
Abstract
Introduction
Femoral neck fractures (FNF) in the geriatric population are commonly treated with hip replacement procedures, such as total hip arthroplasty, unipolar hip hemiarthroplasty (UHA), and bipolar hip hemiarthroplasty (BHA). The optimal treatment remains controversial, considering outcomes and cost-effectiveness, with UHA often being cheaper. This prospective observational study aims to evaluate UHA’s clinical and radiological outcomes, safety, and survivorship compared to existing literature.
Methods
We followed 90 elderly patients who underwent UHA following FNF. We assessed patients using the Parker score before and after surgery, as well as Harris Hip Score (HHS), and Postel-Merle d’Aubigné (PMA) scores postoperatively. All complications, acetabular erosions and heterotopic ossifications (HO), were documented.
Results
One year post-surgery, 26.7% of patients had passed away, mostly due to declining general health status. Systemic complications occurred in 14.4% of cases, with a 1.1% rate of deep surgical site infections. A single dislocation resulted from excessive stem anteversion. UHA implant survival rate was 97.8% after 4 years. The Parker score remained stable, and HHS at 6 and 12 months was 71.5 ± 12.9 and 70.9 ± 11.8, respectively, while PMA score was 14.3 ± 2.4 and 14.5 ± 2.1, respectively. Five hips showed Baker I acetabular wear. HO were noted as Brooker I in 12 patients, II in 4 patients, and IV in 1 patient.
Discussion
UHA exhibited comparable systemic complication rates, implant survivorship, and dislocation rates to those in the literature for both UHA and BHA. The deep surgical site infection rate was lower than reported for BHA. Patients’ functional and mental abilities did not decline based on clinical scores. Acetabular wear in UHA was similar to its bipolar counterpart, while HO were only minor findings with no clinical implications.
Conclusion
In elderly patients, UHA demonstrated clinical and radiological outcomes similar to BHA in existing literature. UHA may represent a cost-effective alternative for patients with limited life expectancy.
Keywords
Introduction
The growing percentage of elderly individuals, along with the increasing life expectancy, are resulting in a global increase in the occurrence of osteoporosis-related femoral neck fractures (FNF). 1 In this group of patients, displaced FNF are mostly treated with prosthetic replacements, such as total hip arthroplasty (THA), or hemiarthroplasty (HA), in which the retained native acetabulum articulates with a bipolar or unipolar femoral implant. 1 Hip fractures in older patients are associated with a multitude of pre-operative medical conditions and a frail general status, as well as high rates of post-operative morbidity, mortality, and loss of independence. 2 In this context, optimal treatment of FNF in elderly patients remains controversial in terms of outcomes, but also in terms of cost-effectiveness, as unipolar hemiarthroplasties (UHA) are often a cheaper alternative. 3 The aim of this prospective observational study is to monitor the clinical and radiological outcomes, as well as the safety and survivorship of UHA by comparing its outcomes to current literature.
Methods
The present clinical study is conducted in conformity with the French regulations and approval has been waived by the CCTIRS (Comité Consultatif sur le Traitement de l’lnformation en matière de Recherche dans le domaine de la Santé - French Medical Research Board), and the CNIL (Commission Nationale de l’informatique et des Libertés - National Commission on IT and Liberty). Written informed consent to publication of clinical information and imaging was obtained from all patients. STROBE cohort reporting guidelines were followed. 4
Patients Selection
We prospectively followed 90 patients who underwent UHA for FNF between January 2013 and December 2017 (Figure 1). Patients with pathological fractures, rheumatoid arthritis or symptomatic osteoarthritis were not included. The study cohort consisted of 66 women (73.3%) and 24 men (26.7%), with a mean BMI of 22.38 ± 3.91 kg/m2. All selected patients were over 75 years old with a mean age of 89.4 ± 5.0 years (76-102), and no severe cognitive dysfunction (more than 3 correct answers on the Short Portable Mental Status Questionnaire). 77.8% of patients were more than 85 years old and 46.5% were living in a nursing home. Most cases (98.9%) had notable pre-existing medical conditions: 83.3% had a cardiovascular disease, 20% had respiratory issues, 24% had neurological disorders, 22.2% presented digestive problems and 20% had diabetes. The mean ASA (American Society of Anesthesiologists) score was 2.7 ± 0.6 points (1-4). Most patients (64.4%) were ASA 3 (Severe or debilitating systemic disease/severe impairment of major function that does not result in disability), while 5.6% were ASA 4 (severe systemic disease that is a constant threat to life). 93.3% were classified as Charnley A (non-pathological contralateral hip or previously successfully operated), 1.1% were classified B (controlateral hip in need of an arthroplasty, or an unsuccessful or failing arthroplasty), and 5.6% were classified C (Multiple joints in need of arthroplasty, multiple failing arthroplasties, or other factors contributing to failure to achieve normal locomotion).
5
79.3% of all fractures were classified as Garden III or IV. 45.6% occurred on the right side, and 54.4% on the left. The fracture line’s obliquity was <30° (Pauwels 1) in 8 cases, 30°<-<50° (Pauwels 2) in 46 patients, and >50° (Pauwels 3) in 36 cases.
6
Patients’ selection and cohort formation according to the exclusion criteria.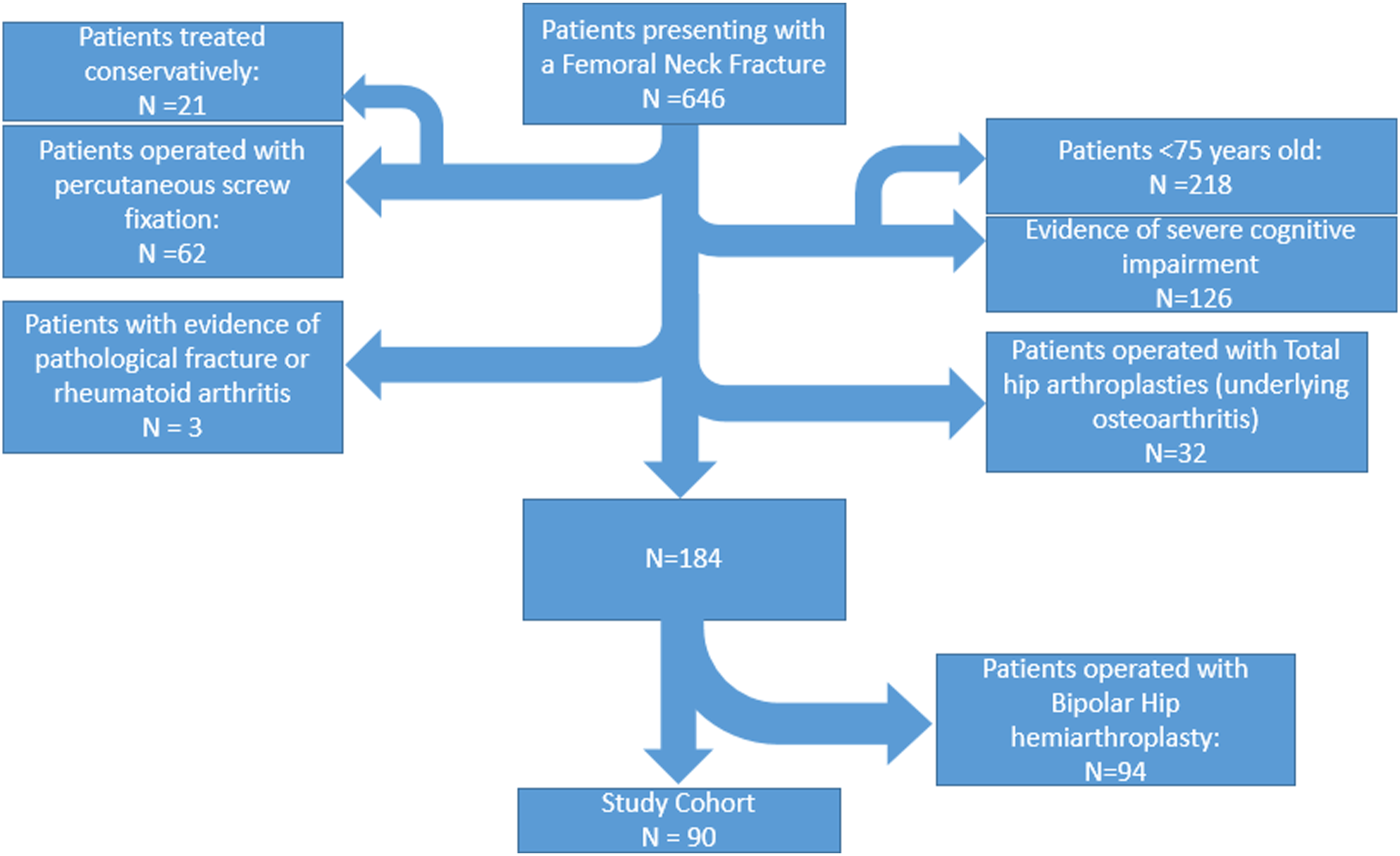
Surgical Intervention and Post-Operative Care
All patients were operated in the University Hospital of Clermont-Ferrand (Gabriel Montpied), under general anesthesia, by 4 attending surgeons (co-authors RE, GV, SB and SD). The surgical approach was anterolateral in 78 cases and anterior in 12. The prostheses used were the unipolar cephalic implant ONE HEAD with a cemented PLM femoral stem (EUROS, La Ciotat, France) (Figure 2). The 2-mm increments in the prosthetic head diameter allowed accurate reproduction of each patient’s anatomic femoral head measured intraoperatively. All patients were given low-molecular-weight heparin preoperatively and for 30 days postoperatively. Cloxacillin 2 g was given preoperatively, followed by 2 additional doses during the first 24 h. Postoperatively, patients were carefully mobilized (weight bearing as tolerated) with the help of a physiotherapist. They were allowed to sit on an elevated chair on day 0, and were encouraged to abandon the crutches at their own convenience. All restrictions were lifted after 6 weeks. Picture of the ONE HEAD modular unipolar cephalic implant (Left) and PLM stem (Right).
Outcome Measures
Patients were assessed pre-operatively (Parker score for pre-injury mobility and mental status was obtained upon arrival), and post-operatively (Parker, Harris Hip Score HHS, and Postel-Merle d’Aubigné PMA scores) at 6 and 12 months.7,8 On the radiological level, acetabular erosion was analyzed at 6 months post operatively according to Baker criteria, 9 while the Brooker classification was used for assessment of heterotopic ossifications (HO). 10
Statistical Analysis
Categorical variables are expressed as percentages. Quantitative data are expressed as means, standard deviations and ranges. Statistical analysis was performed using Fisher’s exact test for categorical variables and the unpaired t test for quantitative variables. The level of statistical significance was P < .05. Implant survivals were calculated by the Kaplan-Meier method with a confidence interval of 95%. The probability of implant survival was calculated by defining failure as implant revision for any cause. The statistical analyses were performed using the software XLSTAT 2022.4 -Addinsoft, NY.
Results
General Complications
Post-Operative General Complications Following UHA.

aPatients who died during post-operative hospital stay, or presented a complication during that period that eventually led to death within a month post-operatively.
Deaths and Mortality Rate
Two patients died within 4 days postoperatively: One chronic respiratory insufficiency exacerbation in an 88-year-old patient, and 1 stroke in a 97-year-old patient. One patient sustained a heart attack on day 1, was revived, but died 2 months later. One case of pulmonary embolism occurred in a 91-year-old patient who died 14 days post-operatively. Finally, 1 patient sustained a head injury and died 13 days after surgery. Twenty four patients were deceased at 1 year follow-up (26.7%).This number increased to 37 patients (41.1%) at 2 years, and 64 (71.1%) at 4 years. The mean age at the time of death was 91.7 ± 6 years (77-102). Most died from natural causes or due to deteriorated health condition.
Local Complications and Implant Survival
A total of 4 local complications were reported, including 2 hematomas in patients who were on anticoagulation therapy (not requiring surgical procedure), 1 deep wound infection that required a partial revision with head exchange 25 days after the index surgery, and 1 post-traumatic dislocation that needed surgical revision at day 7. During revision, an excessive femoral stem anteversion (−30°) was noticed and corrected. The 2 latter revision surgeries accounted for a total revision rate of 2.2%. No other implant failure (including aseptic loosening and periprosthetic fracture) was recorded for all the duration of the study. Therefore, the estimated survival rate of the implant was estimated around 97.8% at 4 years.
Clinical Outcomes
Due to the old age of patients included in this study, only 4 (of the 26 still alive) presented pysically to the final 4-year follow-up, while the rest were contacted by phone. The mortality rate was high and made the mid-to long-term data collection challenging. The overall mean follow-up was 20.3 months (0-48).
Parker Score (Mobility Score: 9 Points; Mental Score: 10 Points)
Pre-injury Parker score was obtained for all patients, and 58 patients were assessed post-operatively with this tool at a mean clinical follow-up of 6.8 ± 7.4 months (3-35). The mean mobility score was 4.1 ± 2.5 points (.0-9.0) pre-operatively and 3.6 ± 2.3 points (.0-9.0) post-operatively, while the mean mental score was 5.2 ± 3.8 points (.0-10.0) pre-operatively and 6.0 ± 4.2 points (.0-10.0) post-operatively.
Harris Hip Score (100 Points)
Harris Hip Sore (HHS) Results.

PMA Score (18 Points)
PMA Score Results.

Radiological Outcome
Seventy three operated hips were radiographically assessed at 6 months. Sixty eight hips (93.1%) had no secondary acetabular wear. The remaining 5 were classified as Baker Grade I (narrowing of articular cartilage with no bone erosion). Development of HO was graded according to Brooker classification as zero in 56 patients (76.7%), I (mild) in 12 patients (16.4%), II (moderate) in 4 patients (5.5%) and IV in 1 patient (1.4%). No fracture and no evidence of loosening were found in these evaluated hips.
Discussion
Hip fractures are one of the most common geriatric fractures, and their treatment is a significant economic burden for both patients and healthcare systems. 11 The aim of the present study is to monitor the results of UHA performed in our institution in terms of complication rates, clinical, and radiological outcomes in elderly patients treated for FNF, by comparing them to the data provided in current literature concerning both UHA and bipolar hemiarthroplasty (BHA).
Among the cohort, most cases were included according to the French National Authority for Health (Haute Autorité de Santé) recommendations (Parker mobility score <5 or age >85 years old). Due to the life threatening character and high perioperative mortality rate of FNF, especially when considering the fragility of the included patients, 26.7% of our patients died within a year, and only a few patients attended the final follow-up. The same observation is made in previous studies where around a quarter of patients die within a year post-operatively.2,12
The systemic complications rate of 14.4% found in our study is comparable to the literature on unipolar heads as Hedbeck reported 10.3% of general complications including deep vein thrombosis and pressure ulcers. 13 Ogawa reported the same percentage in 281 140 Japanese patients over 60 years old treated with HA (without specifying the HA implant type). 14 In a 2015 meta-analysis by Zhou, both unipolar and bipolar designs yielded a general complication rate neighboring 15%. The absence of significant differences between UHA and BHA is understandable since these types of complications are mostly related to the patient’s age, health status, and multiple pre-existing comorbidities rather than the implant design itself. Furthermore, it has been proven that a high ASA score and advanced age were correlated to an increased risk of complication and mortality in both groups equally. 15 In the present study, nearly half our population already lived in a nursing home and needed assistance in daily life before their fracture, with an ASA score >3 in 70% of cases, which goes in line with previously published series. 16
The deep surgical site infection rate of 1.1% was reasonable regarding recent literature, as a 2021 series of 3966 patients by Craxford yielded a 1.7% infection rate in UHA. 17 As for BHA, a meta-analysis by Wang, reported 16 cases of periprosthetic joint infection on a total of 311 bipolar HA (5 studies), making the infection rate of this kind of implant as high as 5%, 18 while keeping in mind that infections cannot be solely imputable to the implant, as multiple factors can be involved.
The only potentially implant-related complication reported in this study was a dislocation that required a total surgical revision 1 week after index surgery, accounting for a dislocation rate of 1.1%. This is to be contextualized by the circumstances that led to this event (traumatic fall) and the fact that an excessive stem anteversion was present. There was no need for conversion to THA since the probable cause was identified and corrected. It is important to note that dislocation rates in the literature has been reported to be around 3.9% for UHA and for 2.5% BHA, 19 with more recent meta-analysis showing no significant difference in terms of dislocations rates between the 2 groups.15,20
The survival rate of UHA in the present study is in accordance with the data provided by the 2018 Australian Registry Report, where cumulative survival rates of 97.2% and 96.5% were noted at 2 and 3 years respectively. 21 These high survival rates for UHA also seem to apply on the longer term, as demonstrated by an RCT from Kanto et al 22 who noted a survival rate of 98% at 8 years for UHA, noting that equivalent results were also found for BHA (97% at 8 years) in the same study. Though a slightly lower survival rate has been found for HA in a more recent retrospective study, 23 this outcome was still identical for UHA and BHA (92% at 5 years for both). Furthermore, it is also important to note that no periprosthetic fracture was recorded during our study’s duration, which may be attributable to the systematic use of cemented stems in this specific population. 12
The Parker score did not significantly decrease post-operatively, which demonstrates that patients did not lose functional or mental ability after surgery when compared to their baseline level (before fracture occurred). It can be concluded that most patients returned to pre-fracture level of mobility and mental status (with some even improving their mental score significantly).
Global HHS mean score was similar to what was previously reported by Inngul et al 24 (73.8). More specifically, our study revealed a mean score of 39 points for the Pain Item of the HHS, comparable to the UHA cohort of Inngul, which recorded 39.5 points at the 4-month follow-up. Our observed mean function score of 22.8 also aligns with the findings of the same study, which reported 25.6 points at 4 months. The relatively low mean HHS we documented appears to be primarily influenced by the low scores on the function items, particularly the gait score, averaging 14.9 ± 7.8 points out of 33.
Both our findings and those of Inngul et al stand in contrast to higher HHS reported for UHA in other studies, such as those conducted by Mishra et al and Abdelkhalek et al (81.9 and 84, respectively).25,26 This variance can be attributed to the significantly younger mean age of patients included in the latter 2 studies (67 and 63.5 years, respectively), as the HHS has been shown to consistently decrease with age. 27 The same holds true for the high percentage of patients with poor scores (HHS <70) that we observed. It is worth noting that Abdelkhalek et al demonstrated a significant difference in HHS between UHA and BHA, while Mishra et al did not find such a distinction. This discrepancy was addressed by a meta-analysis conducted by Liu et al, 28 which revealed no statistically significant difference in HHS between UHA and BHA.
As for the PMA score, almost half the patient of our cohort had good to excellent scores, and this proportion remained constant between 6 and 12 months post-operatively (46.55% vs 46.16% respectively).
Regarding radiological observations, only 6.9% of evaluated patients had a Grade I acetabular erosion according to Baker’s classification at 6 months of follow-up. This finding is not surprising in a cohort of elderly patients, knowing that the level of physical activity is correlated with the severity of acetabular erosion in UHA. 29 In a previous study involving younger individuals (mean age 67), the rate of acetabular wear in UHA was as high as 20%. 25 In the study of Inngul, 24 acetabular wear was reported at 16% in UHA group and 5.5% in the BHA at 4 months post-operatively. This gap appears to progressively close over the years until no statistical significance remains, as demonstrated by multiple subsequent meta-analysis.3,15,28 The lack of significant difference can be explained by a possible loss of mobility of the BHA with time, which leads to a UHA-like functioning. 3
Farey et al 20 drew conclusions from a comprehensive analysis of 62 875 hip procedures, indicating that UHA posed a higher risk of revision for acetabular erosion compared to BHA, particularly after 5.5 years. However, it is noteworthy that in our current study, only 26 patients remained alive at the 4-year mark, and none reported experiencing inguinal pain. As a result, the potential benefits of choosing BHA over UHA for this specific outcome remain a subject of debate. 30
Development of HO was observed in only 17 patients, the vast majority of whom (12) only presented minimal bony islands within surrounding soft tissues (Brooker 1) at 6 months post-operatively. These findings may at least partly be attributed to the surgical (anterolateral and anterior) approaches. 31 Though HO development has been previously analyzed in THA, HA or hip resurfacing, to our knowledge, no study has investigated the relationships between the design of HA (UHA vs BHA) and development of HO. This should be the focus of further dedicated studies.
We encountered some limitations in the analysis of our results. The relatively low number of patients makes it prone to selection and observational biases, in addition to a high number of patients lost to follow-up, and the relatively short period of the latter, mostly imposed by the short life expectancy of a majority of the patients. Multi-center, large-sample comparative studies are needed for more robust results.
Conclusion
Return to a near pre-fracture functional level, and good radiologic outcomes can be expected of UHA irrespective of the amount of initial FNF displacement, and despite the advanced age and dependent status of the population. The present study adds up to the literature suggesting that the use of UHA may provide the same outcome as their bipolar counterparts with the advantage of being about 1000$ cheaper. This aspect of the surgical management should be taken into consideration as the number of hip procedures is expected to rise along with the growing elderly population, especially in developed countries where social security programs must be as cost-effective as possible.
Footnotes
Author Contributions
Surgery: S.B., G.V., S.D., and R.E. Study conceptualization and protocol: S.B. and S.D. Data collection: I.A. Data analysis: I.A. and J.G. Redaction: J.G. and G.V. Manuscript Correction: R.E.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.