
Abstract
Background
Humeral shaft fractures occur frequently in older patients. The more proximal end of the shaft is prone to non-union when compared with more distal fractures. We provide an overview of several key features of this significant patient group.
Method
Our institutional fracture database was searched for all cases of proximal third humeral shaft fractures in patients over 60 years of age. Retrospective evaluation of patient demographics, management, length of stay and incidence of non-union was performed.
Results
75 patients (61 female) were analysed. 33 patients were ‘frail’ (Clinical Frailty Scores of >4). Non-union occurred in 19 of 45 non-surgically treated fractures and in 1 of 37 cases treated surgically. Mean length of stay was 5.9 days (non-operative) and 6.6 days (operative). Proximal extension into the humeral head is common.
Conclusion
Non-surgical management of proximal third humeral shaft fractures is associated with an increased risk of non-union. We detail an operative technique and case example supporting early fixation of displaced proximal third humeral shaft fractures in older patients that can be utilized for both primary and delayed fixation. In view of the significant association of non-union a well-constructed prospective cohort study with outcome assessment would be of value to further characterize this emerging injury population.
Introduction
Injuries to frail and older people are increasing, with considerable impact on them, their carers and the health service in which they are treated.1,2 These patients and their fractures have different personalities to higher-energy transfer trauma and their management pathway should reflect this. Retaining independence can aid recovery and reduce demand on health services and carers amongst other benefits. 3 In patients of a similar age with hip fractures, non-surgical management is very rare although with fractures of the upper arm, the converse is the norm. 4
Older patients may be reliant on appliances to walk, and any upper limb injury can cause considerable reduction in confidence and independence. 5 In the United Kingdom, the best practice tariff (BPT) was introduced to incentivize hip fracture care and reduce the sequelae of immobility and independence loss. Improved clinical outcomes and sizable cost savings to the NHS have resulted. 6 Upper limb fractures will inevitably increase in the ageing population and the care afforded to patients with these injuries should parallel those afforded to patients with hip fractures.
Fractures in the proximal third of the humeral shaft are prone to non-union (with rates reported as high as 54%), 7 especially with non-operative management.4,8-12 This contrasts with less contemporary studies of predominantly younger patients.13,14 Furthermore, advancing age and glenohumeral osteoarthritis have been highlighted as risk factors for non-union with non-operative treatment of humeral shaft fractures.10,15 Secondary surgery for non-union is associated with inferior functional outcomes, more pain on activity and incomplete recovery.16,17 Debate therefore surrounds the primary treatment method for displaced proximal third humeral shaft fractures in older patients.
In 2020, Oliver et al. 18 investigated the changing demographic of humeral shaft fractures and proposed that proximal third humeral shaft fractures should be considered fragility fractures due to their occurrence in older, female patients following low-energy trauma and secondly, that their incidence was increasing.
Our primary aim is to add to the evidence by providing a focused study of displaced, proximal third humeral shaft fractures in patients over 60 years of age. Our secondary aims are to review rates of union, assess the degree of clinical frailty in this cohort, and the impact on length of in-patient hospital stay. This information will help surgeons when deciding on optimum care with their patients and will help design more definitive investigation of this important injury population.
Method
A retrospective review of the radiological records from an institutional database of all patients over 60 years sustaining proximal third humeral shaft fractures from January 2012 to end of December 2017 (6 years) was performed using Picture Archiving and Communication System, (PACS).
Radiographs were screened and fractures were not considered proximal third humeral shaft if: - Fracture entirely distal to the proximal-to-middle third junction of humeral shaft - Fracture entirely within the proximal Muller square (A square whose sides are the same length as the widest part of the epiphysis) ie. proximal humeral, non-diaphyseal fractures. - Segmental fracture that was not contained entirely within the proximal one-third of the humeral shaft.
Serial radiographs were examined by two senior reviewers. Radiological and case records were analysed for demographics, length of stay, Rockwood Clinical Frailty Scale score, 19 and fracture pattern as defined by the AO/OTA Classification (Arbeitsgemeinshaft fur Osteosynthesefragen/Orthopaedic Trauma Association). Serial radiographs and operative records were used to assess outcomes including treatment method, evidence of union, and time to union. Patients excluded were those less than 60 years old at presentation, pathological fractures, open fractures, peri-prosthetic fractures and those with multiple injuries.
Non-union was defined as the lack of bridging callus on at least two cortices on orthogonal radiographs at 9 months post injury and no progression over 3-month period. Requirement for delayed surgical fixation indicating failed non-operative treatment was also assessed.
Primary operative intervention was undertaken when fractures had displacement of more than cortical width or any angulation. Angulation was either present or not and was not routinely measured as is the case when analysing displaced intracapsular neck of femur fractures. A displaced and/or angulated proximal third humeral shaft fracture represents a less stable injury, prompting a move towards advising surgical fixation.
Surgical Technique
The majority of patients undergoing surgery (29) had plate fixation. 8 were fixed with having intramedullary nailing.
Plate fixation was with a Proximal Humeral Internal Locking System (PHILOS) LCP plate (DePuy Synthes) as almost all fractures extend proximally into the greater tuberosity and this device can achieve good proximal fixation. Plate lengths depended on each patient’s humeral length and fracture but aimed to have a least three screws (6 cortices) distal to the fracture. Surgery was performed by the senior author or by trainees under his direct supervision.
Patients are positioned in the semi beach chair position with image intensifier coming in from the opposite side. The affected arm should be able to move into full extension free from the edge of the operating table. It is important to check prior to starting that it is possible to obtain antero-posterior and lateral views of the entire humeral shaft, and glenohumeral antero-posterior and axillary lateral views of the shoulder joint.
The surgical approach is anterior, employing the deltopectoral interval proximally and splitting brachialis anteriorly as far distally as required. The position of the radial nerve must be considered during fracture reduction. The anterior deltoid insertion is released by sharp dissection to allow correct placement of plate. The fracture haematoma is removed, and the appropriate plate applied after demonstrating that humerus can be reduced with restoration of length, alignment, and rotation.
Occasionally 3.5/2.7 mm screws are used to obtain temporary reduction of the humeral shaft prior to plate application and occasionally 2 mm K-wires employed. A minimum of five 3.5 mm locking screws are used in the humeral head, positioned divergently into the subchondral bone without drill or screw joint penetration, and at least three bi-cortical locking screws distal to the diaphyseal fracture element.
The fracture line frequently extends proximally into the humeral head at the greater tuberosity and is often undisplaced. Some fractures are unstable proximally with involvement of the surgical neck, and when displaced a 2/0 Fiberwire (Arthrex) is passed through the plate proximally, then as a cerclage suture around the rotator cuff tendons and then back through the plate. The senior author has found this neutralises the deforming forces of the rotator cuff and considerably reduces varus displacement, and subsequent fixation failure postoperatively.
A sling is worn for comfort and active elbow range of movement exercises begin on the first day postoperatively along with shoulder pendular exercises. The sling is removed when the patient has good elbow control, normally within a couple of days of surgery.
A wound check and radiographic assessment is undertaken at 2 weeks following surgery. Outpatient physiotherapy is arranged, and further follow up at 6 weeks, 3 months, 6 months and approximately 1 year with interval x-rays
Results
Basic Demographics of Proximal Third Humerus Fractures in Operative and Non-Operative Groups in the Over 60 s.

*DMARDs = Disease-modifying anti-rheumatic drugs.
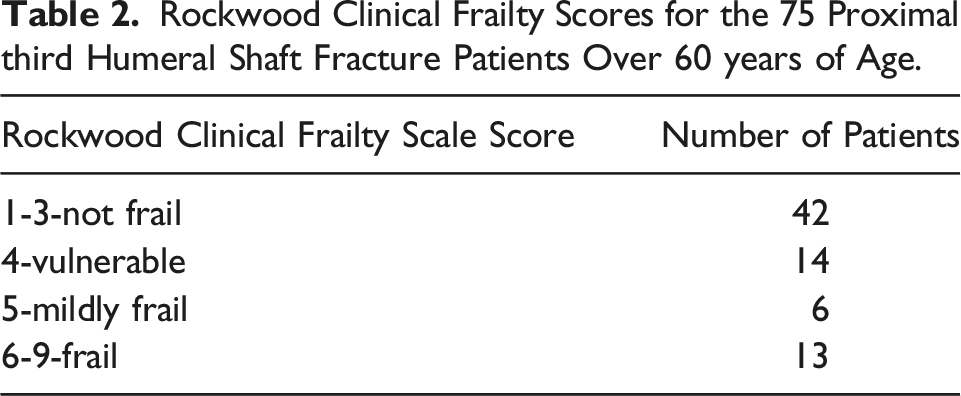
Rockwood Clinical Frailty Scores for the 75 Proximal third Humeral Shaft Fracture Patients Over 60 years of Age.
Comparing Operative vs Non-Operative Management Non-Unions, Time to Union (in those that United) & Length of Stay in Proximal Third Humeral Shaft Fractures in the Over 60 s.

Non-Operative and Operative Proximal Third Humeral Shaft Fractures and Non-Unions in the Over 60 s by AO/OTA Classification Subgroups.

30 patients had their fracture fixed primarily and 7 fractures had delayed fixation with mean time to surgery 122 days. Twenty-nine fractures were treated with open reduction internal fixation with a plate and locking screws, 8 with an intra-medullary nail with proximal and distal locking. 36 of 37 fractures united in the operative group; 8 of the 8 treated with locked intra-medullary nail and 28 of the 29 treated with plating. There were no instances of nerve injury, deep infection, or peri-prosthetic fracture (Figure 1). Percentage of proximal third humeral shaft fractures by AO/OTA classification.
Case 1–Delayed Fixation of Symptomatic Non-Union Following 8 months Non-Operative Management
Left-hand dominant 73-year-old lady, with a Clinical Frailty Score of four, injured her left humerus following a fall in her kitchen. Radiographs showed an AO/OTA 12B3a fracture. Of note, this is not a multi-fragmentary, type C fracture, as if it were to be reduced, there would be contact between part of the most proximal and distal segments. She was managed non-operatively but continued to experience pain at 8 months follow-up and no radiological evidence of union and her function and range of motion was limited (shoulder elevation to 70°).
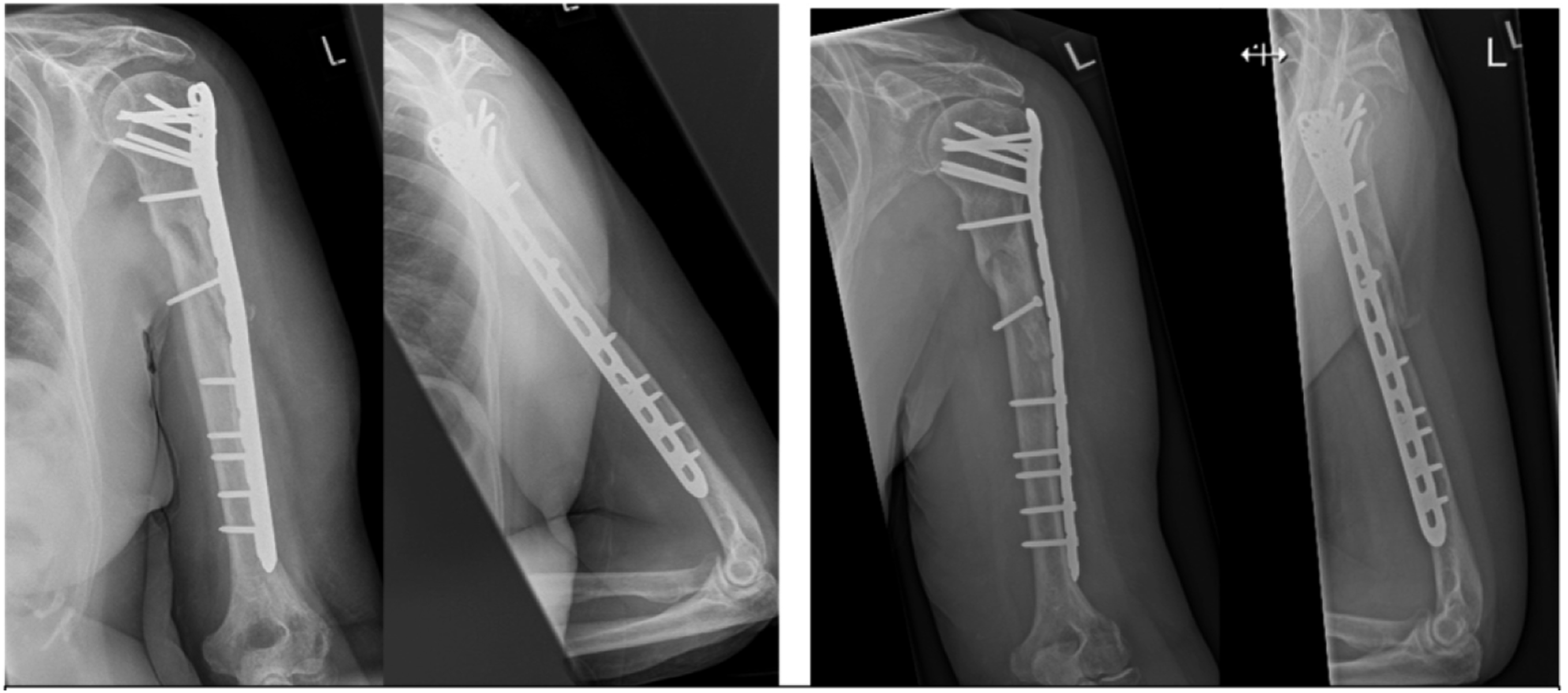
Surgical debridement of her non-union with plating was performed and at final follow-up 10 months post-operatively the fracture was united, both clinically and radiologically, with excellent range of motion of the shoulder (Figures 2-5 and 6-9). AP and scapula Y views of case 1 at presentation and following 8 months. AP and scapula Y views of case 1 at 4 weeks post-surgery and then at final.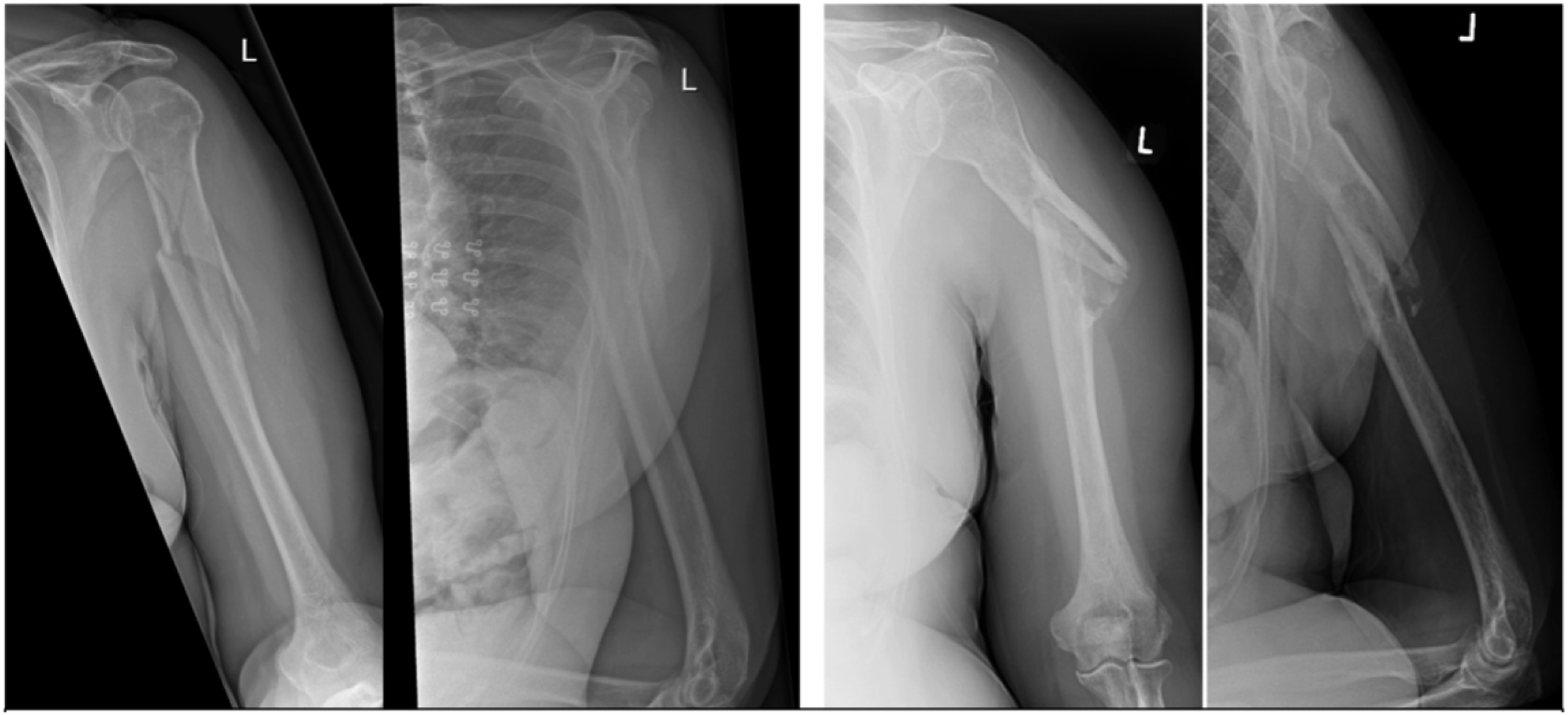
Discussion
The proximal third humeral shaft fracture in the older patient has been highlighted in ‘whole humeral’ series as being less likely to heal and should be considered for fixation. 4 The literature specific to this injury pattern is, however, sparse. We report a series of 75 proximal third humeral shaft fractures in patients over 60 years of age and corroborate a trend towards non-union with non-operative management. Surgery by contrast has a high rate of union in the over 60 s and we have described our simple and generalizable technique.
Most fractures (55%) were simple AO type A in keeping with the lower energy trauma expected in this older population. This is more than double than in Stedtfield and Biber that assessed 50 proximal third fractures across all age groups where 26% were type A fractures, perhaps reflecting the additional energy involved in younger patient trauma resulting in more type B and C fractures. 27% of our fractures were complex AO type C compared to their 54%. 20
The highest rate of non-union was seen in non-operatively managed AO Type B fractures, specifically bending wedge, where this occurred in six of eight patients. This contrasts with that seen in Ekholm et al. 16 2006, where non-union rate was highest in AO Type A fractures, though this only analysed 29 fractures. Much greater numbers are required to analyse fracture classification with any degree of statistical significance.
Mirroring the hip fracture population, most cases are female—this is a fragility fracture of the osteoporotic older woman. In 2020, Oliver et al 18 suggested that proximal and mid humeral shaft fractures should be considered fragility fractures and our findings would align with this 33 out of 75 patients were classed as ‘vulnerable’ or varying degrees of ‘frail’ (Rockwood CFS scores four and above), and these patients are at risk of losing independence following a physical insult, or less likely to have the physiological reserve to deal with trauma. Frailty is increasingly recognized as a global indicator of patient outcomes and a considerable number of patients sustaining this injury would be considered frail. 21
The British Geriatric Society 22 predict that 10% of over 65 s would be classed as ‘frail’ and, if true, this group would be considered frailer than average with a frailty incidence of 44%. Perhaps a key finding, and fundamental to surgical decision making, the frailty element can be seen through a different lens. 42 of 75 patients were not classed as frail. With hip fractures— frail patients are operated on to afford pain relief and enable early mobilization, while fit patients also undergo early surgery to optimize recovery.
The older patient with a proximal third humeral fracture can similarly be seen to have a ‘frailty split’: - There are those classified as ‘frail’ as per Rockwood score, with low tolerance of injury and prolonged recovery, who could potentially benefit from early pain control and avoidance of sarcopenia to overcome mobility concerns, provided they are fit enough for an anaesthetic. - There are also those who aren’t classified as ‘frail’ who have a greater physiological reserve and can better cope with the reduced function associated with a period of non-operative treatment. This group warrant being fully counselled around operative intervention given the high association of non-union with non-operative treatment. This may better guide approach to management and optimize patient specific care.
Length of stay in our unit was comparable between the groups. Achieving stability through surgery in humeral shaft fractures can provide early pain control, allow arm movement and early patient mobilisation. 23 Active elbow and shoulder pendular exercises start on the first day post-op. Weightbearing through affected arm was commenced after 4 weeks in this cohort of patients, but we are now moving towards weightbearing as tolerated through arm as required.
The non-operative management of these injuries in our unit has historically been down to the individual team, with U-slab application in the first instance, and timing of conversion to a functional humeral brace at the treating surgeon’s discretion. There are clearly many factors that may influence this decision such as the ‘personality’ of the fracture, the patient’s body habitus and skin condition, patient choice, and later during treatment, the presence or absence of radiological callus.
The senior author has moved away from using functional humeral braces for displaced proximal third humeral shaft fractures due to the humerus hinging and angulating on the medial side of the brace, backed up with data suggestive of a high incidence of non-union.
The senior author would therefore use a U-slab for displaced fractures until evidence of bridging callus is seen, which is then removed to allow free mobilisation depending on symptoms. Non-operative management is now only performed if a patient decides for this management or if they are medically unfit to undergo surgery. The numbers of displaced fractures managed non-operatively in our unit have reduced considerably.
Our data corroborate a trend towards non-union in non-operatively managed proximal third humeral shaft fractures (19 of 45) compared to operative (1 of 37). Pollock et al reported 31 humeral shaft fractures in patients over 55 treated non-operatively; 45% of fractures in the proximal third went onto non-union, which is similar to that seen in our study (42%). They also found a statistically significant correlation between increased average age and increased incidence of non-union when reviewing prior studies. 10
Our data align with results seen in multiple studies where non-union in non-operatively treated proximal third humeral shaft fractures is considered high, irrespective of age, such as Toivanen et al. with 54% non-union in 13 fractures, Rutgers and Ring with 29% non-union in 14 fractures, Harkin and Large with 40% non-union in 25 fractures and Ali et al with 24% in 54 fractures.4,7,9,11 Though these did not specifically look at the over 60 s age group. These series also demonstrate the weakness of the literature overall with heterogenous age range reporting, varied fracture patterns and very small numbers.
Fracture displacement is often used as a marker for intervention. It depends upon its relationship with the deltoid insertion and whether the fracture is segmental. Our observation is that most occur at or just distal to the level of the deltoid insertion and thus deltoid commonly displaces the proximal fragment into abduction leaving the distal segment in varus, as demonstrated in Case 1. Therefore, patients with displaced proximal third fractures associated with any displacement of cortical thickness, angulation or proximal segment comminution are selected for primary fixation in our unit. Whilst acknowledged as informed anecdote only, we consider them to represent the highest likelihood of progression to non-union with non-operative management.
Our data show that fracture union can reliably be achieved in this older, fragility fracture cohort when provided with sufficient mechanical stability through operative fixation, even in the presence of delayed fixation. This supports the idea that non-union in this age group is predominantly associated with insufficient mechanical stability rather inadequacy of biology. It could also explain why glenohumeral joint arthritis has been found to be an independent risk-factor for non-union, since increased shoulder joint stiffness would potentially increase strain at the fracture site. 15
We have shown that by using a bridge plating technique proximal third humeral shaft fractures heal reliably within 6 months, with mean time to union at just over 3 months. Each case should be taken individually especially in very elderly, frail patients and discussion with patient, family and the multi-disciplinary team are vitally important in the decision-making process. Further investigation into the short- and longer-term functional outcomes is warranted.
There are several limitations of this work although we do not feel that these detract from the key features we seek to bring to the wider orthopaedic community. These fractures are at risk of not healing with resultant impact on the patient, their carers and their healthcare system. Patients and clinicians can make more informed choices of considering surgery in this group and there would be real benefit in standardized study of this injury across multiple centres in a prospective cohort. We acknowledge that this work would be improved with prospective data, a standardized protocol for non-operative management, pre and post injury patient-reported outcome data, and a larger study group to corroborate our findings is needed. We present a single surgeon, single centre convenience consecutive series. It could be a further 75 cases would provide different results although this would contrast with other studies. Timing of healing in such a sample is almost arbitrary as it depends on clinic attendance and forecasted review. Assessment of union is notorious and again is a threat to this work. None of the operated patients declared as united have had any further complications nor needed unplanned surgery since the time of data collection and whilst not error proof, this does in some way strengthen the presumption that union assessment is robust.
Conclusion
We have shown that proximal third humeral shaft fractures occurring in older patients are bimodal in terms of frailty. Many are consistent with a fragility fracture population and 44% of this cohort are either ‘vulnerable’ or clinically ‘frail.’ Whilst having no inconclusive proof we suggest that non-operative management is more likely to result in non-union compared to operative.
Given the increasing emergence of this fracture type as being associated with a threat of non-union and the impact on both the frail and non-frail host, it is surprising that less academic enquiry has been focused on proximal third humeral fractures in older patients. We recommend that a core outcome dataset is developed and in the first instance, a large multicentre prospective cohort study is carried out to properly characterize this injury and impact on both patient and clinical services.
Footnotes
Declaration of Conflicts Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.