
Abstract
Objective
To introduce the clinical features of and surgical techniques for a rare type of irreducible pertrochanteric femur fracture pattern with bisection of the lesser trochanter.
Methods
From January 2017 to December 2019, 357 patients with per/intertrochanteric femur fractures underwent surgery by closed reduction and internal fixation, of whom 12 patients were identified with rare preoperative imaging features, the lesser trochanter was almost equally bisected. The main fracture pathoanatomy of these cases included: The anterior fracture line passed along the intertrochanteric line to the medial lesser trochanter and bisected it into 2 equal parts from mid-level of the lesser trochanteric protrusion. The proximal part of the lesser trochanter connected to the head-neck fragment and attached by the psoas major tendon, while the distal part of the lesser trochanter connected to the femoral shaft and attached by the tendon of the iliac muscle. These fractures were irreducible by a closed maneuver and were reduced with limited assistance by some devices, and short intramedullary nails were used for fixation of these fractures.
Results
All patients were followed up for an average of 14.2 ± 2.1 months. Clinical fracture union occurred at an average of 10.8 ± 1.5 weeks, while radiographic union occurred at an average of 12.7 ± 1.2 weeks. No cut out of the helical blade was visible on radiographs. The average Parker-Palmer score was 6.9 ± 1.3 (range, 5-9) at the last follow up, including 8 cases rated as excellent, 2 as good and 2 as fair.
Conclusion
Two-part pertrochanteric femur fractures with bisection of the lesser trochanter have an irreducible fracture pattern with cortical locking and soft tissue incarceration. Soft tissue release and short cephalomedullary nail fixation for this fracture pattern provide stable fixation and allow early exercise. This treatment appears to have excellent outcomes in the short and medium terms.
Keywords
Introduction
Intertrochanteric femur fractures are among the most serious causes of mortality and morbidity in elderly people, and early surgical intervention is advocated to reduce hypostatic pneumonia, pressure ulcers or other complications caused by being long-term bedridden as much as possible.1-5 Most intertrochanteric fractures can be reduced by closed manipulation on a fracture table, with longitudinal traction and internal rotation of the extremity.6-8 However, approximately 10% of cases may not be able to be closely reduced through the conventional reduction method.9-13 These cases are defined as irreducible fracture patterns, and some form of open reduction with the insertion of a device is used in these cases.
Two-part intertrochanteric femur fractures with bisection of the lesser trochanter were first reported by Moehring et al, 9 with a low incidence among total pertrochanteric fractures. Sharma et al 10 reported 4 kinds of irreducible fractures, including a type in which the proximal fragment attached to a lesser trochanter was locked underneath the shaft fragment, bisected lesser trochanter with a locked proximal fragment, a posteromedial fragment overlapped at the fracture site, and a proximal fragment was flexed passively by the underlying lesser trochanter. Other authors have discussed irreducible fracture patterns, and the failure to recognize these patterns may cause serious consequences, leading to prolonged operation time and increased bleeding.11-13
The intertrochanteric fracture with a bisected lesser trochanter had the following pathoanatomical features: the main trochanter fracture line crossed the lesser trochanter and split it into 2 parts almost equally. The proximal portion of the lesser trochanter was a part of the proximal head-neck fragment, attached by the psoas major tendon, and deformed to a flexion-external rotation and valgus position. The distal portion of the lesser trochanter was a part of the distal femur shaft, attached by the iliac muscle tendon, and deformed to a proximal shortening and internal rotation position. The cause of fracture irreducibility was superolateral osseous interlocking and inferiomedial capsulo-ligament-tendon incarceration, repeated closed maneuver may fail and increase iatrogenic injury. The purpose of this study was to present the surgical technique for and the clinical outcome of this case series treated by a limited open incision and short proximal femoral intramedullary nail fixation.
Materials and Methods
Patients Data.

M: male, F: female, CN: cephalomedullary nails, FRQ: fracture reduction quality, TWB: time to partial weight bearing.
Fracture Characteristics
Preoperative X-ray, computed tomography (CT), and three-dimensional CT reconstruction images were used for fracture evaluation (Figure 1). These were simple two-part fractures without comminution. The anterior fracture line passed along the intertrochanteric line to the medial lesser trochanter and bisected it into 2 equal parts from mid-level of the lesser trochanteric protrusion. The proximal part of the lesser trochanter connected to the head-neck fragment and attached by the psoas major tendon, while the distal part of the lesser trochanter connected to the femoral shaft and attached by the tendon of the iliac muscle. The fracture had a typical displacement and overlapping relationship, ie the head-neck fragment was flexed anteriorly and rotated laterally, this displaced the fracture spike (inferior-medial cortical corner) anteriorly through the capsule causing soft-tissue incarceration, and the superior-lateral corner engaged into the femoral shaft to form a bony interlocking. The reason of irreducible by closed maneuver was that superolateral osseous interlocking and inferiomedial capsulo-ligament-tendon incarceration. Schematic picture to show the features of the pertrochanteric fracture with bisection of lesser trochanter. The upper portion of lesser trochanter was a part of the proximal head-neck fragment, which was attached with the psoas tendon, while the lower portion of lesser trochanter was a part to the distal femur shaft, which was attached with ilioas tendon.
Surgical Technique
Operations were performed by 1 orthopaedic trauma group familiar with the technique of cephalomedullary nailing of the proximal femur. Under spinal anesthesia, all operations were performed on a radiolucent traction table in the supine position. The usual manipulation of closed reduction of the fracture may be tried but usually fails. Therefore, limited open reduction was performed to reduce unnecessary secondary iatrogenic injury, with the injured limb fixed and placed in the natural tension state without traction.
A 3-5 cm long skin incision distal to the tip of the greater trochanter on the lateral thigh was made, which could also be used for insertion of the helical blade or lag screw. After exposure of the subcutaneous tissue, fascia lata, and lateral thigh muscle, the lateral side of the proximal femur was approached. A blunt separation from the anterior surface of the trochanter to the neck was performed, and the surgeon could use his or her finger to palpate the displacement at the fracture site.
Fracture reduction was carried out without traction and assisted by instruments. The technical tips are summarized as follows: ① With lateral rotation of the injured leg, a bone hook was introduced into the fracture site to catch the anterior cortex of the femoral shaft, and then, lateral traction and rotational leverage using a bone hook or periosteal elevator were attempted to release the cortical interlocking at the lateral-superior corner of the head-neck fragment. ② With traction of the leg, tensioned tendons or muscle on the medial side of femoral shaft (iliofemoral ligament, anterior capsule, or iliac muscle), which was considered to hinder reduction, was dissected to release the soft tissue locking and incarceration. ③ The head-neck fragment was retracted laterally, and the fracture was reduced by a bone hook. Then, 1 or 2 K-pins were inserted transversely or along the head-neck axis to temporarily hold the fracture. ④ After satisfactory reduction of the fracture, internal rotation and adduction of the limb could be performed, which facilitated cephalomedullary nailing, as described in detail in the manufacturer’s instructions. The K-pins could be removed when they interfered with nail insertion. The implant used is this case series was short proximal femoral intramedullary nails produced by Double Medical Technology Inc. from China.
Postoperative Management and Follow Up
All cases were encouraged to perform muscle isometric exercise and stand up on bed on the first postoperative day and were permitted to get out of bed with weight bearing as tolerated, at least 2 weeks after operation.
Patients were reviewed at 6 weeks, 3 months, 6 months, and 1 year after the operation, with clinical and radiographic assessments of the progress of healing and complications. Occurrences of internal fixation failure, including coxa vara deformity, refracture, cut out of the blade or penetration of the femoral head, and screw breakage, were recorded. The quality of fracture reduction (reduction score) and postoperative fracture stability (stability score) was assessed by the criterion proposed by Chang et al15,16 according to the AP view and lateral view of X-ray images. The Parker Palmer walking ability score was calculated at the last follow-up.
Results
All patients were followed up for an average of 14.2 ± 2.1 months (range, 12-18 months). With the assistance of brace, partial weight bearing was encouraged at an average of 3.0 ± 1.0 weeks (range, 2-4 weeks). Clinical fracture union, which was implied by the absence of local tenderness on palpation or motion of the injured hip joint, occurred at an average of 10.8 ± 1.5 weeks (range, 8-14 weeks). Radiographic union, as evidenced by bony trabeculae crossing the fracture interspace, occurred at an average of 12.7 ± 1.2 weeks (range, 12-16 weeks). All cases of fracture had healed with no loss of position by the 6-months or 12-months check-up. No patients had any evidence of AVN of the femoral head according to clinical assessment and radiographs by final follow up. No cut out of the helical blade was visible on radiographs. There were 3 cases with helical blade migration and sliding laterally. One case had developed delayed DVT 6 months after operation, which was improved after conservative treatment.
According to the criterion proposed by Chang et al.
16
(Table S1), the quality of fracture reduction was assessed using X-ray images taken immediately after the operation. Seven cases were assessed with a score of 4, and 5 cases were assessed with a score of 3. Seven cases were assessed with a stability score of 8 (excellent), and 5 cases assessed with stability score of 7 (good). The Parker Palmer walking function score
17
was used to evaluate the outcome of surgery. The average Parker-Palmer score was 6.9 ± 1.3 (range, 5-9) 1 years postoperatively, including 8 cases rated as excellent, 2 as good and 2 as fair. Images of typical cases are shown in Figures 2 and 3. Illustrative case with radiographic images (A) An intertrochanteric fracture with bisection of lesser trochanter on preoperative X-ray image; (B) Coronal plane on CT scan showed bony interlocking in the lateral superior conner (arrow); (C) The posterior cortex of the femoral neck was structurally intact (arrow). Head-neck fragment lateral rotated by traction of abductor on CT image; (D) 3D-CT reconstruction image of the fracture; (E) Mimics simulated fracture reduction and showed that the lesser trochanter was divided into 2 parts; (F) CT reconstruction showed that the psoas major tendon attached to the medial protrusion of head-neck fragment; G: Intraoperative reduction and maintenance of the fracture by use of a hook; (H-I) AP view and medial view of X-ray images 2 weeks after operation; (J) Front view on postoperative 3D-CT images; (K) Medial view on postoperative 3D-CT images. ★Upper part of lesser trochanter departed from head-neck fragment by traction of psoas major; (L-M): AP view and medial view of X-ray images 1 year after operation. Illustrative case 2 with radiographic images (A) AP view of X-ray image of an intertrochanteric fracture with bisection of lesser trochanter; (B) Coronal image of CT scan; (C) 3D-CT reconstruction image; (D) Mimics simulated fracture reduction; (E) After fracture reduction, transverse k-pin was inserted for temporary maintenance; (F-G) Intraoperative AP view and lateral view by fluoroscopy; (H-I) AP view 2 weeks after operation; I AP view and medial view of X-ray images 1 year after operation.

Discussion
With the aging of the population, pertrochanteric femur fractures are among the most serious causes of mortality and morbidity in elderly people, and early surgical intervention is advocated to relieve pain, avoid complications of long-term bed rest and recover self-care ability.3-5 Short cephalomedullary nails have been more frequently used for unstable intertrochanteric fractures in recent years.6-8 Regardless of the type of fracture, obtaining a good reduction quality is the goal of the internal fixation of fractures and is one of the most important factors affecting the long-term clinical outcome.
However, some kinds of fractures are not amenable to closed reduction through conventional manipulation, which are referred to as irreducible patterns. The radiological features of irreducible intertrochanteric fractures have been summarized, and classifications have been introduced by several authors. In our clinical practice, we divide these fractures into 2 categories. The first category involves communicated fractures (4 parts, 5 parts, or more), with the fragments separated from each other and obviously dislocated (coronal plane, sagittal plane and transverse plane), and there is no hinge of soft tissue between the fragments. During the operation, the force induced by traction of the extremity is not transmitted to the head-neck fragment, which may cause difficulty in realigning the fracture site. The second category is related to the structures of the lesser trochanter and iliopsoas. Fractures are often not very comminuted, and obvious bone interlocking and/or soft tissue interlocking occurs, which require the assistance of instruments.
The second group includes the following 4 subtypes. ① The lesser trochanter is fractured and departed, with the lower tip inserted into the fracture site or distal femoral cavity, which may cause irreducibility. ② The lesser trochanter is connected to a head-neck fragment with traction by the interposed iliopsoas tendon, and the head-neck fragment may be seriously flexed and displaced. ③ The lesser trochanter is connected to the femoral shaft, and the thicknesses of both fracture sites are not equal. ④ The lesser trochanter is bisected equally, with the iliacus muscle interposed between the head-neck fragment and femoral shaft. This is the fracture pattern we discussed in this paper.
Literature Data of Pertrochanteric Fractures with Bisecting Lesser Trochanter.
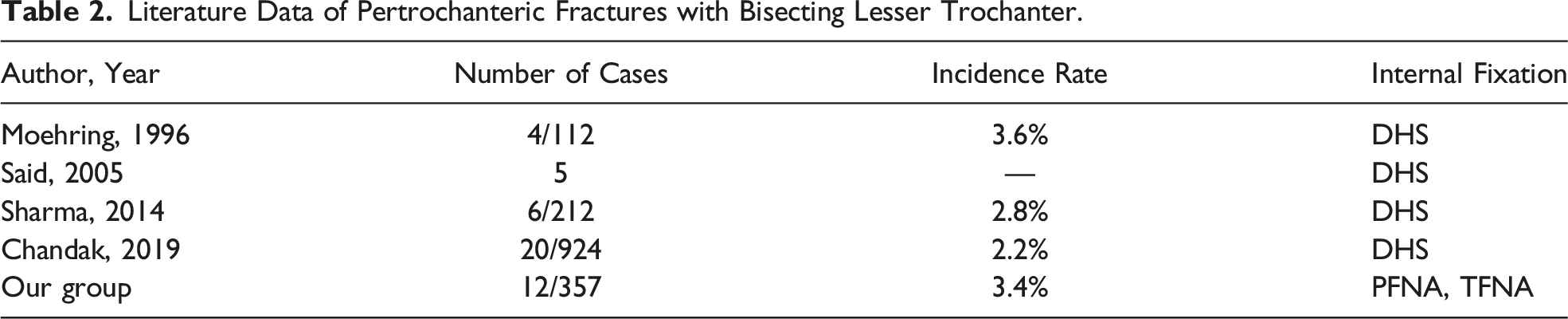
The occurrence of intertrochanteric fractures with bisection of the lesser trochanter may be related to the anatomical insertion of the iliopsoas tendon into the lesser trochanter.18,19 The iliopsoas tendon is a conjoined tendon. Bartoska et al 20 dissected 50 specimens and found that the iliopsoas tendon was attached directly to the lesser trochanter in 2 portions. The first circular portion, which was the attachment of the m. psoas major tendon to the apex of the trochanter minor, while the other longitudinal portion, which included the m. iliacus tendon medially enclosing the insertion of the m. psoas major tendon and projecting distally from the base of the lesser trochanter. Philippon et al 21 studied 53 specimens and found that the insertion points of the iliopsoas were a single tendon, double tendon and triple tendon, with occurrence rates of 28.3%, 64.2% and 7.5%, respectively (including iliac accessory tendon). The psoas major tendon is always in the most medial position and ends at the apex of the lesser trochanter. Gomez-Hoyos et al 22 studied the tendinous footprint of the lesser trochanter and found that the iliopsoas tendon footprints in the lesser trochanter were longitudinally oval and distributed in the anteromedial region of the lesser trochanter. There were 3 specimens with a single conjoined iliopsoas tendon, while 7 specimens with a divided attachment footprint were identified for the iliacus muscle and psoas major muscle. The bald area between the tendinous insertion of the psoas major tendon and iliacus tendon was a weak area that was easily fractured, which was the main cause of the bisection of the lesser trochanter.
Conclusion
Two-part pertrochanteric femur fractures with bisection of the lesser trochanter are an irreducible fracture pattern with cortical locking and soft tissue interposition. Short cephalomedullary nail fixation for this irreducible fracture pattern provides stable fixation and allows early exercise. This technique appears to have excellent outcomes in the short and medium terms.
Supplemental Material
Supplemental Material - Two-Part Intertrochanteric Femur Fractures with Bisection of the Lesser Trochanter: An Irreducible Fracture Pattern
Supplemental Material for Two-Part Intertrochanteric Femur Fractures with Bisection of the Lesser Trochanter: An Irreducible Fracture Pattern by Sun-jun Hu, Shi-Min Chang, Shou-chao Du, Li-zhi Zhang, and Wen-feng Xiong in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by National Natural Science Foundation of China (NSFC, no. 81772323).
Ethical approval
The article does not contain any studies with human participants or animals performed by any authors.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.