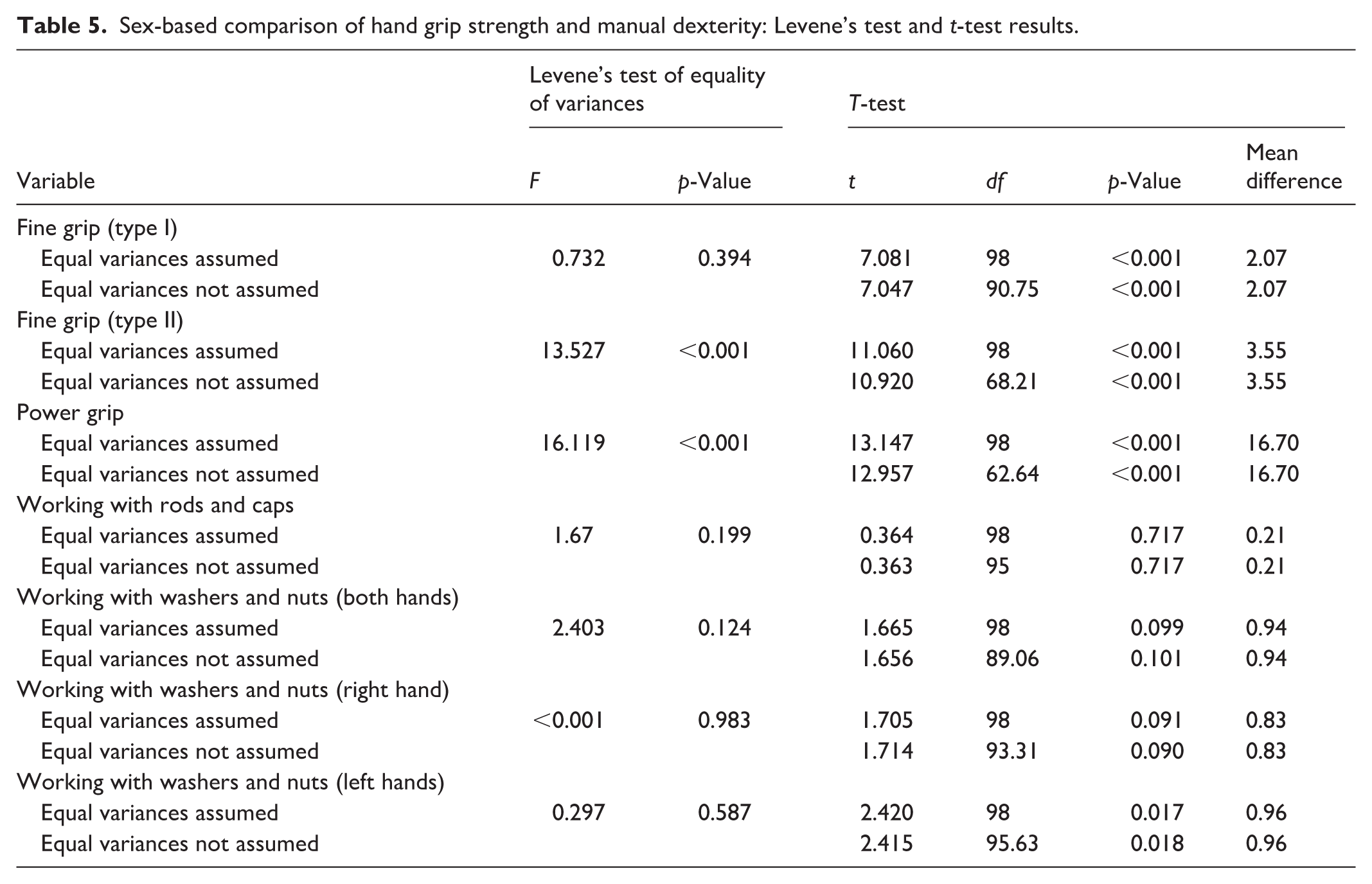
The mean (±SD) completion time for the washers-and-nuts task using both hands was 21.58 ± 2.86, with values of 22.06 ± 3.21 for males and 21.12 ± 2.41 for females. The difference between sexes was not statistically significant (T = 1.665, df = 98, p = 0.099). These comparisons are also presented in Table 5.
Correlation between hand anthropometric dimensions and grip strength
Pearson correlation analyses were conducted to examine the relationships between the 30 hand anthropometric dimensions and grip strength measures. The correlation coefficients are presented in Table 6.
Pearson correlation coefficients between hand anthropometric dimensions, grip strength and annual dexterity for all participants.

p < 0.05; **p < 0.01.
All anthropometric dimensions showed statistically significant positive correlations with tip pinch, key pinch, and power grip strength (p < 0.05). For tip pinch strength, the strongest correlation was observed with width across four fingers (r = 0.488), while the weakest was with hand depth (r = 0.253). For key pinch strength, the strongest correlation was found with dominant hand length (r = 0.615), and the weakest with hand depth (r = 0.338). For power grip strength, palm width demonstrated the strongest correlation (r = 0.780), whereas hand depth showed the weakest association (r = 0.341).
Correlation between hand anthropometric dimensions and manual dexterity
The relationships between hand anthropometric dimensions and manual dexterity performance were examined using Pearson correlation analysis, with results presented in Table 6. No statistically significant correlations were identified between any of the 30 anthropometric dimensions and performance on the rods-and-caps task. For the washers-and-nuts task, no significant correlations were observed with dominant hand length or hand depth. However, statistically significant positive correlations were identified with palm width, width across four fingers, and wrist width (p < 0.05).
Discussion
This study examined the relationships between hand anthropometric dimensions, grip strength, and manual dexterity among dental students, with the aim of clarifying how anatomical characteristics relate to functional hand performance relevant to dental practice. The findings indicate that hand anthropometric dimensions are strongly associated with both power and fine grip strength, whereas manual dexterity shows limited dependence on hand size and strength.
One of the key findings of this study is the significantly higher grip strength observed in male students compared with female students across all grip types. This finding is consistent with previous studies reporting greater grip and pinch strength in males, which has been attributed to differences in muscle mass, hand dimensions, and overall physical capacity.10,13 Similar sex-based differences in grip strength have also been reported among dental students and dental professionals in other populations. 9 Age was not included in the analysis because the study population consisted of a relatively homogeneous group of dental students with a narrow age range.
In the present study, all measured hand anthropometric dimensions were positively correlated with power grip strength as well as fine grip strength (tip pinch and key pinch). Width-related measures and hand length demonstrated the strongest associations. These findings are in line with earlier research indicating that larger hand dimensions contribute to greater grip and pinch strength, both in general populations and in occupational groups requiring precise hand function.13,14 Such relationships highlight the biomechanical importance of hand size in force generation during dental procedures that involve repetitive gripping and pinching.
In contrast to grip strength, manual dexterity did not differ significantly between male and female students, and most hand anthropometric dimensions were not significantly associated with dexterity performance. Only a limited number of width-related dimensions showed significant correlations with performance in the more complex washer-and-nut task. These findings are consistent with previous studies suggesting that manual dexterity is less dependent on anatomical characteristics and more influenced by neuromuscular coordination, fine motor control, and task familiarity.16,23 Efficient coordination between the central nervous system and hand muscles enables precise force modulation and timing, which are critical for fine motor tasks commonly performed in dentistry. In addition, repeated exposure to task-specific activities improves motor planning and sensorimotor integration, leading to more efficient and stable hand movements. Çakıt et al. 22 similarly reported weak or non-significant associations between hand dimensions and manual dexterity among dental students, despite clear relationships with grip strength. 23
The distinction observed in this study between grip strength and manual dexterity has important implications for dental education and occupational health. Dental tasks often require sustained gripping and precise finger movements over prolonged periods, which may contribute to fatigue and the development of work-related MSDs in the upper limbs.24,25 While adequate grip strength is necessary for effective tool manipulation, excessive force demands or prolonged static loading may increase musculoskeletal strain. It is important to note that higher grip strength or manual ability is not necessarily indicative of better functional performance in dental practice. While a certain level of grip strength is required to meet the functional demands of dental tasks, strength beyond these demands may not confer any additional benefits. Moreover, excessive or sustained force application may increase muscular load and contribute to fatigue and the development of work-related MSDs. Therefore, optimal rather than maximal grip strength appears to be more relevant for safe and efficient dental performance. 11 Systematic review evidence suggests that ergonomic interventions in dental practice are associated with reduced musculoskeletal symptoms and improved work performance in dental professionals and students. 25
The weak association between hand anthropometry and manual dexterity further suggests that dexterity is a skill that can be improved through training and practice rather than being determined by physical characteristics alone. This aligns with previous findings indicating that repeated task exposure and motor learning play a central role in the development of fine motor skills required in dentistry. 13 Consequently, structured preclinical training programs focusing on repetitive, task-specific skill development may help enhance manual dexterity regardless of hand size or strength.
The relevance of hand anthropometry and grip and pinch strength to work-related MSDs in dental professionals lies in the physical demands of dental tasks, which require sustained precision grip, repetitive fine motor movements, and controlled force application. Variations in hand dimensions and strength capacity may influence how forces are distributed across the hand and forearm during instrument use, potentially affecting muscular load and fatigue. By examining the relationships between hand anthropometric characteristics, grip strength, and manual dexterity, the present study provides a functional context for understanding individual differences that may contribute to biomechanical strain during dental work.
This study adds to the existing literature by linking detailed hand anthropometric measurements with both grip strength and manual dexterity within a single population of dental students. These findings contribute baseline evidence that may inform ergonomic considerations in dental education and instrument design, particularly in relation to hand–tool interaction.
Overall, the findings of this study are consistent with existing evidence demonstrating strong associations between hand dimensions and grip strength, alongside variable or weak relationships between anthropometry and manual dexterity.13,14,16,23 By simultaneously examining anthropometric characteristics, multiple grip strength measures, and standardized dexterity tasks in dental students, the present study adds to the growing body of literature informing ergonomic considerations and educational strategies in dentistry.
Several limitations should be considered. The cross-sectional design limits causal interpretation, and participants were recruited from a single dental school, which may restrict generalizability. Additionally, manual dexterity was assessed using standardized laboratory tasks rather than simulated clinical procedures, which may not fully reflect real-world dental performance. Future studies should incorporate longitudinal designs, diverse populations, and clinically relevant task simulations to further explore the relationships between hand anatomy, functional performance, and musculoskeletal health in dental professionals.
Conclusion
This study demonstrated significant associations between selected hand anthropometric dimensions, grip strength, and manual dexterity among dental students. The findings highlight the functional relevance of hand characteristics in dental practice and may inform ergonomic considerations in dental education and instrument design.
Footnotes
Acknowledgements
This article is the result of a research project approved by the Research Vice-Chancellor of Urmia University of Medical Sciences. In this way, the authors express their gratitude to the Department of Research and Management of the university and the participants of this study. We sincerely appreciate all the participants who cooperated with us throughout this study. The authors would like to acknowledge and thank the participants of this research.
Ethical considerations
This study was approved by the Medical Ethics Committee, Urmia University of Medical Sciences ethics code: IR.UMSU.REC.1398.494.
Consent to participate
All participants were informed about the purpose and procedure of the research and also signed an informed consent form before participation.
Consent for publication
The authors declare that this article contains original unpublished work and has not been submitted elsewhere for publication at the same time. All authors have consented to publication.
Author contributions
LRB and TA contributed to the study design and conceptualization. Data collection was performed by LRB and MJ. Data analysis was conducted by TA. MH drafted the initial manuscript. All authors contributed to data interpretation, critically revised the manuscript, and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article extracted from thesis of Master of Science, was funded by Urmia University of Medical Sciences, which provided essential financial support for the research (Ethics Code: IR.UMSU.REC.1398.494).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Some or all datasets generated during and/or analyzed during the current study are not publicly available (due to restrictions that their information could compromise the privacy of research participants) but are available from the corresponding author on reasonable request.*
Declaration on the use of AI
We utilized ChatGPT-4 (OpenAI) solely for the purpose of enhancing the clarity, coherence, and grammar of the English language. The authors have reviewed and approved all modifications to ensure accuracy and alignment with the research objectives.