
Abstract
Keywords
Introduction
With an annual incidence of 120 per 100 000, femoral neck fractures are the most common fractures in Germany, predominantly affecting older individuals (incidence in those aged >70 years is 508/100 000). 1 It is estimated that the number of hip fractures worldwide will increase from 1 260 000 in 1990 to 4 500 000 by 2050. 2 For many of those affected, hip fractures will mean their independence is taken away from them, and the injury is associated with a high mortality rate. For example, 18% of those affected move into a retirement home as a result of their fracture, and 24% die within 1 year of injury. 3
The main goal of modern surgical approaches to treatment is rapid mobilisation in order to reduce complications and improve long-term survival. 4 Displaced femoral neck fractures are associated with an increased risk of femoral head necrosis where an osteosynthetic treatment approach is taken, such that endoprosthetic approaches are recommended, particularly in the elderly.5-7 In such cases, dual-head prostheses are technically easier to implant and are associated with shorter operation times, reduced blood losses, lower rates of dislocation, and lower costs as compared to approaches using a total endoprosthesis.5,8 Treatment with a total endoprosthesis demonstrates better functional outcomes in the long term, and should therefore especially be used in younger patients or those who are more active.8,9
It has been demonstrated that patients with postoperative anaemia are more difficult to mobilise following surgical treatment of hip fractures, have to remain hospitalised for longer, and have increased mortality rates.10,11 It is also important to note, however, that blood transfusions can lead to an increased incidence of wound infections and cardiac complications due to their impact on the immune system, producing increases in postoperative mortality and morbidity as well as rising treatment costs.12-15
Despite blood losses in cases of intracapsular fracture being lower than for extracapsular fractures, 16 surgical treatments using a dual-head prosthesis are more invasive than using an intramedullary nail. For example, implantation of a dual-head prosthesis results in an intraoperative blood loss of 150-350 mL, and the perioperative blood loss is reported as 800-1800 mL. 16 This means that it is not rare for patients to require transfusion. Ashkenazi et al reported a transfusion rate of 44% in 2020 in their study of 1218 patients who did not receive tranexamic acid as part of treatment with a dual-head prosthesis. 17 In this respect, it would seem beneficial to minimise perioperative blood losses.
Tranexamic acid (TXA) has been used in various different forms since 1966 for prophylaxis and treatment of bleeding. It is a cost-effective synthetic derivative of the amino acid lysine: it binds reversibly to plasminogen to produce an anti-fibrinolytic effect. 18 In recent years, it has been demonstrated that for elective hip and knee replacement surgeries, perioperative blood losses and the frequency of postoperative blood transfusions could be significantly reduced following TXA administration without an increase in the complication rate.19-22
In recent years, initial studies with small sample sizes have also shown a beneficial effect of administration of TXA with respect to blood losses and transfusion rates when used as part of treatment of femoral neck fractures using a dual-head prosthesis.23-25
Study Objectives
The aim of this study is to determine whether preoperative administration of TXA applied as part of treatment of femoral neck fractures using a dual-head prosthesis reduces blood losses and frequency of transfusion in a homogeneous study population. The secondary objective of the study is to determine whether the incidence of post-operative complications, such as acute kidney failure, heart attack and death decreases following administration of TXA. Furthermore, the frequency of TXA-associated complications (thrombosis, embolism, stroke, seizures) is to be recorded.
Patients and Methods
Study Design
Contraindications for TXA and recommended dose adjustments in renal insufficiency adapted from Pfizer´s Summary of Product Characteristics (SmPC).

Once any contraindications had been clarified and following recommendations from the literature, 23 patients in the TXA group received the standard dose of 1 g TXA intravenous (adjusted to 0.5 g in cases of renal insufficiency) 10 min prior to surgery (Table 1). The primary inclusion criteria were: medial femoral neck fracture and implantation of a cemented dual-head prosthesis. Cases presenting with any other musculoskeletal injuries were not permitted. Additionally, patients taking any anticoagulants other than aspirin could not be included. The analysis included patients who had received implants via both lateral and anterolateral approaches. Patients who were treated between 2015 and 2020, ie after the most recent change to the cross-sectional haemotherapy guidelines from 2014, 27 were included.
Data Collection
Analysis was carried out of the digital medical records. The following data was recorded for all patients: demographic data (gender, age, weight, height, BMI, aspirin intake, ASA score); process parameters (surgical technique, knife-to-skin time, duration of post-operative admission); and complications (thrombosis, embolism, stroke, heart attack, seizure, death); laboratory data from the day of admission (haemoglobin (Hb), haematocrit (Hct), platelet count, creatinine (Crea), glomerular filtration rate (GFR), quick time, activated partial thromboplastin time (aPTT); and from 1st post-operative day (Hb, Hct, platelet count); as well as the lowest GFR or highest creatinine values recorded over the course of treatment. In addition, the total number of red cell concentrates transfused over both the intra-operative and post-operative period were counted (RCC).
Preoperative blood volume could be determined from the data collected by applying the formula devised by Nadler et al, 28 and blood loss was calculated by applying the method by Good et al 21
Statistical Analysis
SPSS V.27 (IBM SPSS Statistics for Windows. Armonk, NY: IBM Corp) was used for the statistical analysis. The threshold for significance was set at P = .05.
Results
Over the analysis period, 345 patients underwent surgical treatment for a femoral neck fracture; of these, 187 were excluded due to contraindications to TXA administration (Table 1) or due to presenting with other fractures. Accordingly, it was possible to include 158 patients in the study, of whom 93 patients (59%) received TXA preoperatively. Seventy three patients received the full TXA dose of 1g preoperatively. For 20 patients, the dose was reduced to 0.5 g due to renal insufficiency. The other 65 patients (41%) did not receive TXA and were included in the comparison group.
The patient groups did not show significant differences for gender distribution (nonTXA 64.5% female; TXA 61.5% female; P = .739) or for average age (nonTXA 82.3 ± 8.2y; TXA 84.2 ± 7.01y; P = .144). According to the ASA classification, there was no difference between the two groups with respect to severity of pre-existing diseases (P = .907, Figure 1). 36% of patients in the TXA group were taking a platelet-aggregation inhibitor (aspirin) at the time of their injury. In the nonTXA group, this was 40%, which did not constitute a significant difference (P = .171). In terms of the preoperative laboratory results (Hb, Hct, Crea, GFR, Quick, INR, PTT), there were similarly no significant differences between the two groups (P > .05). Surgery was carried out on average 20.3 ± 13.9 h (nonTXA 19.5 ± 13.9 h; TXA 20.9 ± 14.0 h; P = .507) after the injury occurred. ASA classification of the two study groups.
On average, surgery was carried out at 20.3 h (3-77 h) after the presumed time of injury (nonTXA = 20.9 h; TXA = 19.5 h; P = .507).
Frequency of TXA administration and surgical technique.

The average knife-to-skin time was 80.95 ± 26 min, and there was no difference between the nonTXA group (80.97 ± 23 min) and the TXA group (80.94 ± 28 min). Patients were, however, treated significantly faster when following the anterolateral approach, irrespective of TXA administration (lateral approach 86.8 ± 27.3 min; anterolateral approach 75.5 ± 23.8 min; P = .014).
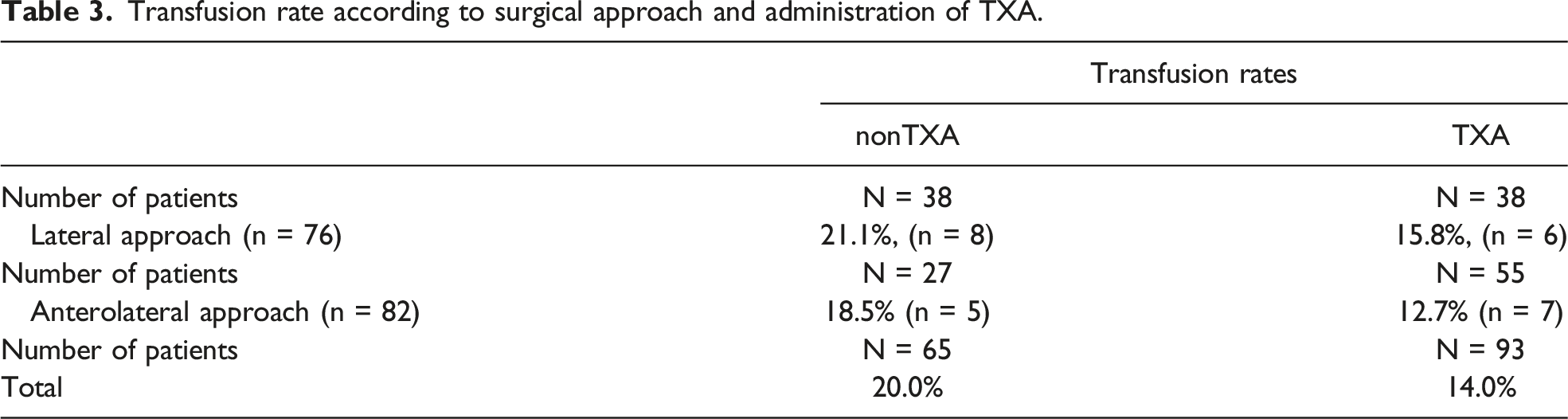
Transfusion rate according to surgical approach and administration of TXA.
The number of red-cell concentrates required per transfused patient was also evaluated. This revealed that patients in the nonTXA group were transfused with an average of 2.62 red-cell concentrates, whereas only 1.92 red-cell concentrates were required in the TXA group. This corresponds to a 26.7% reduction in the amount of blood transfused in the TXA group, although this result is not significant (P = .454).
Perioperative blood loss (recorded until blood sampling on day 1 post-OP).

Blood loss, red-cell concentrates and transfusion volume related to the TXA dose per kilogram of body weight.

It was not possible to determine a positive effect on the frequency of post-operative renal failure occurring. This complication occurred at essentially the same rate in both groups (nonTXA 7.7%; TXA 6.5%; P = .761).
Post-operative thrombo-embolic events.

Discussion
Guidelines from the United States of America recommend TXA use as part of elective procedures to implant hip and knee total endoprostheses for reducing blood losses and need for transfusion. 29 TXA is chemically similar to lysine, and so can block lysine binding sites on plasminogen, resulting in a temporary inhibition of fibrinolysis. 18 However, relatively limited evidence is available with respect to treatments for medial neck fractures using a dual-head prosthesis. Krebs et al included just one double-blind study in their 2019 review, whereby 84 patients received preoperative TXA in this same scenario. 30 In this study from 2015, Lee et al provided evidence of a 13% reduction in transfusion rates in the TXA group, concluding that the use of TXA can be recommended as part of procedures for implantation of dual-head prostheses for femoral neck fracture. 23
In our retrospective study, we included 93 patients who received TXA as part of treatment for femoral neck fractures using a dual-head prosthesis. We were only able to provide evidence for a trend towards a reduction in blood losses and transfusion rates, as well as a reduction in transfused blood volume. There was no significant difference due to administration of TXA.
In the nonTXA group, the transfusion rate was 20%, falling into the same range as seen by Lee et al (19%) 23 ; this was a significantly lower value than was found by Emara et al, 24 whereby 35% of patients not receiving TXA received a transfusion. However, in our study administration of TXA only reduced the transfusion rate down to 14%. This trend was independent of whether the surgery was performed via a lateral or anterolateral approach. Lee et al and Emara et al, on the other hand, saw a significant reduction in transfusion rates, down to 6% and 5% respectively, following TXA administration.23,24 Watts et al were also able to provide evidence of a non-significant reduction in transfusion rate. 31 In their study, the transfusion rate was reduced from 26% to 17% with administration of TXA for the treatment of hip fractures with a dual-head prosthesis or total endoprosthesis. The authors concluded that with just 69 patients receiving TXA, the sample size was too small to provide evidence of a significant difference. This same cause may well have been behind a lack of significance in our study, in which 93 patients received TXA.
It is striking that in our study the calculated blood loss from admission up to blood sampling on day 1 post-OP, ie over the perioperative period, did not change. There were no differences in the patient demographic parameters which could have caused this, such that we can assume that there must have been other factors influencing blood loss besides administration of TXA that were not specifically recorded in our study. On retrospective analysis, it can be noted that at the beginning of the inclusion period all surgeons were operating via a lateral approach, whilst operations carried out towards the end of the inclusion period were performed, mainly by the more experienced surgeons, using an anterolateral approach. The other surgeons continued to operate using a lateral approach. Due to the small sample size, a more differentiated evaluation carried out in this regard for the individual surgeons was not meaningful.
No intraoperative complications which could be related to administration of TXA occurred. Additionally, no complications have been reported in the literature. Postoperatively, the rate of thrombo-embolic events in the TXA group is slightly higher at 7.5% as compared to the nonTXA group (4.6%). This has already been described in the literature by Zufferey et al. In their study, the rate of postoperative events following osteosynthetic treatments for hip fractures in a TXA group was 10% higher as compared to their nonTXA group, which did not constitute a significant difference (16% vs 6%). 32 As part of their reviews published in 2019 of the existing studies on TXA administration as part of treatment of hip fractures, Krebs et al and Qi et al were not able to find any studies in which there was a significant increase in the rate of thrombo-embolic events.30,33
It was not possible to figure out a significant reduction in the incidence of post-operative renal failure in our patient population (nonTXA = 7.7%; TXA = 6.5%; P = .76). Cheung et al obtained the same result in their 2020 study, which evaluated U.S. registry data of 3812 patients who had received TXA as part of treatment for hip fractures: irrespective of TXA administration, they saw post-operative renal failure in 4.9% of cases. 34 In some other studies, patients with pre-existing renal insufficiency were excluded,32,35 or else further investigations were not carried out. By contrast, results from a 2014 study by Poeran et al, 22 with a patient population composed of 20 051 patients receiving elective hip and knee total endoprosthesis, identified a significant reduction in postoperative renal failure, with a decrease from 1.6 to 1.2%. This demonstrates that a high number of cases is required to even detect these small changes in the complication rate.
With respect to trauma patients, the CRASH II study was able to show that the shorter the time delay from trauma to administration, the greater the effectiveness of TXA. 36 For elective surgeries, TXA is given just before the start of surgery and any blood losses only occur either during the operation or after the operation. Studies with large sample sizes were able to show evidence of a benefit for patients undergoing elective procedures for endoprosthetics. 22 In cases of femoral neck fracture, blood losses due to the fracture itself tend to be low, 37 but there is an activation of the fibrinolytic system. 38 As a result of this, earlier dosing with TXA should be considered if necessary.
Determining the optimal dose of TXA is still problematic. The regimens for TXA administration in the studies presented here, all relating to procedures for elective endoprosthetic implantation and urgent fracture treatments, showed a great deal of variation. For example, a single 1g dose has been given before surgery;35,39,40 or 10 mg/kg 41 or 15 mg/kg42-45 doses have been applied according to body weight. In some cases, a second dose was also administered postoperatively.41,43,46 Local application of 2 g or 3 g TXA has also been trialled.39,47 In all of the studies cited here, blood loss associated with surgical treatment of hip fractures was reduced, and complications were not seen to increase. However, the number of cases is so small that it is not possible to make recommendations for a therapy regimen. We selected the 1 g dose primarily because it was the easiest to dose. The dose was therefore between 10 mg/kg and 15 mg/kg for most patients. However, in patients with higher-grade renal insufficiency, only 0.5 g TXA was administered pre-operatively, irrespective of the patient’s weight. Wang et al 48 published a dose-finding study in 2016 including about 40 patients per group; this study was able to demonstrate that effects of TXA can be seen at doses of 10 mg/kg. Nevertheless, a more pronounced effect could be seen at a dose of 15 mg/kg with a reduction in both blood loss and probability of transfusion. Following this logic, some of our patients must have been under-dosed due to our fixed dose of 1 g (or a reduced 0.5 g dose in renal insufficiency). We could only see a decrease in blood loss and transfusion volume at a dose of more than 15 mg/kg [Table 5]. However, this group was relatively small, so that no significance could be reached.
In summary, it was not possible to provide evidence of a significant reduction in transfusion rate, blood loss or post-operative renal failure in our study. We were only able to identify a trend towards reduced transfusion rates and transfused blood volume. This may be due to the low sample size and the fixed-dose regime of 1 g (or 0.5 mg for cases of renal insufficiency). No side effects or increased complication rates following administration of TXA were observed. There is growing evidence in the literature that TXA should also be used as part of endoprosthetic treatments for femoral neck fractures, similarly to procedures carried out for elective hip replacements. However, high-quality studies with larger sample sizes, as well as registry studies, would be desirable and indeed necessary to draw conclusions on this particular issue, especially with respect to the TXA doses employed.
Limitations of the Study
The patients included in the study underwent surgeries which involved 2 different approaches, and the inclusion period was relatively protracted at 5 years. However, the statistical evaluation demonstrated that the patient populations were comparable despite this. The transfusion protocol was implemented over the entire study period according to the cross-sectional haemotherapy guidelines from 2014. 27 Furthermore, this is a retrospective study, as randomised control studies on TXA use are essentially impossible to implement in Germany due to the high costs involved when following current regulations. However, given that administration of tranexamic acid was only recorded in the anaesthesia protocol and was not specifically communicated to doctors in charge of subsequent treatment, it is unlikely to have had an influence on postoperative treatment.
Footnotes
Author Contributions
Study design, conception, and critical revision: AW Acquisition of data: IW Analysis, and interpretation of data: PS, IW, AW Literature search and drafting of manuscript: AW, IW Final manuscript review/editing: AW, PS, IW, GH. All authors read an approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Helsinki: The authors declare that the procedures were followed according to the regulations established by the Clinical Research and Ethics Committee and to the Helsinki Declaration of the World Medical Association.
Funding
We acknowledge financial support for the publication by the German Research Foundation Projekt-Nr. 512648189 and the Open Access Publication Fund of the Thueringer Universitaets- und Landesbibliothek Jena.
Ethics Approval
This study is a retrospective analysis of patients with hip fractures treated surgically between 2015 and 2020 at the University Hospital Jena, Germany. It was approved by the local ethic committee of the University Hospital Jena (5030-01/17).
Consent for Publication
Is not necessary. All data are anonymized.
Informed Consent
According to the Ethics Committee of the University Hospital Jena (5030-01/17), informed consent is not required, as this is a retrospective data evaluation with anonymised data.
Availability of Data and Material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.