
Abstract
Background
Preoperative anemia has been associated with perioperative morbidity and mortality in patients undergoing cardiac and non-cardiac surgery. Preoperative anemia is common in elderly hip fracture patients. The primary objective of the study was to explore the relationship between preoperative hemoglobin levels and postoperative major adverse cardiovascular events (MACEs) in hip fracture patients over 80 years.
Methods
The retrospective study enrolled hip fracture patients over 80 years from January 2015 to December 2021 in our center. The data were collected from the hospital’s electronic database after approval by the ethics committee. The primary objective of the study was to investigate MACEs, and the secondary objectives included in-hospital mortality, delirium, acute renal failure, ICU admission rate, and transfusion (>2 U).
Results
912 patients were entered for final analysis. Based on the restricted cubic spline, the risk of preoperative hemoglobin (<10 g/DL) was associated with an increased risk of postoperative complications. With univariable logistic analysis, a hemoglobin level <10 g/DL was associated with increased MACEs [OR 1.769, 95% CI (1.074, 2.914), P = .025], in-hospital mortality [OR 2.709, 95% CI (1.215, 6.039), P = .015] and transfusion >2 U risk [OR 2.049, 95% CI (1.56, 2.69), P < .001]. Even after adjustment for confounding factors, MACEs [OR 1.790, 95% CI (1.073, 2.985), P = .026], in-hospital mortality [OR 2.81, 95% CI (1.214, 6.514), P = .016] and transfusion >2 U rate [OR 2.002, 95% CI (1.516, 2.65), P < .001] were still higher in the lower hemoglobin level cohort. Moreover, a log-rank test showed increased in-hospital mortality in the cohort with a preoperative hemoglobin level of <10 g/DL. However, there was no difference in delirium, acute renal failure, and ICU admission rates.
Conclusions
In conclusion, for hip fracture patients over 80 years, preoperative hemoglobin levels <10 g/DL might be associated with increased postoperative MACEs, in-hospital mortality, and transfusion >2 U.
Keywords
Introduction
Hip fracture is the main traumatic injury among seniors and has become a public health issue with a growing aging population. Comorbidities in older patients may deteriorate rapidly due to direct and indirect influences such as immobilization, pain and anemia. In addition, the hip fracture results in blood loss and may lead to or worsen anemia in elderly patients.1–4 Preoperative anemia is associated with perioperative morbidity and mortality in patients undergoing cardiac and non-cardiac surgery.5–10 Hemoglobin levels below 12 g/dL in women and below 13 g/DL in men are defined as anemia by the WHO. 11 Anemia is common in older patients, especially in traumatic surgery patients. Preoperative anemia can affect functional mobility (heart, brain, kidney) of surgical patients. Research indicates that the clinical outcomes of anemia might result from anemia-induced tissue hypoxia. 12 Few studies have addressed the relationship between preoperative anemia and postoperative outcomes in patients over 80 years undergoing hip surgery and the optimal level of preoperative hemoglobin in these patients. The purpose of this retrospective observation study was to investigate the relationship between preoperative hemoglobin levels and postoperative morbidity and mortality in this subgroup of patients.
Materials and Methods
Data Sources and Study Population
After approval from the institutional Ethics Committee, we accessed the medical records of all eligible patients via the clinical electronic database. This was a retrospective cohort study and the procedure followed strobe guidance. Data on elderly surgical patients (over 80 years) with hip fractures were extracted from the clinical electronic database from January 2015 to December 2021. The exclusion criteria were as follows: (1) multiple fractures; (2) other surgeries within 3 months; (3) revision surgery; (4) brain surgery history; (5) missing baseline data.
Endpoints
The primary outcome was major adverse cardiac events (MACEs). The secondary outcomes were in-hospital mortality, delirium, acute renal failure (ARF), ICU admission, and perioperative transfusion (>2 U). MACEs refer to recurrent angina, myocardial infarction, cardiac failure, malignant arrhythmia, and death from cardiovascular causes. A decrease in eGFR and an increase in creatine were used to diagnose ARF. Delirium was diagnosed through the Confused Assessment Method (CAM-5).
Covariates Associated With Endpoints
Demographic variables were extracted for baseline characteristics. Comorbidities were recorded, including hypertension, diabetes, chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD), heart failure, atrial fibrillation, stroke, renal failure, and cancer. Anesthesia types included general anesthesia with a nerve block, nerve block with sedation, and neuraxial anesthesia. The hip fracture types were intertrochanteric, subtrochanteric, femoral neck, and trochanter. Surgical procedures included internal fixation, hemiarthroplasty, and arthroplasty.
Statistical Analysis
The continuous variables are presented as the mean (SD), and the proportion is presented for categorical variables. The enrolled patients were divided into 4 cohorts as indicated by the transfusion guidelines for comparison of baseline characteristics. For analysis of variance, the chi-square test, Fisher exam test, or Kruskal-Wallis rank-sum test were applied as appropriate. To explore the association between the level of preoperative hemoglobin and all endpoints of elderly patients over 80 years undergoing hip fracture surgery, restricted cubic spline curves (RCSs) were used based on Cox proportional hazards models with 4 knots at the 5th, 35th, 65th, and 95th percentiles. 13 The analyses were adjusted for age, sex, preoperative days, and comorbidities. Primary and secondary outcomes were analyzed using both unadjusted regressions and adjusted multivariable regression, with a preoperative hemoglobin level of 10 g/DL as the reference group based on the RCS curve. For sensitivity analyses, the subgroup of patients aged from 80 years to 89 years were tested for all endpoints. A two-tailed P value of less than .05 was considered statistically significant. All analyses were processed using SPSS 26.0 and R version 4.0.
Results
From 2015 to 2021, a total of 1 116 hip fracture patients over 80 years enrolled in the study. Seventy-two patients were excluded with multiple injuries/multiple procedures during the same admission period. Patients undergoing ipsilateral revision procedures were also excluded. Ten patients were excluded for receiving other surgeries within 3 months. Another sixty-six patients were excluded for missing baseline data. A total of 912 eligible hip fracture patients over 80 years of age were included in the study (Figure 1). Schematic demonstration of the study sample.
Baseline Characteristics of Hip Fracture Patients Over 80 Years Old.
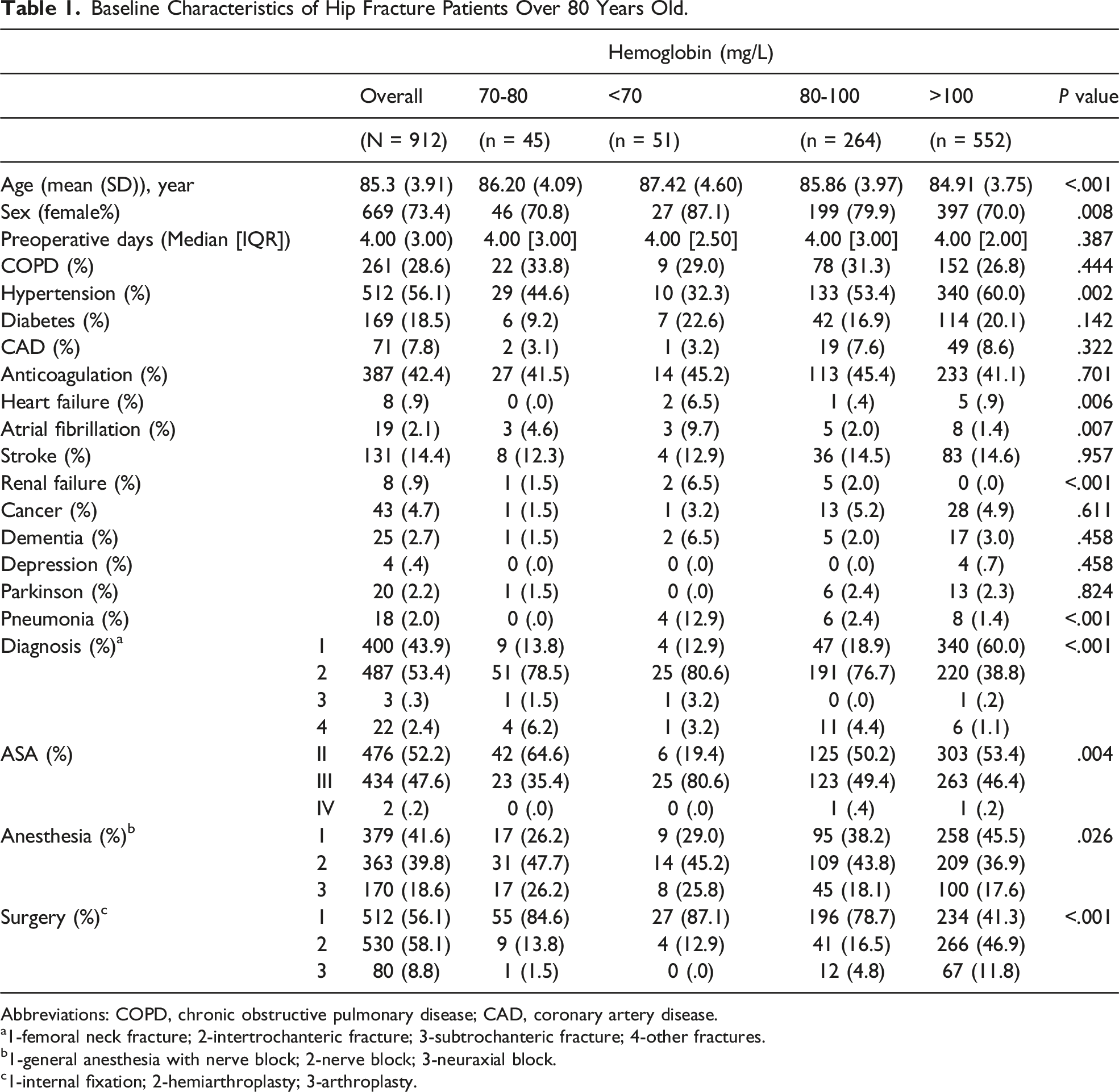
Abbreviations: COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease.
a1-femoral neck fracture; 2-intertrochanteric fracture; 3-subtrochanteric fracture; 4-other fractures.
b1-general anesthesia with nerve block; 2-nerve block; 3-neuraxial block.
c1-internal fixation; 2-hemiarthroplasty; 3-arthroplasty.
Preoperative Hemoglobin and Endpoints
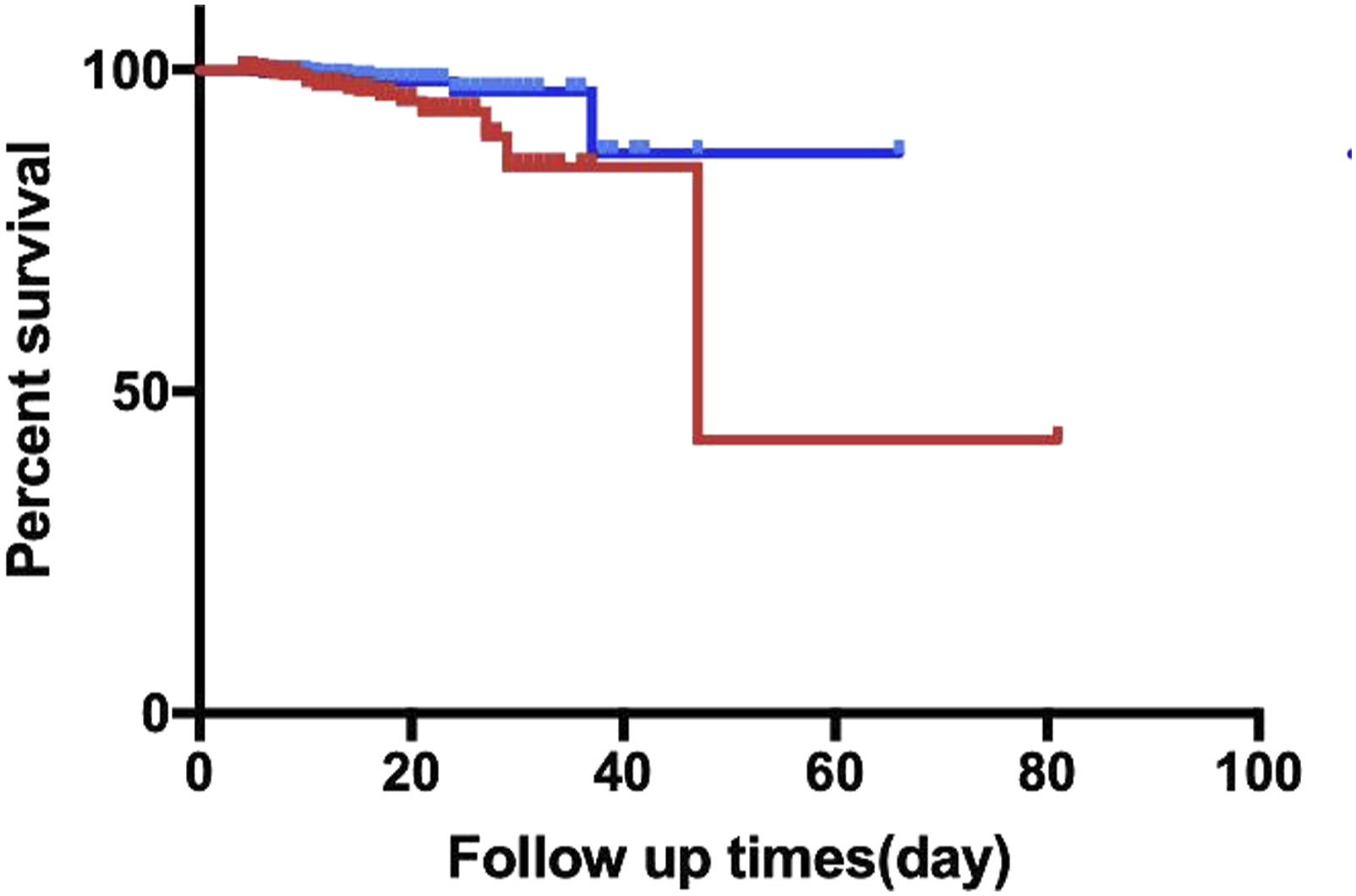
For postoperative complications, sixty-seven MACEs and twenty-six deaths were identified during hospitalization after surgery. After adjusting for all potential confounders (age, sex, ASA classification, diagnosis, anesthesia methods, surgery types, and comorbidities) for the endpoints, the relationship between preoperative hemoglobin level and MACEs/other composite complications were shown in Figure 2. According to the graph, a preoperative hemoglobin level higher than 10 g/DL decreased the occurrence of complications. With univariable logistic analysis, the hemoglobin level <10 g/DL cohort was associated with increased MACEs [OR 1.769, 95% CI (1.074, 2.914), P = .025], in-hospital mortality [OR 2.709, 95% CI (1.215, 6.039), P = .015], and transfusion >2 U rate [OR 2.049, 95% CI (1.56, 2.69), P < .001], but there was no difference with delirium rate, ARF and ICU admission rate between the cohorts of hemoglobin level <10 g/DL and hemoglobin level ≥10 g/DL. Even after adjustment for age, sex, ASA classification, diagnosis, anesthesia methods, surgery, and comorbidities (COPD, hypertension, diabetes, heart failure, atrial fibrillation, preoperative pneumonia and renal failure), there was a similar increase in MACEs [OR 1.790, 95% CI (1.073, 2.985), P = .026], in-hospital mortality [OR 2.81, 95% CI (1.214, 6.514), P = .016] and transfusion >2 U rate [OR 2.002, 95% CI (1.516, 2.65), P < .001]. The log-rank analysis also showed increased hospital length of stay in the cohort with a preoperative hemoglobin level <10 g/DL (Table 2). Additionally, Kaplan-Meier analysis demonstrated that a hemoglobin level <10 g/DL was associated with higher in-hospital mortality (Figure 3). A. Preoperative hemoglobin level and RCS of MACEs. Results were adjusted for age, sex, ASA classification, diagnosis, anesthesia methods, surgery, and comorbidities (COPD, hypertension, diabetes, heart failure, atrial fibrillation, preoperative pneumonia, and renal failure). The pink color zone represents the 95% confidence intervals for the spline model. B. Preoperative hemoglobin level and RCS of other composite complications. Results were adjusted for age, sex, ASA classification, diagnosis, anesthesia methods, surgery, and comorbidities (COPD, hypertension, diabetes, heart failure, atrial fibrillation, preoperative pneumonia, and renal failure). The pink color zone represents the 95% confidence intervals for the spline model. Unadjusted and Adjusted Outcomes of Postoperative Complications Between Cohorts of Hemoglobin <10 g/DL and Hemoglobin >10 g/DL. Abbreviations: MACEs, major adverse cardiac events; ARF, acute renal failure. Probability of in-hospital mortality. Line (in blue) represents preoperative hemoglobin >10 g/DL, and line (in red) represents preoperative hemoglobin <10 g/DL.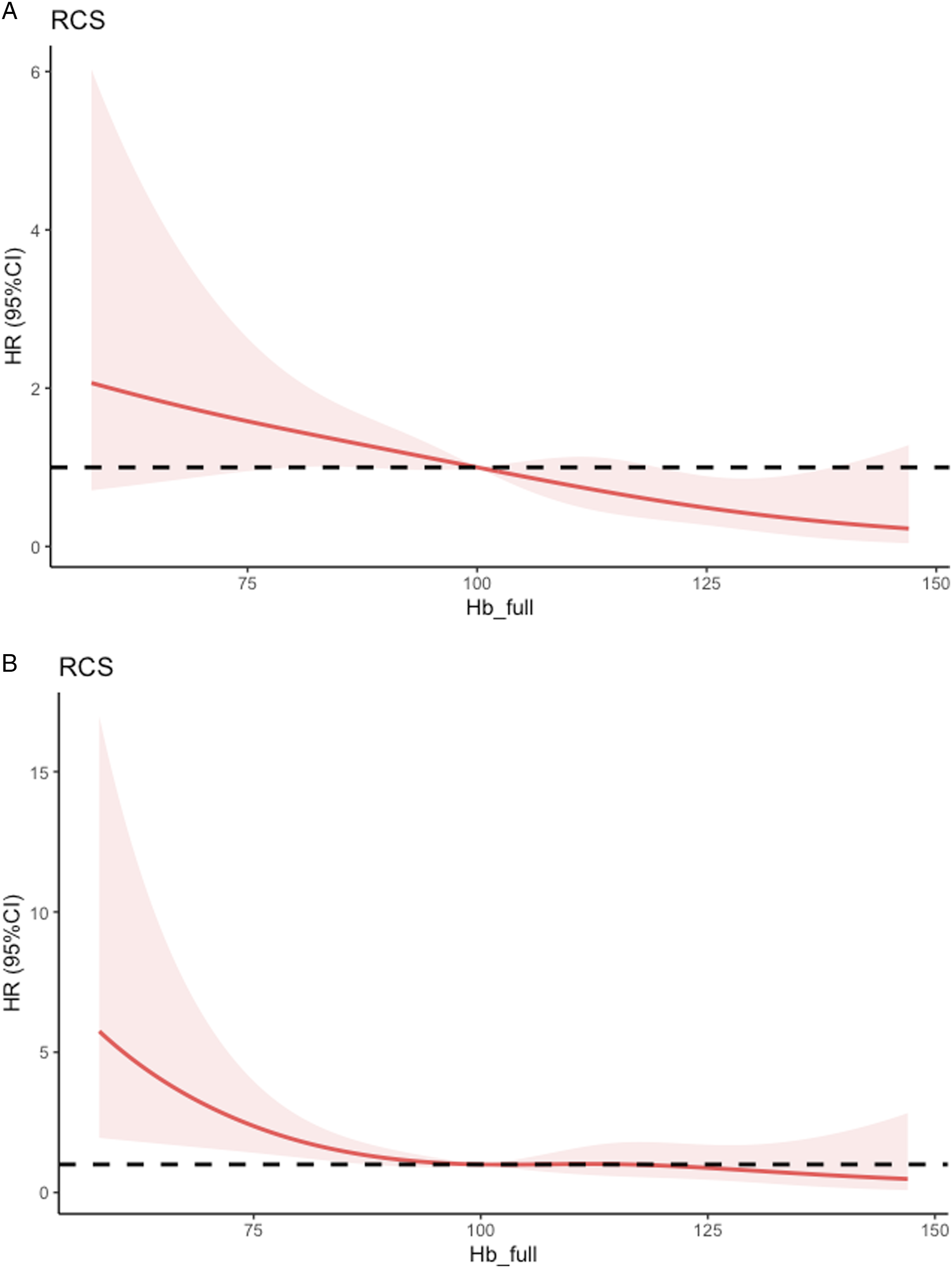

Sensitivity Analysis
Sensitivity Analysis of Patients of 80 Years to 89 Years Between Cohorts of Hemoglobin <10 g/DL and Hemoglobin >10 g/DL.

Abbreviations: MACEs, major adverse cardiac events; ARF, acute renal failure.
Discussion
In the current study, we demonstrate that for patients over 80 years receiving hip fracture surgery, a preoperative hemoglobin level <10 g/DL might be associated with increased postoperative MACEs, in-hospital mortality, and more transfusions >2 U. The results are the same even after multivariable adjustment and subgroup analysis.
Several studies have explored the relationship between preoperative anemia and postoperative outcomes. A retrospective cohort study reported by Musallam and colleagues analyzed data from 227 425 patients undergoing noncardiac surgery and concluded that preoperative anemia was independently associated with an increased risk of 30-day morbidity and mortality. 5 Furthermore, they found that even with a mild degree of preoperative anemia, composite postoperative morbidity at 30 days was higher in patients with anemia than in those without anemia. Their research focused on femoral neck fracture and surgery of arthroplasty, but the intertrochanteric fracture happened more frequently in the over 80 years old group and arthroplasty was not priority as other surgery types in over 80 years. Another large-scale retrospective cohort study recorded 5 922 primary arthroplasty procedures and reported that the presence of anemia in the cohort was associated with inferior outcomes after arthroplasty. Anemics were more likely to require blood transfusion than patients without preoperative anemia, which was consistent with our conclusion. Furthermore, they also found that anemics were more likely to have postoperative complications than patients without anemia. 6 Similarly, we reported increased cardiovascular-related complications and in-hospital mortality, which agreed with the results of Bailey and colleagues.
Compared to other factors, such as old age, anemia is a modifiable preoperative condition. There is a lack of a universal preoperative hemoglobin threshold for frail elderly patients over 80 years receiving hip fracture surgery. Transfusion guidelines 2011 recommended preoperative hemoglobin levels of 9 g/DL or 10 g/DL for patients with a history of ischemic heart disease as the transfusion threshold and suggested a higher blood transfusion trigger for older patients. 14 In Denmark, a hemoglobin level of 9.7 g/DL is recommended as the RBC transfusion threshold. 15 Guidelines for the management of hip fractures 2021 recommended that the recognition and management of blood should precede according to an agreed-upon hospital protocol. 16
What is the optimal preoperative hemoglobin level for hip fracture patients over 80 years? The recommendations from the 2018 Frankfurt consensus conference suggested 8 g/DL in patients with hip fracture and cardiovascular disease or other risk factors. However, although data from 17 607 literature citations and 145 studies, including 63 RCTs with 23 143 patients and 82 observational studies with more than 4 million patients, were analyzed, this was a conditional recommendation, and only 10 studies analyzed hip fracture patients. Furthermore, none of the studies focused on patients over 80 years old. 17 Neef and colleagues 18 pointed out the current situation and concluded that preoperative anemia management has not yet been established, but the results of the studies confirmed the positive effect of preoperative anemia diagnosis and treatment. However, for the special group of hip surgery patients over 80 years, the workflows of inspection and correction of preoperative anemia were established in our center. The guidelines in 2018 suggested that the hemoglobin trigger could be lower than 10 g/DL, but the evidence for frail hip fracture patients over 80 years old was insufficient. 19 Although blood management in cardiac surgery favors the restrictive transfusion strategy compared to the liberal transfusion strategy.20–23trials and reviews focused on hip fracture patients hold a different view. A context-specific systematic review and meta-analysis reported that restricted transfusion strategies should be applied with caution in high-risk patients undergoing major surgery and this may be detrimental. 24 It was a systematic review in perioperative and acute care settings according to patient characteristics and clinical settings and was closer to real-world research. A meta-analysis by Gu and colleagues 25 reviewed ten studies and found that restrictive transfusion (mostly a hemoglobin level of 8 g/DL or symptomatic anemia) increases the risk of cardiovascular events compared to liberal (mostly a hemoglobin level of 10 g/DL) transfusion (RR = 1.51, 95% CI: 1.16, 1.98; P = .003) in patients undergoing hip fracture surgery. The TRIFE randomized controlled trial enrolled 284 hip fracture patients over 65 years of age and concluded that for frail elderly hip fracture patients, recovery from a physical disabilities transfusion strategy (threshold 9.7 g/DL) was similar to a liberal strategy (<11.3 g/DL). 26 Our retrospective study explored the optimal preoperative hemoglobin level for elderly hip fracture patients over 80 years of age and concluded that a preoperative hemoglobin level >10 g/DL might be associated with lower postoperative morbidity and mortality, which supported the results of the Gu and TRIFE studies.
One strength of our study is that it focuses on a subgroup of hip fracture patients over 80 years, who are the most vulnerable population of hip fracture patients and are at high risk of perioperative morbidity and mortality. Another strength of our study is that RCS was used to explore the optimal hemoglobin level for the group of patients. There are also some limitations in the study. First, it is a retrospective observational study. RCS and different statistical analyses were used to test the validity of the results. The subgroup of 80 years to 89 years confirmed the results and conclusions of the study. Second, a lower preoperative hemoglobin level of <10 g/DL was associated with more transfusions, and transfusions may be associated with some of the clinical outcomes.
Conclusions
In conclusion, for hip fracture patients over 80 years, a preoperative hemoglobin level of <10 g/DL was associated with an increase in postoperative MACEs, in-hospital mortality, and transfusion >2 U rate. Furthermore, we obtained the same results even after multivariable adjustment and subgroup analysis for hip fracture patients over 80 years. It is indicated that increasing the preoperative hemoglobin above 10 g/DL might lower the postoperative MACEs, in-hospital mortality and perioperative transfusion > 2U.
Footnotes
Acknowledgments
Thanks are owed to Cao Dongmei, the director of the medical record room for data collecting, and my family for support of my work.
Author Contributions
Data collection: M. Li and J. Shen, Statistical Analysis: C. Chen and L. Yang, Drafting of manuscript: C. Chen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Young talents Science and technology project of Changzhou Health Commission No. QN201925.