
Abstract
Background
Fragility hip fracture patients are often malnourished. Nutrition supplementation may help, but it is unclear if supplementation is impactful when considering outcomes. A systematic review of literature examining perioperative nutrition status for older adults experiencing a hip fracture was performed.
Methods
We searched Medline, CAB Abstracts and Embase (Ovid); Cochrane Library (Wiley); PubMed; Scopus; Global Index Medicus; Web of Science Core Collection; SPORTDiscus (EBSCO); and clinical trial registries ClinicalTrials.gov and WHO ICTRP from inception to April 2021, incorporating terminology related to nutritional interventions, fragility fractures, and postoperative outcomes. Two investigators reviewed citations for inclusion, extracted nutrition intervention criteria, and categorized hip fragility outcomes.
Results
Of 1792 citations, 90 articles underwent full-text screening, and 14 articles were included in the final sample. We identified nutritional interventions and 4 outcomes of interest. 8 studies (n = 649) demonstrated a mean difference of .78 days (CI .34-1.21) in length of stay (LOS) between the nutritional intervention and control groups. Rehabilitation ward stays were discussed in 2 studies demonstrating a non-statistically significant difference. 7 studies (n = 341) reported mortality rates; when pooled there was no statistically significant difference. 5 studies showed data for postoperative infections and 4 studies reported on postoperative urinary tract infections. Pooling of data found a statistically significant result (Relative Risk: .49 [.32, .75], P = .001) with low heterogeneity (I2 = 27%). 4 studies reported urinary tract infections (n = 140) in the intervention group and (n = 121) in the control group with a non-statistically significant result. Grip strength was only reported in two studies but pooling of the data was non-statistically significant.
Conclusions
This systematic review highlighted the lack of consensus regarding the type of nutrition interventions available and impact on outcomes of interest including mortality, length of stay, infections, and grip strength for fragility hip fractures in older adults.
• Frail preoperative physical function status adversely affects physical functional recovery in the postoperative period. • Malnutrition can be an increased risk for postoperative complications such as increased length of stay. • The impact of nutritional supplementation has not been fully ascertained in this population. Nutritional supplementation decreases postoperative infections following fragility hip fractures but is not associated with reduced length of stay, decreased mortality, or improved grip strength. Nutritional supplementation is a low-cost and low-risk intervention with the potential to improve postoperative outcomes.Key Points
Why does this paper matter?
Introduction
Fragility hip fractures are a common occurrence among older adults, especially women. The predicted increase in the number of older individuals will likely increase the incidence of falls. 1 Hip fragility fractures are a major cause of disability and dependency. Patients suffering a hip fragility fracture have a 1-year mortality rate of more than 1/4 and 1/3 require transition to a more restricted living environment. By the year 2050, the global number of hip fragility fractures is expected to be 4.5 million. 2 The economic burden on the US healthcare system is significant and currently accounts for $5.96 billion per year, with 44% of total costs due to intertrochanteric hip fractures. 3 The impact of hip fragility fracture goes beyond the patient affecting caregivers, families, and society at large.
Poor nutritional status pre-fracture is correlated with sarcopenia, poor presurgical function, and diminished appetite. 4 The literature suggests the utilization of a nutritional assessment in presurgical planning is associated with shorter hospital length of stay and reduced postoperative complications.5,6 Past studies have often focused on providing replacement calcium and vitamin D without further nutritional intervention. While this is of value, it does not explicitly address the question of nutritional supplementation and its role in postoperative recovery. In studies that do include nutritional interventions, those interventions are diverse and include oral nutritional supplements (ONS), nasogastric feedings, and administration of steroids. Oral supplements are reported as easy to give; however, there are older adults who may be unwilling or not able to consume these products effectively. 7 Nasogastric feedings are complex to administer and such supplementation has not been shown to reduce mortality. 8
It is not clear if perioperative nutritional support of older hip fragility fracture patients improves meaningful clinical outcomes. Many studies have demonstrated improvement in nutritional parameters with perioperative administration of oral nutritional supplements. However, whether this translates into clinically meaningful benefit remains undetermined. Perioperative supplementation may shorten hospitalization and decrease postoperative complications.9–11 A 2016 Cochrane review of randomized and quasi-randomized controlled trials of nutritional interventions for people aged over 65 years with hip fracture included 41 trials with 3881 participants. Most had methodological flaws with low or very low-quality evidence. Very low-quality evidence indicated that oral supplements may reduce poor outcomes including complications but demonstrated no clear effect on mortality. 8
A clearer understanding of the role of perioperative nutritional status would be helpful in identifying older adults who are likely to benefit from ONS, optimizing hip fracture liaison processes to improve quality of care, and identifying nutritional markers that serve as predictive markers for postoperative complications. We conducted a systematic review of the literature to examine whether perioperative nutritional interventions for older fragility fracture patients are associated with improved clinical or functional outcomes.
Methods
We conducted a comprehensive search of 11 databases: Medline, CAB Abstracts and Embase (Ovid); Cochrane Library (Wiley); PubMed; Scopus; Global Index Medicus; Web of Science SCI-Expanded; SPORTDiscus (EBSCO); and clinical trial registries ClinicalTrials.gov and WHO ICTRP. Our search combined controlled vocabulary and keyword searching relating to the core concepts of fragility fractures and nutritional supplementation. A complete search strategy is available in the Appendix. The search was first conducted in March 2020 and was updated in April 2021. No limitations were placed on study design, date of publication, or language of publication. To ensure no potentially relevant items would be overlooked, we conducted hand searching of reference lists of included articles and relevant reviews. The review was registered in PROSPERO (CRD42021159788).
Results were compiled in EndNote X7.8, and screening was facilitated by Rayyan, a web-based screening tool designed for systematic reviews. 12 Screening was completed in two phases: title/abstract screening, followed by screening of the full-text. Screening at both stages was done in duplicate, with two independent reviewers applying the inclusion and exclusion criteria. We included studies that were focused on fragility fractures, had an older adult population (defined as 65 years old and above), featured a nutritional intervention, and included at least one outcome of interest. We excluded studies that were focused on fractures caused by trauma and studies that did not report original data, such as opinion pieces and narrative reviews. Any discrepancies were resolved through discussion, or by a third party where necessary. At the full-text screening phase, reasons for exclusion were recorded and are reported in accordance with PRISMA standards. 13
The data extraction form was developed by one researcher and piloted by all researchers for further refinement and to ensure agreement between extractors. All data extraction was done in duplicate, with two researchers working independently to extract relevant data points. The methodological quality of the included studies was assessed using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies, which assesses the quality of the paper with regards to selection bias, study design, confounders, blinding, data collection methods, and withdrawals and dropouts.14,15
Quantitative analysis of findings was completed using RevMan. Events data, such as mortality, were pooled and presented as a Peto odds ratio, while continuous data, such as length of stay measured in days, were pooled, and presented as mean differences. Heterogeneity was measured using I2. Moderate heterogeneity was defined as an I2 of above 40%, while an I2 of above 70% was considered high. Quantitative analysis was only undertaken for outcomes with low heterogeneity and a fixed effects model was used.
Results
Study Selection
2641 items were retrieved through searching databases, of which 929 were duplicates. 80 additional studies were identified through hand searching, resulting in 1792 titles and abstracts screened. 1702 studies were excluded at the title abstract phase and 90 studies were screened as full text. Of the 90 full-text articles screened, 76 were excluded. Reasons for exclusion are reported in Figure 1. Details of the included 14 studies are available in Table 1. Prisma flow diagram. Characteristics of Included Studies. RCT = randomized controlled trial; LOS = length of stay; NR = not reported.

Study Characteristics
13 of the 14 studies were randomized,8,16–28 while the remaining study 29 was a quasi-experimental pre-post comparison group design without randomization. Studies were most frequently conducted in Spain,18,22,24 Australia,19,20 and Sweden.28,29 Remaining studies were conducted in Austria, 23 England, 17 Hong Kong, 25 Israel, 16 Switzerland, 26 Turkey, 21 and the United States of America. 27 The caloric value of the nutritional intervention was reported in 12 of the 14 studies and ranged from 149 kcals 22 to 1400 kcals. 29 Protein ranged from 9.9 g 16 to 40 g. 18
Of the 14 studies, 1 was found to have overall low risk of bias,
22
6 had moderate or unclear risk of bias,16,18,25–28 and 7 had high risk of bias.17,19–21,23,24,29 Methodological issues were most commonly associated with selection and blinding of participants. The summary of risk of bias for individual studies and across different domains are reported in Figure 2. Risk of bias for individual studies and across different domains.
Participant Characteristics
Patient Characteristics.
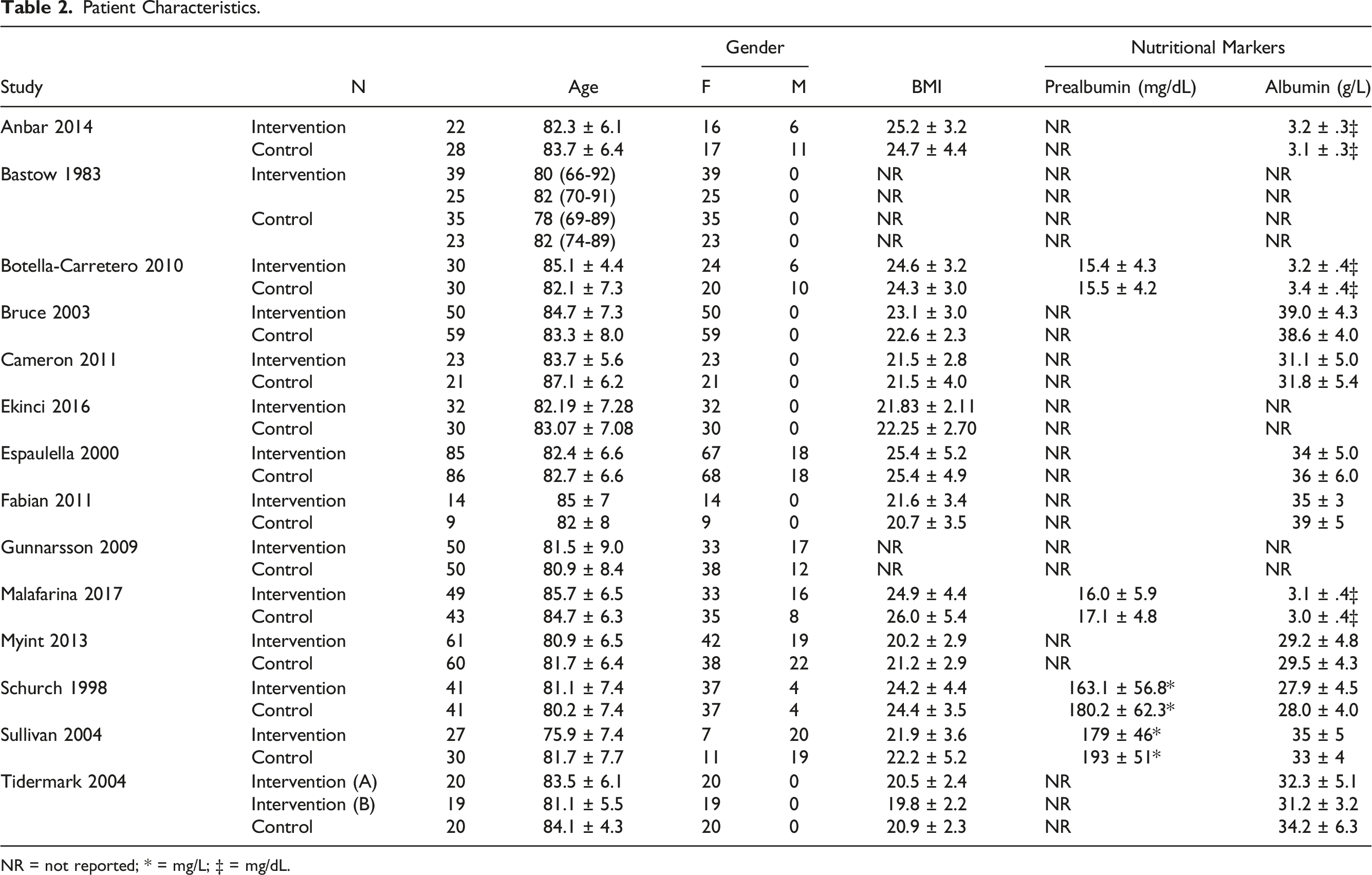
NR = not reported; * = mg/L; ‡ = mg/dL.
Outcomes of Interest
Hospital length of stay and stay in rehabilitation wards
Outcomes of Interest.
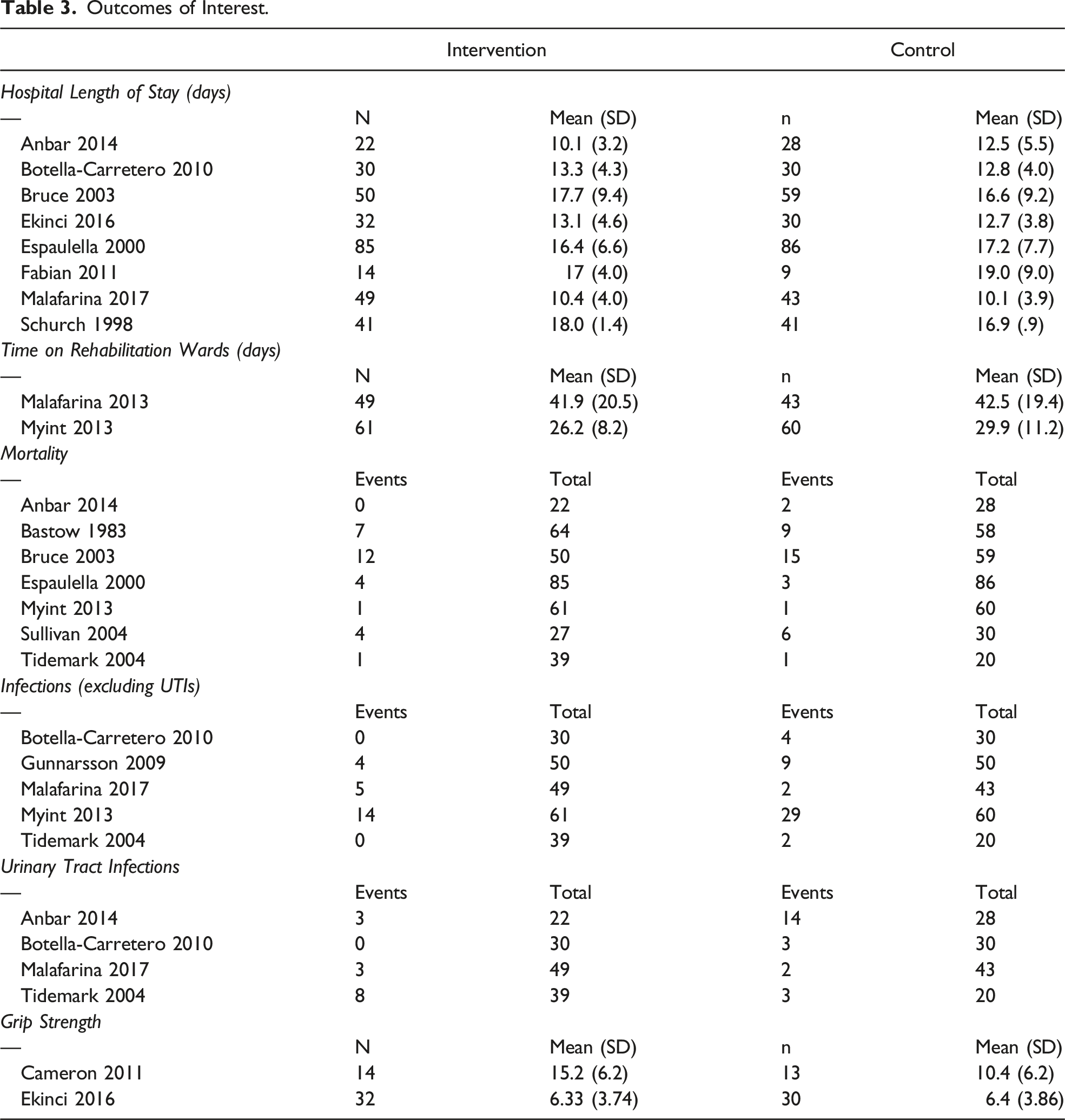
Mortality rates
7 studies reported mortality rates. Cumulatively, these 7 studies reported 29 deaths in 348 participants in the intervention groups and 37 deaths in 341 participants in the control groups. Two studies reported equal mortality rates in intervention and control groups,25,28 4 reported higher mortality rates in the control group,16,17,19,27 and 1 reported higher mortality in the intervention group. 22 When pooled, there was a non-statistically significant difference in mortality rates (RR: .83 [.53, 1.29], P = .4).
Infections and UTIs
5 studies reported on postoperative infections,18,24,25,28,29 and 4 studies reported on postoperative urinary tract infections.16,18,24,28 The five studies reported 23 postoperative infections in the 229 participants in the intervention group, and 46 infections in 203 control group participants. Four studies reported higher infection rates in control groups,18,25,28,29 while one reported higher infection rates in the intervention group. 24 Pooling of the data found a statistically significant result (RR: .49 [.32, .75], P = .001) with low heterogeneity (I2 = 27%).
Of the 4 studies reporting urinary tract infections, 2 reported higher UTI rates in the control groups,16,18 while 2 reported higher UTI rates in the invention group.24,28 14 UTI events of 140 participants in intervention groups and 22 UTI events in 121 control group participants were reported. Pooling of the data found a non-statistically significant difference (RR: .55 [.28, 1.07], P = .08).
Grip strength
Only two studies reported grip strength.20,21 Cameron reported higher grip strength in the intervention group while Ekinci reported better grip strength in the control group. Pooling of the data found a non-statistically significant difference (MD: .62, CI: −1.14-2.37, P = .49) and high heterogeneity (I2 = 72%).
Discussion
Despite broad interest in this issue and over 40 years of inquiry, it remains unclear how to best and even if to routinely provide nutritional supplementation to older hip fracture patients undergoing surgical repair. There were surprisingly few recent high-quality studies given the prevalence and health impacts of fragility fractures. Risks of being malnourished in the perioperative period are well documented. Poor outcomes including surgical complications, prolonged hospitalization and mortality are consistently described. This review demonstrates that in certain populations with specific interventions there may be some demonstrable benefit to perioperative supplementation nutrition. Many of these studies are small and require replication to confirm their findings.
Assessing the benefit of perioperative nutritional supplementation for fragility hip fractures in older persons is complicated by the heterogeneity of both the specifics of the intervention and the patient populations studied. While all studies include protein and caloric supplementation, the delivery, quantity, additional components, and monitoring vary widely among the studies reviewed. Study populations are generally female and over the age of 65; however, inclusion criteria differ widely. Some studies focus on the severely malnourished, others those with no to mild deficiencies and some have exclusion criteria that severely limit the generalizability of the findings. In addition to subject characteristics and interventions, outcome measures are diverse with varying degrees of clinical relevance. Studies are consistently underpowered for important outcomes such as cardiovascular complications and mortality
Bastow and Sullivan used HS enteral tube-feeding to deliver protein-calorie supplementation.17,27 Bastow noted 80% success in utilizing the NG administration route and decreased length of institutional care with supplementation. Sullivan found no benefit to the intervention with frequent difficulty in maintaining access with the tubes but was underpowered for most of the outcomes assessed. Studies that utilized nutritional support with a leucine metabolite, protein and calcium with vitamin D both demonstrated clinical benefit including reductions in immobilization 21 and improved muscle mass. 24
Schurch supplemented patients for 6 months and found a significant decrease in rehab LOS from 54 to 33 days. 26 The authors postulated that this was due to a decrease in overall complications including possibly new osteoporotic fractures. The only study to include a metabolic steroid with nutritional supplementation demonstrated benefits in activities of daily living and quality of life after 6 months of intervention. 28 The authors conclude that Nandrolone therapy may be a beneficial addition if patients are unable to exercise, noting that exercise is preferred based on other studies.
Most studies represented the population of interest. Subjects were appropriately older (>75 years old) women with osteoporosis and fall-related injuries. Subjects with dementia were almost universally excluded, which limits generalizability. Multiple different types of interventions were deployed across the studies analyzed. Different formulations of supplement, delivery method, and anabolic additions were utilized. Protein content of the supplementation varied widely. Pre-fracture functional status was generally not assessed. Measurement of intake by both subjects and controls was not consistent across the studies and could have impacted outcomes in several of the trials. Many studies include participants with normal to elevated BMI. Finally, the duration of the intervention and length of the study period varied widely and not all studies included rehabilitation stays.
Our findings show trends toward benefit in some of the important outcomes identified in the studies. These are not definitive but are consistent with findings of other systematic reviews.8,30 As noted above, this area of research is complex. Study populations are generally convenience samples with diverse characteristics. Interventions have not been standardized and clinically meaningful outcome measures are not consistent. Considering the magnitude and implications of hip fractures, continued assessment of potentially beneficial interventions is warranted. Multi-site trials with standardized interventions, well-defined relevant outcomes and adequate power are necessary to move this field forward.
Fragility fractures, especially hip fractures are sentinel events in the older adult population. Outcomes are even worse in the frail and malnourished population. Future research is needed to explore nutritional protocols and supplements to better optimize these patients to give them not only the best chance of healing, but a better opportunity to return to their pre-fall level of function. Perhaps with the evolution of fracture liaison services and more attention to multidisciplinary care there will be more protocol driven nutritional data.
Limitations
Our systematic review has several limitations. First, only 14 articles met the inclusion criteria. Second, there is a low risk of bias in only one study. In part, this is due to inherent challenges, such as the difficulty of blinding people to nutritional interventions or assessment. Third, dietary patterns vary from country to country. Therefore, direct comparisons may pose challenges when assessing health outcomes after fragility fractures across cultures.
Conclusion
Despite malnutrition and hip fractures having a significant impact on patient lives, this systematic review highlighted the lack of consensus regarding the type of nutrition interventions available and impact on outcomes of interest including mortality, length of stay, infections, and grip strength for fragility hip fractures in older adults. Given the predicted increases in overall hip fracture rates, a systematic approach to fragility fracture care is imperative. Nutritional supplementation may be one way to optimize these patients for surgery.
Footnotes
Appendix
Search Strategy for Ovid Medline (1) exp Osteoporotic Fractures/ (2) (intertrochanteric or subtrochanteric or trochanteric or hip* or femur or femoral). tw,kw. (3) exp Hip/ (4) 1 and (2 or 3) (5) exp Hip Fractures/ (6) (fragil* or (low adj2 (impact or energy or level)) or “low-impact” or “low-energy” or “low-level”). tw,kw. (7) (4 or 5) and 6 (8) ((fragil* or (low adj2 (impact or energy or level)) or “low-energy” or “low-impact” or “low-level”) adj3 (intertrochanteric or subtrochanteric or trochanteric or hip* or femur or femoral) adj3 fracture*). tw,kw. (9) 4 or 7 or 8 (10) exp Nutrition Therapy/ (11) exp Diet Therapy/ (12) exp Elder Nutritional Physiological Phenomena/ (13) exp Diet/ (14) exp Nutrition Assessment/ (15) exp Nutritional Status/ (16) exp Dietary Supplements/ (17) exp Food/ (18) (nutrition* or malnutrition or diet* or nourish* or undernourish* or malnourish*). tw,kw. (19) (underweight or overweight or obese or obesity or vegetable* or fruit* or starch* or cereal* or (diet* adj1 (fat* or protein* or fibre or fiber*))). tw,kw. (20) ((eating or food or feeding) adj2 (behavio* or habit* or intake*)). tw,kw. (21) (calories or ((caloric or energy) adj2 intake)). tw,kw. (22) (vitamin* adj3 (sufficien* or insufficien* or deficien*)). tw,kw. (23) or/10-22 (24) 9 and 23 (25) (aged or geriatric* or elder* or old* or ageing or aging). tw,kw. (26) exp Aged/ (27) exp Geriatrics/ (28) exp Aging/ (29) exp Frail Elderly/ (30) or/25-29 (31) 24 and 30 (32) exp humans/ (33) exp animals/ (34) 33 not 32 (35) 31 not 34 (36) ..dedup 35
Author Contributions
Conception/design: all authors; provision of study material: JSO; collection and/or assembly of data: all authors; data analysis and interpretation: all the authors; manuscript writing: all authors; final approval of manuscript: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.