
Abstract
Introduction:
Based upon the Third National Health and Nutrition Examination Survey data, iron deficiency anemia is the cause of at least 20% of cases of anemia in adults over the age of 65. This is especially relevant in patients undergoing major orthopedic surgery as substantial perioperative blood loss is possible, leading to a high rate of allogeneic blood transfusion in total hip replacements, total knee replacements, and hip fracture repairs.
Significance:
The results of this systematic review may be of interest to clinicians and hospital administrators evaluating the clinical efficacy and cost effectiveness of intravenous (IV) iron administration prior to major orthopedic surgery.
Materials and Methods:
The original studies considered for this review included patients who were over 18 years of age, undergoing major orthopedic surgery, and who received an IV iron treatment in the preoperative setting. A total of 1083 articles were identified and reviewed. After removing duplicates, 1031 publications were screened, and 105 full-text studies were assessed for eligibility. A total of 98 were excluded and 7 articles remained which met the criteria for this review. The primary outcome examined in the included studies was the allogeneic blood transfusion rate. The secondary areas of interest were changes in serum hemoglobin, morbidity and mortality, length of stay, and cost effectiveness.
Results:
This systematic review found little evidence that IV iron therapy is effective at reducing transfusion in patients undergoing major orthopedic surgery.
Conclusions:
We do not recommend preoperative IV iron therapy for all patients scheduled for major orthopedic surgery.
Introduction
Preoperative anemia is common among patients undergoing major orthopedic surgery and can be found in up to 20% of patients. 1 Based upon the Third National Health and Nutrition Examination Survey data, iron deficiency anemia (IDA) is the cause of at least 20% of cases of anemia in adults over the age of 65. 2 Thus, optimization of patients’ iron stores preoperatively would be expected to resolve many cases of anemia. Preoperative anemia is associated with increased blood transfusion, health care costs, morbidity, and mortality. 3 -13 This is especially important in major orthopedic surgery as substantial perioperative blood loss is possible, leading to a high rate of allogeneic blood transfusion (ABT) in total hip replacements (25%-60%), total knee replacements (25%-50%), and hip fracture repairs (30%-70%). 14 -22 Blood transfusion has been associated with increased infection rates, longer hospital stays, and higher mortality with 1 study demonstrating a dose-dependent correlation between units of blood given intraoperatively and the incidence of complications after major surgery. 23 -25 Thus, it would be expected that ABT and the incidence of side effects could be reduced through the perioperative correction of IDA.
Iron deficiency anemia can be treated with either oral or intravenous (IV) replenishment of iron. Oral iron is inexpensive, but patient compliance is often poor due to gastrointestinal side effects and intestinal absorption may be limited. Intravenous iron raises hemoglobin (Hb) faster than oral iron, is more cost-effective than oral iron, and is well tolerated. 26,27 Indeed, serious adverse events have only been reported in 38 per 1 000 000 IV iron administrations with no known differences in safety between currently available formulations. An earlier formulation, high-molecular-weight iron dextran, was associated with a fatal anaphylactic reaction. This side effect has not been seen in the currently available formulations, but 0.5% of patients do experience a non-life-threatening, self-resolving complement-mediated “pseudo-allergy.” 28 Associated symptoms include arthralgia, myalgia, and flushing but no cardiovascular or respiratory effects. Intravenous iron can also be administered more quickly and conveniently than oral iron, often during a single clinic visit. For instance, up to 1000 mg of ferric carboxymaltoside (FCM) can be delivered in approximately 15 minutes. 28
The 2018 Frankfurt Conference consensus statement strongly recommends early detection and management of anemia before major elective surgeries with the use of iron supplementation for patients with IDA. 29 These guidelines also recommend that clinicians consider the addition of short-acting erythropoietins to treatment regimens for anemic patients scheduled for major orthopedic surgery but recommend against the use of erythropoiesis-stimulating agents. The British Society for Haemotology further recommends the administration of IV iron when IDA is diagnosed close to the day of surgery. 30 However, prior systematic reviews of preoperative IV iron administration have found inadequate evidence for the intervention due to a limited number of randomized controlled trials and low power in the studies that have been performed. 31 -33
Therefore, we performed a systematic review to evaluate the current evidence supporting IV iron administration as a preoperative treatment for anemia in patients undergoing major orthopedic surgery. We focused primarily on improvements in ABT rate and secondarily examined evidence for improvements in morbidity, mortality, length of stay (LOS), and the overall cost-effectiveness of the intervention. These results may be of interest to clinicians and hospital administrators evaluating the clinical efficacy and cost-effectiveness of IV iron administration prior to major orthopedic surgery.
Materials and Methods
Protocol and Registration
The protocol for this systematic review was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We enlisted the assistance of a research librarian and statistician in developing the protocol at Countway Library of Medicine, Boston, Massachusetts. The protocol was registered with international prospective register of systematic reviews (PROSPERO Application Number: 160872).
Eligibility Criteria
The original studies considered for this review included patients who were over 18 years of age, undergoing major orthopedic surgery, and who received an IV iron treatment in the preoperative setting. Review articles, published abstracts, letters to the editor, study protocols, and case reports were excluded from this systematic review. The study flow diagram and all exclusion criteria can be found in Figure 1.
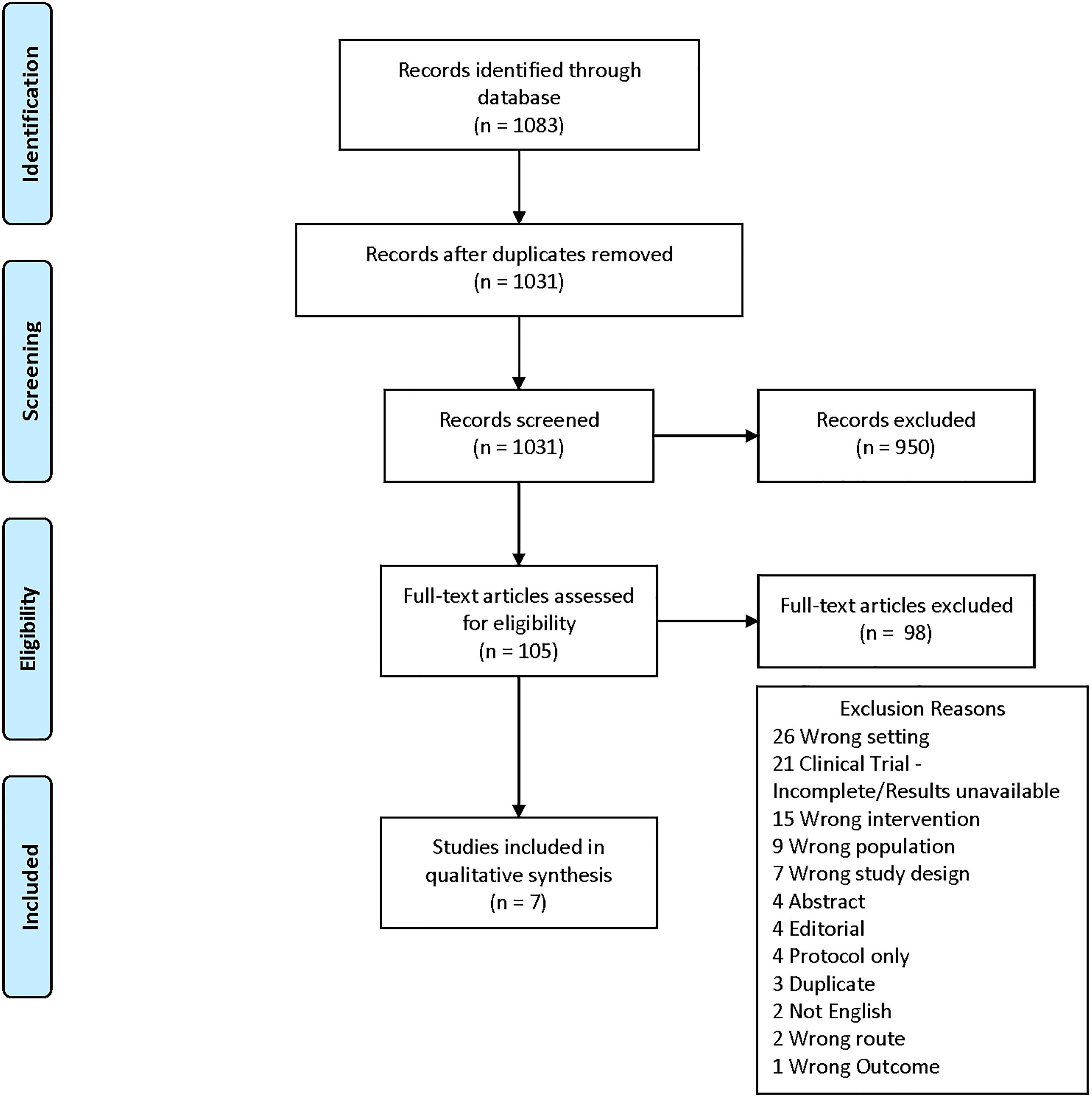
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram with exclusion criteria. Of the 1083 studies initially identified through the database search, only 7 were eventually included in the qualitative analysis.
Information Sources and Data Analysis
We searched several databases including PubMed, Cochrane, CLINAHL, WOS, and EMBASE on September 20, 2019 for all publications through September 2019. The search term list (see Appendix A) included the following terms: “anemia,” “hemoglobin,” “hematocrit,” “preoperative period,” “preoperative care,” “perioperative period,” “perioperative care,” “postoperative period,” “postoperative care,” “iron,” “iron compounds,” “hematinics,” “treatment outcome,” “outcome assessment,” “outcome and process assessment,” and “patient outcome assessment.”
The studies were independently identified and subsequently reviewed by 5 authors in 2 different phases. Results of the systematic review were collected and processed using Covidence software (Melbourne, Australia). 34 During the first phase, one author screened all titles and abstracts produced by the search criteria in the databases to determine eligibility. A second author read the full-text of each article that made it past the screening phase and independently decided if the publication should be included. After this, a third author evaluated the validity of reasons for the excluded articles. Disagreements were harmonized by consensus, and a final set of studies was chosen using the above methods. In the second phase, a qualitative analysis was performed instead of a meta-analysis due to the limited number of available studies. One reviewer extracted data and another verified the data. Extracted data included publication title, author(s), year of publication, location of publication, design of the study, population characteristics, intervention given to the patient population, comparator(s), and outcome results (Table 1).
Studies That Were Independently Identified and Subsequently Reviewed by the Authors Meeting the Search Criteria.

Abbreviations: ABT, allogeneic blood transfusion; AE, adverse event; EPO, erythropoietin; FCM, ferric carboxymaltose; Hb, hemoglobin; HF, hip fracture; IV, intravenous; IU, international units; LOS, length of stay; PHF, pertrochanteric hip fracture; PNI, postoperative nosocomial infections(s); QoL, quality of life; RBC, red blood cell; sTfR, soluble transferrin receptor; SHF, subcapital hip fracture; THR, total hip replacement; TKR, total knee replacement.
Outcomes
The primary outcome examined in the included studies was ABT rate. The secondary outcomes were changes in serum Hb, morbidity and mortality, LOS, and cost effectiveness.
Quality Assessment
The quality and risk of bias for the 4 randomized and 3 non-randomized studies were assessed with the Cochrane Risk Assessment tool and Newcastle-Ottawa Scale (NOS), respectively. 35,36 The Cochrane Risk Assessment tool assesses bias in randomized studies by assigning a rank of “high,” “low,” or “unclear” in 5 subcategories. 35 Subcategories include selection bias which is evaluated on random sequence generation and allocation concealment; reporting bias which is evaluated on selective reporting; performance bias which is evaluated on blinding of participants and personnel; detection bias which is evaluated on blinding of outcome assessment; attrition bias which is evaluated on incomplete outcome data; and other sources of bias. Study quality was defined as “good” if the study had no “high” ratings for risk of bias. Study quality was defined as “fair” if the study had 1 to 2 “high” ratings for bias. Study quality was defined as “poor” if the study had 3 or more “high” ratings.
The NOS is used as a tool to assess the quality of non-randomized studies using a scoring system that rates studies based on selection, comparability, and outcome. 36 Study quality is defined as “good” if the study scored in the ranges of 3 to 4 for selection, 1 to 2 for comparability, and 2 to 3 for outcome. Study quality was defined as “fair” if the study scored 2 for selection, 1 to 2 for comparability, and 2 to 3 for outcome. Study quality was defined as “poor” if the score did not meet criteria for either “good” or “fair.”
Results
Literature Search
A total of 1083 articles were identified and reviewed. After removing duplicates, 1031 publications were screened, and 105 full-text studies were assessed for eligibility. A total of 98 were excluded, and 7 articles remained which met the criteria for this review.
Study Characteristics
All of the studies in this systematic review included cohorts of patients undergoing major orthopedic surgery, with at least some anemic patients included in each study. A total of 7 studies were included. The studies involved a total of 3965 patients. All but one of the studies had ABT requirements as either a primary or secondary outcome. Preoperative Hb was the primary outcome in Biboulet et al. Four of the studies were conducted in Spain, 1 in France, 1 in the United Kingdom, and 1 in Austria. The design of the studies included 3 randomized and blinded studies. One randomized nonblinded study, 1 non-randomized non-blinded study, and 2 observational studies. All 7 studies included subjects receiving lower limb orthopedic surgery. Bernabeu-Wittel et al, Cuenca et al, Moppett et al, and Serrano-Trenas et al each included only hip fracture repair patients. Biboulet et al and Heschl et al included total hip replacement and total knee replacement patients. Munoz et al was the most inclusive with subjects receiving total hip replacement, total knee replacement, or hip fracture repair.
Quality of Included Studies and Risk for Bias
The grading schemes for the randomized and non-randomized studies are specified in Tables 2 and 3, respectively. Four articles were good quality, and 3 articles were poor quality. The poor-quality publications were ranked as such due to a lack of multivariate analyses and a lack of comparability between cohorts in the studies utilizing retrospective cohorts. The 4 articles of good quality had a low risk of bias.
Cochrane Risk of Bias Tool for Randomized Studies.

Newcastle Ottawa Scale for Non-Randomized Studies.

Abbreviations: ABT, allogeneic blood transfusion; DSHF, displaced subcapital hip fracture; Hb, hemoglobin; LOS, length of stay.
Definitions and Measures
The presence of anemia in subjects varied between studies. Bernabeu-Wittel et al included only patients with Hb between 9 and 12 g/dL. Biboulet et al included patients with Hb between 10 and 12.9 g/dL. Cuenca et al, Heschl et al, Moppett et al, and Serrano-Trenas et al did not utilize Hb to include or exclude patients from their studies. Munoz et al excluded patients with Hb < 10 g/dL due to the high risk of preoperative transfusion in that subset of patients.
Association of Iron Therapy and Transfusion Frequency
All but 1 of the 7 studies looked at transfusion frequency or units transfused per patient as an outcome. Although it was not one of their study’s outcomes, Biboulet et al did report this information. None of the 4 good-quality studies found a significant improvement in these metrics overall. Conversely, all 3 poor-quality studies did find significant improvement.
Bernabeu-Wittel et al found a high overall transfusion frequency with 52.5% of patients receiving at least 1 transfusion. 37 They found no significant reduction in transfusion frequencies or transfusions per patient in the IV FCM with erythropoietin (EPO) cohort relative to the control cohort. Overall, transfusion was required in 52% of patients in the FCM with EPO group, in 54% of patients in the FCM group, and in 56% of patients in the control group. The mean number of RBC transfusions per patient was 1.17 in the FCM with EPO group, 1.32 in the FCM only group, and 1.29 in the control group.
Biboulet et al found a very low transfusion frequency overall and found no significant reduction in transfusion frequency or mean units received. 38 Only 2% of patients in the IV FCM arm received ABT, while 6% of patients in the oral iron arm received ABT. The mean number of RBC units transfused per patient was 0.06 and 0.12, respectively.
Moppett et al found no significant reduction in ABT frequency between the group receiving IV iron sucrose and the control cohort. 39 A total of 28% of patients receiving IV iron sucrose were transfused while 29% of control patients were transfused. The mean number of units transfused was not reported in this study.
The other good-quality study, Serrano-Trenas et al, found no significant reduction in postoperative transfusion frequency between the cohort receiving IV iron sucrose and the control cohort. 40 Overall, transfusion was required in 33.3% of iron sucrose patients and 41.3% of control patients. They also analyzed transfusion requirements in smaller patient subsets and found that IV iron did significantly reduce the frequency of ABT in patients with an admission Hb ≥ 12 g/dL (18.3% vs 36%) or with intracapsular hip fracture (14.3% vs 45.7%).
Cuenca et al found no significant change in overall transfusion frequency between a prospective cohort receiving IV iron sucrose and a retrospective control cohort. 23 Overall, 15% of patients receiving IV iron received transfusions compared to 36.8% of control patients. However, Cuenca et al did find a significant effect on mean RBC units transfused per patient. The IV iron cohort received a mean of 0.26 units per patient while the control cohort received a mean of 0.77 units per patient.
Heschl et al compared patients managed by a preoperative preparation protocol (PREP) to similar patients who were not managed on protocol (NOP) who were identified by propensity score matching. 41 Preoperative preparation protocol patients received 2 doses of 1 g IV FCM and patients meeting anemia of chronic disease criteria received EPO. The authors also found a significant reduction in ABT frequency and mean RBC units transfused per patient when comparing PREP to NOP patients. A total of 12% of PREP patients were transfused (mean of 0.2 units of RBCs per patient) and 24% of NOP patients were transfused (mean of 0.5 units of RBCs per patient).
Munoz et al found a significant reduction in ABT rates between a retrospective cohort receiving IV iron ± EPO and a retrospective control cohort. 1 Significance was maintained for pertrochanteric hip fracture (PHF) repair, total hip replacement, and total knee replacement. The mean number of units per patient was also significantly reduced in each of these categories. Of note, neither transfusion rates nor units transfused per patient were significantly changed in patients undergoing subcapital hip fracture repair (SHF). Of PHF patients receiving IV iron, 38.4% were transfused (mean of 0.9 units per patient), while 59.8% of controls were transfused (mean of 1.5 units per patient). Of SHF patients receiving IV iron, 27.6% were transfused (mean of 0.6 units per patient), while 32.7% of controls were transfused (mean of 0.8 units per patient). Of total hip replacement patients receiving IV iron, 16.7% were transfused (mean of 0.3 unit per patient), while 34.4% of controls were transfused (mean of 0.8 units per patient). Of TKR patients receiving IV iron, 6.2% were transfused (mean of 0.1 units per patient), while 24.0% of controls were transfused (mean of 0.5 units per patient).
Association of Iron Therapy and Hb Levels
As most of these studies involved emergent surgery, there was often insufficient follow-up time to track improvement of serum Hb prior to surgery. Only 2 of the included studies had an extensive preoperative preparatory period for anemia treatment and reported this information. 38,41 However, all of the studies tracked postoperative serum Hb levels. Only 2 of the 4 good-quality studies and 1 of the 3 poor-quality studies found significantly increased Hb with IV iron supplementation.
Bernabeu-Wittel et al reported a significant improvement in discharge and 60-day post-discharge Hb levels in the EPO with FCM cohort. 37 Discharge Hb was 10.24 g/dL in the EPO with FCM cohort, 10.0 g/dL in the FCM only cohort, and 9.67 g/dL in the control cohort. The 60-day post-discharge Hb was 12.46 g/dL in the EPO with FCM cohort, 12.34 g/dL in the FCM only cohort, and 12.0 g/dL in the control cohort. Although the difference was nonsignificant, intra-cohort Hb differences first began to appear 72 hours postoperatively. At that time, Hb in the EPO with FCM cohort was 9.37 g/dL, FCM-only Hb is 9.23 g/dL, and the control cohort Hb was 9.11 g/dL.
Biboulet et al measured baseline Hb, preoperative Hb, and postoperative Hb at days 1, 3, and 5. 38 They reported a significant improvement in Hb in the IV iron group versus the oral iron group at each time point. Mean preoperative Hb improved from 12.2 to 14.9 g/dL in the IV iron group and from 12.3 to 13.9 g/dL in the oral iron group. The mean postoperative Hb continued this trend at day 1 (12.6 vs 12.2 g/dL), day 3 (12.6 vs 11.6 g/dL), and day 5 (13.4 vs 12.3 g/dL). Preoperative ferritin also increased significantly in the IV iron group (from 145 to 325 μg/L) and declined in the oral iron group (from 138 to 64.5 μg/L).
Moppett et al measured daily Hb from admission until 7 days after surgery. 39 They found no significant difference in Hb at any point during the study. The mean admission Hb was slightly lower in the IV iron sucrose arm at 12.24 versus 12.54 g/dL in the control arm patients. This difference continued at day 1 (11.11 vs 11.27 g/dL) but reversed by day 7 (10.32 vs 10.09 g/dL). However, reticulocytosis was significantly increased with IV iron sucrose administration. The day 7 mean reticulocyte count was 91.2 × 109 cells/L in the IV iron sucrose group and 75.8 × 109 cells/L in the control group.
Serrano-Trenas et al measured hematocrit at admission, 24 hours postoperatively, and at 7 days postoperatively. 40 They found no significant differences between the IV iron cohort and the control cohort. From admission to 7 days postoperatively, the IV iron group mean hematocrit dropped from 36.8% to 31.6% while the control cohort mean hematocrit dropped from 36.4% to 30.8%.
Cuenca et al measured serum Hb preoperatively and at postoperative day 2 and found no significant differences between cohorts. 23 Overall, they found an equivalent preoperative mean Hb of 10.7 g/dL and found that by postoperative day 2, this dropped to a mean of 9.6 g/dL in the IV iron group and 10.1 g/dL in the control group.
Heschl et al measured Hb at a preoperative visit, on the day of surgery, and at hospital discharge. 41 Mean Hb at the preoperative visit was significantly higher in the PREP group (13.3 g/dL) compared to the NOP group (12.9 g/dL). This reversed on the day of surgery as the PREP group had transitioned to having significantly lower serum Hb (12.2 g/dL) than the NOP group (12.9 g/dL). This was due to a 1.1 g/dL decline in mean Hb in the PREP group as mean Hb was stable between measurements in the NOP group. Discharge Hb was not significantly different between groups. The PREP group had a serum Hb of 10.7 g/dL, while the NOP group had a Hb of 10.6 g/dL.
Munoz et al measured Hb at admission through postoperative day 7. 1 At postoperative day 7, serum Hb was significantly reduced in the IV iron ± EPO cohort compared to the control cohort after PHF repair (10.5 vs 10.8 g/dL) or SHF repair (10.1 vs 10.5 g/dL). In contrast, the same analysis on the total hip replacement subgroup showed a significant improvement (10.7 g/dL vs. 10.1 g/dL), and no significant difference was seen with total knee replacement (10.1 vs 10.3 g/dL).
Association of Iron Therapy and Morbidity and Mortality
All 7 of the studies examined the association between iron therapy and a variety of measures of morbidity and mortality. None of the 4 good-quality studies found significant differences, but 2 of 3 poor-quality studies found improvements in mortality with IV iron administration.
Bernabeu-Wittel et al measured survival at discharge and 60 days and tracked health-related quality of life with a standardized survey at baseline and 60 days post-discharge. 37 They also tracked readmissions and serious adverse events. They found no significant differences between groups with any of these measures. Biboulet et al measured preoperative fatigue and physical fitness and tracked major complications through postoperative day 30. 38 Preoperative fatigue and fitness levels were not significantly different between study arms and no major complications were identified in either study arm. However, 1 patient in the IV iron group developed deep venous thrombosis at postoperative day 7. Moppett et al tracked cardiovascular complications, infectious complications, and 30-day mortality and found no significant differences between groups. 39 In absolute terms, IV iron receiving patients experienced a similar percentage of cardiovascular complications (9% vs 10%), reduced infectious complications (21% vs 29%), and increased 30-day mortality (10% vs 0%). Serrano-Trenas et al measured 30-day mortality, infection rates, and serious adverse events. 40 No significant differences between groups were observed.
Cuenca et al measured infection rates and 30-day mortality. 23 They found no significant change in infection rates but did report a significant decrease in 30-day mortality. A total of 15% of the IV iron cohort experienced infection and none died during the study period, while 33.3% of the control cohort experienced infection and 19.3% died during the study period. Heschl et al measured survival over several years in their retrospective cohorts and found very high overall survival (>95%) with no significant difference between groups. 41 Munoz et al tracked the frequency of postoperative infection and 30-day mortality. 1 They found that IV iron ± EPO treatment was associated with a significant reduction in postoperative infection for patients undergoing PHF repair (15.3% vs 28.9%) or SHF repair (7% vs 23.8%) but had no significant association for total hip replacement (3.8% vs 4.4%) or total knee replacement (2.5% vs 2.8%). These infections were predominantly urinary tract infections. Mortality was significantly reduced in the IV iron ± EPO cohort for patients undergoing SHF repair (2.9% vs 7.5%) while no significant association was seen for the PHF cohorts (7.2% vs 10.7%). Munoz et al additionally found that receiving ABT was associated with a significantly increased risk of postoperative infection for hip fracture repair patients. For patients receiving ABT, postoperative infection occurred in 17.9% of the IV iron ± EPO cohort and 34.7% of controls. For patients that did not receive ABT, postoperative infection occurred in 7.2% of the IV iron ± EPO cohort and 19.5% of controls. The 30-day mortality was also reduced in the IV iron ± EPO cohort, but this reduction was only significant for the subgroup that did not receive ABT. For this subgroup, the IV iron ± EPO cohort had a mortality of 2.8% while the control cohort had a mortality of 7.0%. For the ABT-receiving subgroup the IV iron ± EPO cohort had a mortality of 8.9% and the control cohort had a mortality of 11.9%.
Association of Iron Therapy and LOS
None of the studies directly evaluated the economic implications of iron therapy as an outcome. A related outcome, LOS, was examined by 5 of the 7 studies. Two of the good-quality studies reported this outcome and found no significant difference. The 3 poor-quality studies each reported a significant reduction in mean LOS with IV iron therapy. Moppett et al found no significant difference in LOS between the IV iron (13.4 days) and control (14.2 days) groups. 39 Serrano-Trenas et al also found no significant difference in LOS between the IV iron (13.5 days) and control (13.1 days) groups. 40 Cuenca et al found that their IV iron group had significantly shorter LOS than their control group (11.9 days vs 14.1 days). 23 Heschl et al also reports a significantly reduced mean LOS in their PREP patients compared to NOP patients. 41 The overall LOS between the 2 arms was quite similar, however, at 15.1 and 15.4 days, respectively. Munoz et al found that IV iron ± EPO was associated with significantly reduced LOS for the PHF repair (12.6 vs 13.9 days), SHF repair (11.3 vs 12.7 days), and total knee replacement patients (8.5 vs 13.0 days). 1 They found no significant difference from this intervention for total hip replacement patients (8.1 vs 8.9 days).
Discussion
Our systematic review is the most recent and comprehensive on this topic but was limited in number with only 7 articles—4 that were good quality and 3 that were poor quality. Our goal was to determine whether preoperative IV iron for anemic patients undergoing major orthopedic surgery could improve clinical outcomes or reduce costs. These studies do not provide consistent evidence of a reduced incidence of ABT or reduced costs with IV iron administration. Therefore, we cannot recommend preoperative IV iron as a standard intervention in anemic patients scheduled for major orthopedic surgery.
The best evidence for improved clinical outcomes with preoperative IV iron therapy comes from Cuenca et al and Munoz et al, who each showed significant reductions in transfusion rate, postoperative infection, mortality, and LOS. 1,23 Heschl et al reported similar findings with a reduced transfusion rate and decreased LOS. 41 These 3 studies were all poor quality and at least partially retrospective. Overall, their results contrasted sharply with the 4 randomized, controlled trials, none of which found significant differences in ABT, infection, mortality, or LOS. Due to the urgent nature of the planned procedures in many of these studies, there was little time for preoperative optimization of anemia and IV iron was typically given within a few days of the planned operation. This did not allow for sufficient time to observe preoperative improvements in anemia. Postoperative Hb was followed in many of the studies for at least a week and was typically not significantly changed by IV iron therapy.
There are several potential reasons for heterogeneity between the studies. Bernabeu-Wittel et al was the largest randomized controlled trial, limited their analysis to anemic patients, and tracked postoperative outcomes out to 60 days, all of which were key to answering our study question. 37 However, this study focused on hip fracture repair which reduces the preoperative time to treat anemia. Overall, based upon experimental design and cohort sizes, this was likely the most reliable study found in this systematic review. The high overall frequency of ABT should also improve the likelihood of a clinically significant effect being observed. Unfortunately, the lack of a significant effect seen for ABT, postoperative infection, mortality, and LOS greatly reduced the likelihood that very near preoperative IV iron or IV iron and EPO improved outcomes in a clinically meaningful way. However, there was a small trend toward reduced frequency and volume of ABT in the groups receiving IV FCM, with the IV FCM with EPO group having the lowest frequency and volume. Additionally, the 60-day follow-up did show that the iron intervention successfully treated the anemia and significantly improved levels of Hb, with the IV FCM with EPO group once again having the largest improvement. Thus, a much larger study may have successfully shown a reduced incidence of ABT, although any effect size would likely be small.
Biboulet et al is the only randomized controlled trial that included anemic patients scheduled for elective surgery rather than hip fracture repair. 38 This allowed for lengthy preoperative treatment of anemia and evaluation of preoperative improvement in Hb. In this study, IV iron significantly increases preoperative Hb compared to oral iron, and the absolute frequency and volume of transfusions were decreased. However, the small cohort sizes, low overall incidence of ABT, and lack of complications in this patient population at this hospital make it difficult to determine any clinical benefit from IV iron therapy. Future studies with this experimental design and larger patient cohorts would be helpful for evaluating the clinical effectiveness of preoperative IV iron administration for the treatment of anemia in patients undergoing major orthopedic surgery.
Moppett et al is a smaller, randomized controlled trial that did not focus solely on anemic patients, tracked Hb until postoperative day 7, and focused on hip fracture repair patients. 39 No significant effect is seen on Hb, but there is a trend toward improvement with IV iron treatment and the increased reticulocytosis seen in the IV iron cohort is consistent with some efficacy. However, no effect is seen on transfusion frequency. This is consistent with the findings in Bernabeu-Wittel et al.
The design of Serrano-Trenas et al is similar to Moppett et al’s but includes about 2.5 times more patients. 40 They found no significant effect on ABT, postoperative infection, mortality, or LOS. Once again, the absolute frequency and volume of transfusions was decreased in the IV iron group, so increased subject enrollment may have yielded a statistically significant result.
Cuenca et al also focused on patients undergoing hip fracture repair but utilized a retrospective control cohort rather than a randomized study design. 23 The retrospective control cohort and lack of multivariate analysis limits the conclusions that can be drawn from this study. There was also some evidence that the criteria for transfusion differed between the 2 arms of the study as the difference in mean postoperative Hb between the 2 cohorts (0.5 g/dL) was similar to the difference in mean units transfused (0.5 units per patient). Thus, differences in transfusion rates could be due to changes in transfusion criteria or decision-making in the prospective cohort. Additionally, the very high rate of postoperative mortality (19.3%) in the retrospective control cohort is concerning. As 2 similar studies have been performed with improved designs and have failed to show significant benefit, it is unlikely that the positive results in this study were solely due to the administration of IV iron.
Heschl et al was similar to Biboulet et al as they focused fully on elective surgeries and aimed to correct anemia preoperatively rather than to simply provide additional IV iron just prior to surgery. 41 Unlike Biboulet et al, this study is retrospective which limits the conclusions that can be made. All patients at this site should have been allocated to a PREP if found to be anemic. Depending on the type of anemia, they were to be treated with IV iron and sometimes EPO. The patients that were appropriately allocated are the experimental group and propensity score matching was used to identify appropriate controls who should have been allocated but were not. Unfortunately, matching could not overcome the differences between these cohorts as there remained significant differences in preoperative Hb, American Society of Anesthesiologists physical status, age, body mass index, New York Heart Association heart failure classification, and the incidence of diabetes. Thus, although ABT frequency and units transfused were both halved, it is difficult to draw any conclusions from this study. However, these results are consistent with the findings in Biboulet et al, which is supportive of their validity.
Munoz et al was the largest study with over 2000 subjects from 4 different hospitals and included 4 different surgeries. 1 The difference between the retrospective cohorts in this study was whether the patient received IV iron just prior to surgery. In this study, IV iron administration was associated with an improvement in several clinically important outcomes, but the retrospective design and lack of multivariate analysis limit possible conclusions. However, based on the negative results seen in the prospective randomized controlled studies, it is unlikely that the effect sizes seen in this study were solely due to the intervention.
Overall, these studies provide little evidence of consistent, significant clinical benefit from IV iron administration in the immediate preoperative period. Possibly due to the short follow-up of Hb levels in many of the studies, there is also little evidence of significant improvement in serum Hb with immediate preoperative IV iron administration. However, studies including longer follow-up times after IV iron administration do show consistent improvement in Hb with this intervention. This increase in Hb would be expected to result in a reduced incidence of ABT given sufficient time for patient response. However, these studies do not definitively demonstrate this outcome. Thus, more research is necessary to determine whether preoperative IV iron reduces the need for ABT in major orthopedic surgery.
Cost savings was not a measured outcome in these studies, which limits our ability to make any conclusions about this outcome. The reduction in ABT rate, LOS, and morbidity and mortality seen in the retrospective trials would be consistent with cost savings. However, none of the randomized controlled trials demonstrates a clinically significant effect from this intervention, reducing the likelihood that this approach will reduce costs. Additionally, based on increased costs of €390 per patient, detailed in Biboulet et al, implementation of preoperative IV iron administration may increase costs.
These findings are similar to those reported in the recent meta-analysis by Shin et al. 42 In that review, they focus on perioperative administration of IV iron, while this review only included studies with preoperative IV iron administration. Even with this difference, they still find no support for the administration of IV iron from randomized controlled trials. More large randomized controlled trials are needed to definitively answer this question.
Strengths and Limitations
This systematic review has several strengths. We performed a comprehensive search with broad search terms, enlisted methodological expertise, and did not limit the search to elective surgeries or by time frame. We assessed quality using the Cochrane Risk of Bias Tool and the NOS Assessment of Study Quality. Our review is currently the most recent and comprehensive on this topic.
One of the biggest limitations of our review is the lack of publications investigating IV iron therapy as a preoperative intervention for anemic patients scheduled for major orthopedic surgery. We were only able to identify 7 studies that met our inclusion and exclusion criteria. Of these studies, 4 of the 7 were good quality based on our quality assessment and risk of bias scores, and 3 were poor quality. Results were reported on all studies despite the quality. Nevertheless, strong conclusions could not be drawn from these 7 studies. Many of these studies did not focus on anemic patients, and there was typically minimal time between IV iron administration and surgery. Thus, the anemic patients that were included in many of these studies likely did not have sufficient time to begin recovering from anemia due to this intervention. Lastly, some of the included studies had results that trended toward an effect, so in some cases, the lack of significance may have been due to insufficient power.
Conclusion
In this systematic review, we found little evidence that preoperative IV iron therapy is effective in improving clinical outcomes in patients undergoing major orthopedic surgery. Due to the limited number of randomized controlled studies that met our inclusion criteria, we were unable to conduct a meta-analysis to identify the definitive effect of IV iron therapy on transfusion rates and recovery. From the studies that have been done, there is a trend toward a small improvement in transfusion frequency in patients treated with IV iron, but this effect is nonsignificant in the randomized controlled trials. Thus, we cannot recommend IV iron supplementation for all major orthopedic surgery patients in the preoperative period to reduce the incidence of ABT. However, for patients with known IDA, we still recommend the preoperative treatment of anemia with iron supplementation. Future efforts should be focused on conducting large, prospective, randomized controlled trials to confirm the efficacy of this intervention in preventing ABT, improving postoperative outcomes, and curtailing costs.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.