
Abstract
Introduction
Hip fractures, which result in a high rate of complications and mortality, are a major public health concern in aging societies. Physical restraint for older patients with hip fractures may be employed to ensure safety, continue medical treatment, and minimize the risk of harm to oneself or others. This study aimed to investigate the current practices of physical restraint use among hip fracture patients across 2 acute-care hospitals, as well as uncover factors associated with physical restraint in patients with hip fracture.
Methods
We retrospectively reviewed all patients aged ≥65 years who underwent surgery for hip fractures at two institutions. Physical restraint was applied in accordance with institutional guidelines, following thorough assessments by physicians and nurses and obtaining informed consent from the patient or their family. When we examined the independent associations of physical restraint during hospitalization, the Poisson regression models were used to estimate the relative risks (RRs) and 95% confidence intervals (CIs).
Results
In total, 463 older patients with hip fractures were assessed. Among the included patients, 118 (25.5%) were subjected to physical restraint. Multivariable analysis revealed that 85 years or older (RR, 1.8; CI: 1.1–3.0), a BMI below 18.5 (RR, 1.8; CI: 1.4–2.5), dementia (RR, 2.3; CI: 1.7–3.1), stroke (RR, 1.5; CI: 1.1–2.0), impairment in physical function (RR, 3.1; CI: 1.2–8.3), and administration of antipsychotics (RR, 1.6; CI: 1.0–2.4) were significantly associated with the implementation of physical restraint.
Conclusions
This retrospective study provided real-world data regarding the use of physical restraint in older patients with hip fractures. Patients with older age, low BMI, dementia, stroke, impaired physical function, and administration of antipsychotics may be at high risk for the use of physical restraints. To minimize the use of physical restraints, future research for further data collection will be essential.
Introduction
Hip fractures represent a major public health concern, particularly in aging societies, considering that they are the most common type of fracture among older individuals, leading to serious functional disabilities and adversely affecting life expectancy. 1 Frailty, defined by shrinking, exhaustion, low physical activity, slowness, and weakness in older adults, is also strongly associated with hip fractures.2,3 Surgical treatment is recommended for hip fractures when the patient’s overall condition allows. However, older patients undergoing surgical treatment for hip fractures are at high risk of developing various complications, including pneumonia and pulmonary embolism. Studies have reported an overall adverse event incidence rate of approximately 75% within 6 months after surgery. 3 Early surgical intervention has been reported to significantly reduce mortality rates, prompting the recommendation of surgery within 48 h of injury in recent years. 4
Delirium frequently occurs in older patients during hospitalization, presenting a significant concern for patients, their families, and healthcare providers. 5 Studies have reported that 20%–30% of patients with hip fractures experience delirium during hospitalization, with risk factors including dementia, male sex, older age, living in a facility before surgery, polypharmacy, poor nutritional status, decreased physical function, and reduced cerebral blood flow.6,7 Physical restraint may be applied to patients with hip fractures hospitalized in acute-care hospitals who are at high risk for delirium to ensure patient safety, continue medical treatment, and minimize the risk of harm to the self or others. However, the use of physical restraint in hospitalized patients entails ethical considerations as well as physical and psychological effects, necessitating proper management and evaluation. 7 Given that older individuals are especially vulnerable and often suffer from decreased physical function, dementia, and other mental issues, the use of physical restraints should be carefully considered. 7 Therefore, this issue requires adequate communication between patients, families, and healthcare providers as well as practices based on ethical guidelines.8,9 Ideally, physical restraints can only be used in patients with hyperactive delirium who present with severe agitation, once organic triggers have been corrected and non-pharmacological measures have been implemented. While several studies have investigated the use of physical restraints in intensive care units, those specifically addressing physical restraint practices among older hip fracture patients appear to be scarce.10-14 This study aimed to investigate current practices of physical restraint use among hip fracture patients across two acute-care hospitals and identify factors associated with physical restraint.
Materials and Methods
Subjects
We retrospectively collected the clinical data of consecutive patients aged ≥65 years, who underwent surgery for hip fractures at two acute-care hospitals between April 2019 and March 2021. The specific exclusion criteria were pathological fractures, revision surgeries, and missing data on admission blood tests or physical function.
Ethics Approval and Consent to Participate
This study was approved by the institutional ethics committee. Informed consent was obtained using the opt-out method available on the website. All the study methods were conducted in accordance with the guidelines stated in the Declaration of Helsinki.
Data Acquisition
The following data were collected from the electronic patient record file and assessed: age; body mass index (BMI); sex; surgical procedures, including open reduction and internal fixation, bipolar hip arthroplasty, and total hip arthroplasty; American Society of Anesthesiologists physical status; days from admission to surgery; use of physical restraint; days from admission to physical restraint; medical history, including hypertension, dyslipidemia, diabetes, stroke, heart disease, malignancy, and dementia; preoperative prescribed drugs; and serum levels of albumin on blood examination. Impairment in physical function upon admission was diagnosed based on answers to two questions extracted from the Kihon Checklist, a simple and practical tool for assessing health status and independence in daily living among older adults. 15 Patients who responded “no” to the question “Do you normally stand up from a chair without any aids?” or “yes” to “Have you experienced a fall in the past year?” were determined to have impaired physical strength.
Physical Restraint
Physical restraints were used as a temporary measure to ensure patient safety and prevent harm to self or others only after other interventions such as environmental adjustments, proved ineffective. The environmental adjustments included medication review, relocation of the patient’s room closer to the nursing station, active communication, and early rehabilitation. Physical restraints were applied following appropriate assessments by both physicians and nurses, and with consent obtained from the patient or their family. Discussions on the possibility of removing restraints were held daily during the conferences. The following tools were used for physical restraint: wrist or ankle restraints, waist belts, glove-type restraints, and bed-exit sensors. Medical records indicating the use of these tools were considered evidence of physical restraint.
Polypharmacy and Potentially Inappropriate Medications (PIMs)
The cutoff number of prescribed drugs for polypharmacy was set at 6. 16 According to the guideline, 17 the following 19 categories are considered PIMs requiring special caution when prescribing: antipsychotics, hypnotics, antidepressants, sulpiride, antiparkinsonian drugs, steroids, antithrombotic drugs, digitalis, diuretics, β-blockers, α-blockers, first-generation antihistamines, H2-receptor antagonists, antiemetic drugs, laxatives, antidiabetic drugs, insulin, overactive bladder medications, and nonsteroidal anti-inflammatory drugs. All the prescribed drugs in these categories were identified as PIMs.
Statistical Analyses
The t-test and chi-square test were used for comparison of data among two groups. Data are shown as mean ± standard deviation. When we examined the independent associations of physical restraint during hospitalization, the Poisson regression models were used to estimate the relative risks (RRs) and 95% confidence intervals (CIs). We included all variables associated with physical restraint in the univariable analysis (BMI, medical history of stroke and dementia, serum level of albumin, impairment of physical function, and medication of antipsychotics and α-blockers), and age and sex as a priori factors in the Poisson regression model. Poisson regression was performed using the STATA16 software (Stata Corporation, College Station, TX, USA). P values of <0.05 were considered to indicate statistical significance.
Results
Timing of Physical Restraint Application During Hospitalization (n = 118).

Number of Cases for Each Type of Physical Restraint (n = 118).

Comparison of Baseline Characteristics Between two Groups.

T-test, chi-square test.
BMI: Body mass index, ORIF: Open reduction and internal fixation, BHA: Bipolar hip arthroplasty, THA: Total hip arthroplasty, ASA-PS: American Society of Anesthesiologists physical status.
Number and Prevalence of Cases Taking Potentially Inappropriate Medications.
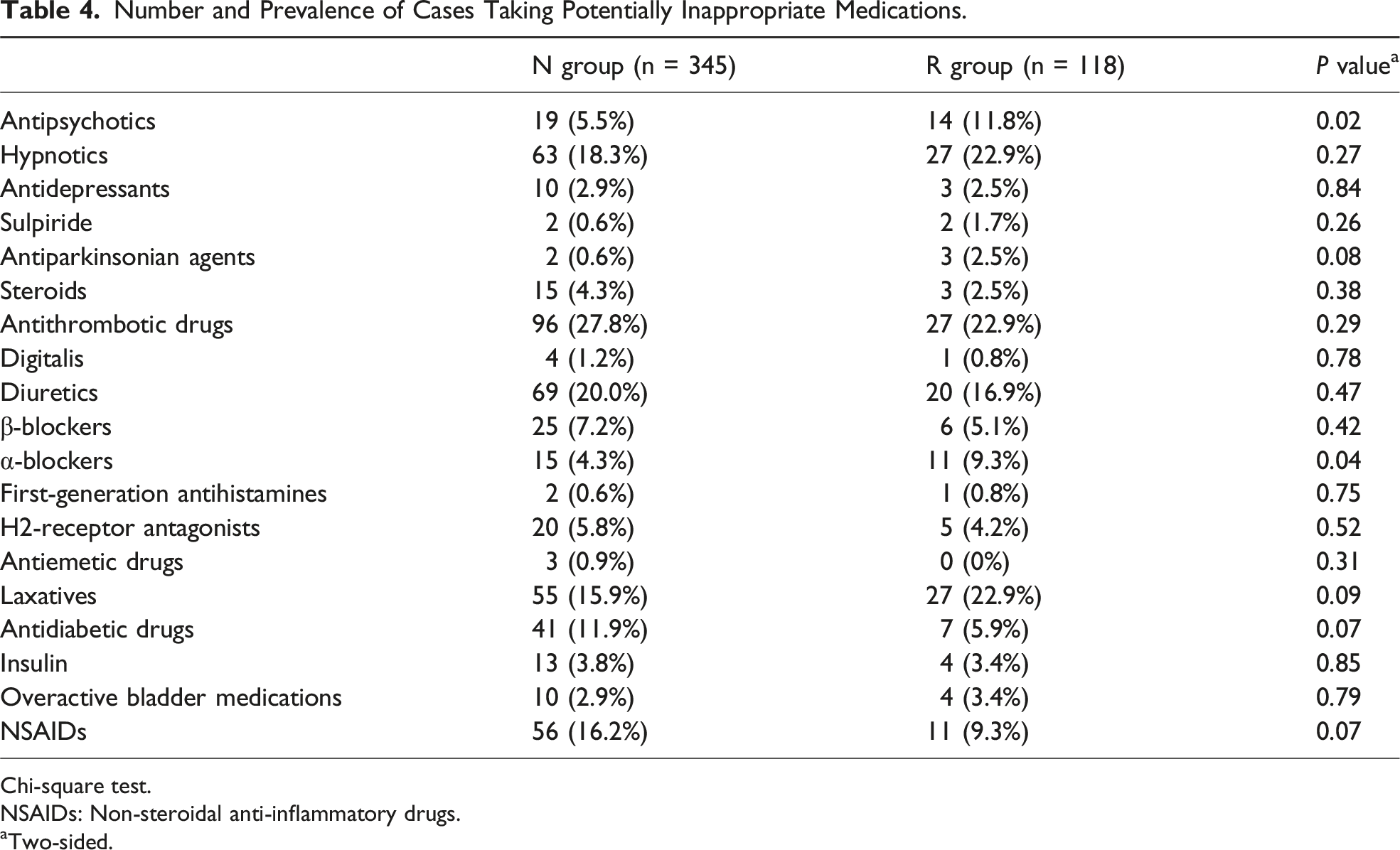
Chi-square test.
NSAIDs: Non-steroidal anti-inflammatory drugs.
aTwo-sided.
Association Between Uncover Factors and Physical Restraint During Hospitalization.

We applied a Poisson regression model, and estimated RRs after adjustment for all variables included in this table.
aTwo-sided.
Discussion
Our findings showed that approximately 25% of older patients with hip fractures experienced physical restraint during hospitalization in acute-care hospitals. Gupta, et al reported that the frequency of physical restraint usage in hospitals across the United States was 0.63%. 13 When limited to acute-care hospitals, Thomann et al 14 reported that the frequency of restraint use was 8.7%. In comparison to the data from the previous studies, the frequency of physical restraint use in our study is markedly higher. This discrepancy is likely attributable to differences in the study populations. While the two previous studies included participants aged 18 years and older, our study specifically targeted individuals aged 65 years and older who had sustained hip fractures. Therefore, we must recognize that physical restraints are commonly used in older patients with hip fractures. In the two facilities included in this study, the frequency of restraint use has decreased compared to the study period. In addition, the majority of the cases were subjected to physical restraint within 2 days after admission. These observations indicate that physical restraints are used early in the hospital stay, which aligns with previous reports showing that most cases of delirium occur in the early stages of hospitalization due to factors such as environmental changes and worsening medical conditions. 18 Therefore, we emphasize the need to be cautious from the time of admission to avoid the use of physical restraints.
The factors associated with physical restraint in patients with hip fractures identified in this study aligned with previously reported risk factors for delirium in this population.6,7 However, the relationship between delirium and physical restraint among hospitalized older patients is highly complex and multifaceted. 19 Delirium is defined as an acute cognitive impairment characterized by a range of symptoms including attention disorders, changes in cognitive function, perceptual distortions, and unstable levels of consciousness. 20 Occasionally, patients with delirium may harm themselves or display uncooperative behavior during medical procedures, prompting healthcare providers to consider physical restraint as a last resort. Considering that risk factors for delirium include severe pain or postoperative conditions, both of which are relevant to patients with hip fractures, older patients with hip fractures are likely to have increased incidence of delirium upon hospitalization, necessitating frequent consideration of physical restraints.21,22 In this study, we were unable to accurately assess whether delirium occurred in all patients. Meanwhile, we were able to investigate the presence of dementia, which is the primary risk factor for delirium, 23 based on the medical history. Therefore, we included dementia as one of the explanatory variables in the multivariable analysis. As expected, dementia was one of the factors associated with physical restraint in older patients with hip fractures.
Given reports showing an association between polypharmacy in older patients and delirium during hospitalization, the current study investigated the impact of polypharmacy and the use of PIMs on the implementation of physical restraints. 24 Our results showed that while polypharmacy was not significantly associated with physical restraints, the administration of antipsychotics was found to have a significant association. In addition, our study identified older age, low BMI, stroke, dementia, and impairment in physical function as factors associated with the use of physical restraints. Considering that these factors are significant indicators of progression toward frailty, our results suggest that within the population of older patients with hip fractures, those with more advanced frailty may be highly associated with physical restraint. 25 Consequently, healthcare providers must be extremely cautious when caring for the most frail and vulnerable patients, who are at greatest risk of developing delirium. This highlights the importance of environmental preparation for patients with these factors to reduce the use of physical restraint as much as possible. Evidence has shown that physical restraint can further increase patient anxiety and worsen symptoms of delirium. 26 Therefore, the appropriate use of physical restraint, which ensures patient safety while minimizing undue stress, requires innovative care strategies, especially for patients with advanced frailty. 27 Previous research has shown that implementing alternative interventions, such as environmental modifications, proper sleep management, cognitive therapies, and personalized support from family and staff, can help prevent or mitigate delirium. 28 Optimizing the hospital environment through enhanced lighting, adjustments in sound levels, and the provision of shared spaces can help prevent the onset of delirium and, as a result, reduce the frequency of physical restraints.29,30 Taken together, hospitalization of patients with hip fractures who possess factors associated with physical restraint will require increased involvement from healthcare providers immediately upon admission. To minimize the use of physical restraints, we should have an opportunity to educate healthcare providers regarding the high rate of restraint use in older patients with hip fractures and to educate them on better strategies.
This study has several limitations. First, although regulated by institutional guidelines, the application of physical restraint was ultimately determined by physicians and nurses. This process results in variations in the criteria for application across individual cases. 31 Second, this was a retrospective cross-sectional study. In the future, a longitudinal investigation is needed to determine whether implementing environmental modifications can reduce the frequency of physical restraint in older patients with hip fractures. Third, when assessing the impairment in physical function, we used the answers to two questions from the previously reported Kihon Checklist. 15 However, the validation of the Kihon Checklist was originally conducted on Japanese community-dwelling older adults and does not target patients hospitalized for hip fractures, who were the subjects of this study. 32 Fourth, the sample size in this study was relatively small. However, when we performed a post-hoc power calculation based on the current sample size, the point estimate of the odds ratio for detecting an association with physical restraint during hospitalization at a power of 0.8 was 1.5. Fifth, this study did not directly assess patients’ delirium, which is a weakness in exploring factors associated with restraint use. Sixth, as this study was conducted in two Japanese hospitals, the generalizability is limited. Caution is needed when applying the findings to other countries with different restraint guidelines. Seventh, cases with missing admission data were excluded in this study. Since more severe cases are likely to have missing data, there is a possibility that this may have introduced bias into the analysis. Nevertheless, to the best of our knowledge, this is the first study to determine the reality of physical restraint implementation in older patients with hip fractures undergoing surgery. We believe that the findings presented herein would be beneficial for all healthcare providers managing older patients with hip fractures.
Conclusion
Although this study has several limitations, it provided real-world data on the use of physical restraint in older patients with hip fractures undergoing surgery in acute-care hospitals. Based on our findings, special attention should be paid to the use of physical restraint among older patients with hip fractures who present with advanced frailty, characterized by older age, low BMI, stroke, dementia, impaired physical function, and administration of antipsychotics upon admission. Ultimately, the current hospitalization environment for older patients with hip fractures must be improved to eliminate the use of physical restraint.
Footnotes
Acknowledgments
The authors would like to thank Ms. Satoko Okada and Ms. Yukari kuno for technical supports.
Ethical Statement
Consent to Participate
Informed consent was waived by Fujita Health University Ethics Committee. Fujita Health University Ethics Committee also approved our use of the opt-out method for obtaining consent, indicating that all eligible patients were included in the present study unless they contacted us to opt out.
Author Contributions
N.F. and S.Y. designed the study. S.F., T.T., T.H., K.S., R.T., and M.M. contributed to the analysis and interpretation of data. S.K. and T.M. performed the statistical analysis. S.F., S.K., T.M., and N.F. wrote the initial draft of the manuscript. T.T., T.H., K.S., R.T., M.M., and SY. critically reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author on reasonable request.