
Abstract
Introduction
Fragility fracture of the pelvis (FFP), generally involving Rommens and Hoffman classification type IVb (H-shaped) requires spinopelvic fixation (SPF). We report the clinical outcome of sacroiliac rod fixation (SIRF) for FFP type IVb in a case series.
Materials and Methods
In this retrospective observational study, six patients (mean age, 80.3 years; range, 74-85 years) with FFP type IVb who underwent SIRF since October 2019 and could be followed up for ≥1 year postoperatively were included. All patients were injured in low-energy falls, a patient had a femoral neck fracture, and other had a humeral neck fracture and distal radius fracture.
Results
The mean (range) operative time was 135 (98-200) min, and mean blood loss was 103 (80-130) g. All patients achieved bone union in an average of 4.3 months. No implant failure or surgical site infection requiring reoperation occurred. No patient complained of iliac screw irritation or requested removal. One patient developed a T12 vertebral fracture at 3 weeks postoperatively. The mean final follow-up period was 17.8 months (13-22 months) and mean final modified Majeed Score (maximum 76 points as the items “work” and “sexual intercourse” were omitted for this study) was 71.7 (56-76).
Conclusions
SIRF is a less invasive surgical technique than SPF that uses only an S1 pedicle screw and iliac screw. SIRF using the “within ring” concept showed good clinical outcome in FFP type IVb.
Keywords
Introduction
Fragility fracture of the pelvis (FFP) reduces activities of daily living (ADL) in the elderly and has a 5-year survival rate similar to that of proximal femoral fracture. 1 Patients with FFP also have more osteoporosis and medical comorbidities than their peers, so systemic complications must be considered during treatment. Conservative therapy is the first choice for FFP without dislocation, but the decline in ADL during the treatment period should be minimized. Additionally, there are many issues to be considered in the surgical treatment of displaced FFP, such as indications, surgical techniques, invasiveness, and fixation in fragile bones.2,3 FFP causes major problems for the elderly. Recently, based on the Rommens and Hoffman classification, 4 minimally invasive surgery for early mobilization, 5 unstable fractures, and failed conservative treatments 3 has been reported.
The FFP Rommens and Hoffman classification type IVb (H-shaped) is characterized by a spinopelvic dissociation containing a bilateral vertical fracture through the lateral mass of the sacrum with a horizontal component connecting them. Generally, the FFP type IVb requires spinopelvic fixation (SPF), and clinical outcomes have been reported. 4 We have experienced several postoperative complications, such as pedicle screw backout of lumbar vertebra, in our SPF surgery cases.
A surgical technique for high-energy pelvic fractures, sacroiliac rod fixation (SIRF), was reported by Futamura et al. in 2018. 6 In a biomechanical experiment with bone model, it has been reported that SIRF provides fixation equivalent to SPF, assuming an AO classification 61C1.3. 7 In clinical practice, SIRF for high-energy unstable pelvic ring injuries, including H-type spinopelvic dissociation, has shown good clinical outcomes. 6
We hypothesized that SIRF would be an effective surgical technique for FFP type IVb and have used it in the surgical treatment of suitable patients. Here we report the clinical outcomes of SIRF for FFP type IVb in a case series.
Materials and Methods
Patients
Characteristics.

CCI = Charlson Comorbidity Index. ASA-PS = American Society of Anesthesiologists physical status. YAM = Young Adult Mean. BMD = Bone mineral density.
Operation
All surgeries were performed on the patient under general anesthesia in the prone position using titanium (Ti) alloy-based spinal instrumentation (ExpediumTM Spine System; DePuySynthes Co., Zuchwil, Switzerland). Skin incisions of 6-7 cm were placed medial to both posterior superior iliac spines (PSIS) (Figure 1A). The fascia was peeled away from the surfaces of the PSIS to develop sufficient space for manipulation of the iliac screws (IS) and S1 pedicle screws (S1PS). First, the bilateral S1PS were aimed at the promontorium and inserted via the tricortical orbit (Figure 1B). The entry point of the IS was set 2-3 cm distal to the head of the S1PS, and the longest and largest diameter bilateral IS was inserted from the PSIS to the anterior inferior iliac spine (Figure 1C). To prevent IS irritation, the IS head was inserted to the level of the posterior surface of the sacrum with sufficient PSIS resection. After cracking the base of the S1 spinous process subcutaneously, the IS on both sides were connected with Ti rods passed subcutaneously, and the S1PS and Ti rods were connected with 30-40-mm offset connectors (Figures 1D, E, F). The operation was completed by grafting a local bone taken from the iliac to the fracture site on the posterior surface of the sacrum. Overview of sacroiliac rod fixation. A: Skin incisions of 6-7 cm were placed medial to both the posterior superior iliac spines (PSIS). B: Bilateral S1 pedicle screws (S1PS) were inserted by tricortical orbit. C: Both the iliac screws (IS) and offset connectors were connected with a single rod. D: The IS on both sides were connected with a rod, and the S1PS and rod were connected with an offset connector. E, F: A postoperative plain radiograph and 3D computed tomographic image.
In all cases, the dislocation of the fracture was <1 cm, and no intraoperative reduction was performed. As a postoperative treatment, full weight-bearing rehabilitation was allowed immediately after surgery. Additionally, teriparatide was started in all patients after surgery. Subsequently, computed tomography (CT) was used to assess bone union. Bone continuity was determined in at least two planes in multiplanar reconstruction CT images to achieve bone union.
Results
Clinical outcome.
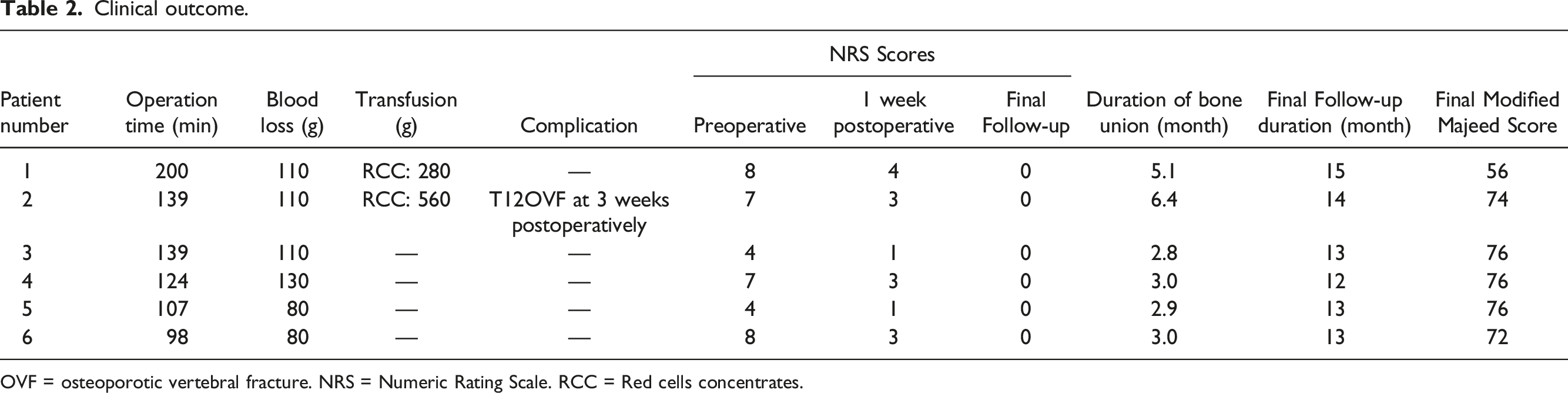
OVF = osteoporotic vertebral fracture. NRS = Numeric Rating Scale. RCC = Red cells concentrates.
The mean final follow-up period was 17.8 months (range, 13-22 months), the mean final modified Majeed Score (maximum 76 points as the items “work” and “sexual intercourse” were omitted for this study) was 71.7 (range, 56-76). Regarding ADL, 8 at the last follow-up, four patients could walk unassisted and two could walk with a walker.
Illustrative Case No.3
A 75-year-old woman had fallen 1 month earlier and developed buttock’s pain. She was diagnosed with lumbar spinal canal stenosis by her previous doctor and treated with medication, but her symptoms persisted, so she was referred to our hospital for consultation. On the initial examination, a plain radiograph showed a fracture of the left pubic rami (Figure 2A), and CT showed an H-shaped fracture of the sacrum (Figures 2B, C), so FFP type IVb was diagnosed. The NRS at that time was 4, and she had difficulty walking for a long time due to pain. SIRF was performed in response to failed conservative therapy due to delayed diagnosis (Figure 2D, E). The NRS at 1 week postoperatively was 1, which indicated a remarkable improvement. Bone union was achieved 3 months after surgery (Figures 2F, G). The modified Majeed Score at the last follow-up was 76. She is currently being followed up to the assess longer-term outcome. Illustrative case. A: A plain radiograph on initial examination: Fracture of the left pubic rami is shown. B, C: An axial and coronal CT image: An H-shaped fracture of the sacrum is shown (arrow), from which FFP type IVb was diagnosed. D, E: A postoperative plain radiograph. F, G: Postoperative computed tomographic image at 3 months: bone union was achieved.
Discussion
The typical posterior surgery for high-energy pelvic fractures is SPF or triangular osteosynthesis.9,10 Traditionally, high-energy H-shaped fractures of the sacrum have been considered an indication for SPF.
Although SPF is an effective technique, the mobile segment of the lumbosacral spine is included in the fixation, which leads to a constant risk of implant failure.11,12 However, Futamura et al. reported the use of SIRF with S1PS as an anchor. 6 Furthermore, in a biomechanical experiment using bone model, it has been reported that SIRF is equivalent to SPF in stiffness, deformation, horizontal resistance, and angular deformity, assuming an AO classification 61C1.3. 7 In clinical practice, SIRF has been performed for high-energy H-shaped fractures of the sacrum with good results. 6 The advantages of SIRF are that it is less invasive than SPF, and the “within ring” concept allows fixation to be completed in the pelvis, preserving the mobile segment. 6
There are few reports of surgery for FFP. Sacroplasty, 13 percutaneous screw fixation, 14 and trans-sacral positioning bar have been reported as typical techniques. 15 Recently, Maki et al. reported that SPF was performed for FFP type IVb with good clinical outcome. 16 SPF is a good technique for FFP as it provides strong fixation, but the longer operation and lumbosacral fixation is problematic, 15 and one report stated that SPF for FFP may be an overtreatment. 16
FFP is a fragility fracture due to osteoporosis without ligamentous injury, 4 which is different from high-energy pelvic fractures requiring ligamentous injury in terms of patient background.2,3,17 Therefore, it is questionable whether FFP and high-energy pelvic fractures should be treated with the same surgical technique, even if both are H-shaped fractures of the sacrum. In the surgery for FFP, since it is performed on elderly patients with osteoporosis, strong fixation is a prerequisite, and measures against SSI, skin ulceration, and screw irritation9,10 that may cause additional unscheduled surgery as well as fixation that reduces the risk of screw loosening and PS backout are required.16,18
This report appears to be the first on the application of SIRF to FFP type IVb. Bone union was achieved in all cases without any major complications, including implant failure, and the final score and clinical outcome were satisfactory. In applying SIRF to FFP, we have made several modifications to the original technique (Figure 3). Although our procedure is minimally invasive with only four anchors, the fixation strength should be ensured so that S1PS penetrates the promontorium (Figures 3A, B) and inserts via the tricortical trajectory.
19
The IS with a maximum possible diameter as well as with length >80 mm
20
and ≥9-90 mm is inserted in all cases (Figure 3C). In addition, to prevent pain and irritation at the screw insertion site, which is a major problem with use of the IS,
21
the IS head is inserted to the level of the posterior surface of the sacrum with sufficient PSIS resection (Figure 3D).
6
In this series, we were fortunate to have no case of SSI and no complaints of irritation of IS. The fixation is smaller than SPF, and it seems to be sufficiently minimally invasive in terms of operative time, blood loss, and 6-7 cm skin incision. The NRS scores at 1 week postoperatively also showed an early pain relief effect. So, far, there have been no implant failures under full weight-bearing immediately after surgery, and the technique seems to be suitable for elderly people who cannot leave their beds due to pain. SIRF for FFP type IVb, which conventionally requires SPF, seems to be a good technique because it provides strong fixation and minimizes the risk of implant failure because of the “within ring” concept. Modifications to apply sacroiliac rod fixation to fragility fracture of the pelvis. A, B: S1 pedicle screw penetrates the promontorium (arrow) and inserts by tricortical trajectory. C: The iliac screws (IS) are inserted with diameters as large as possible and longer than 80 mm. This patient received with IS ranging from 10.0-100-mm in diameter. D: To prevent IS irritation, the IS head is inserted to the level of the posterior surface of the sacrum with sufficient the posterior superior iliac spines resection (broken line).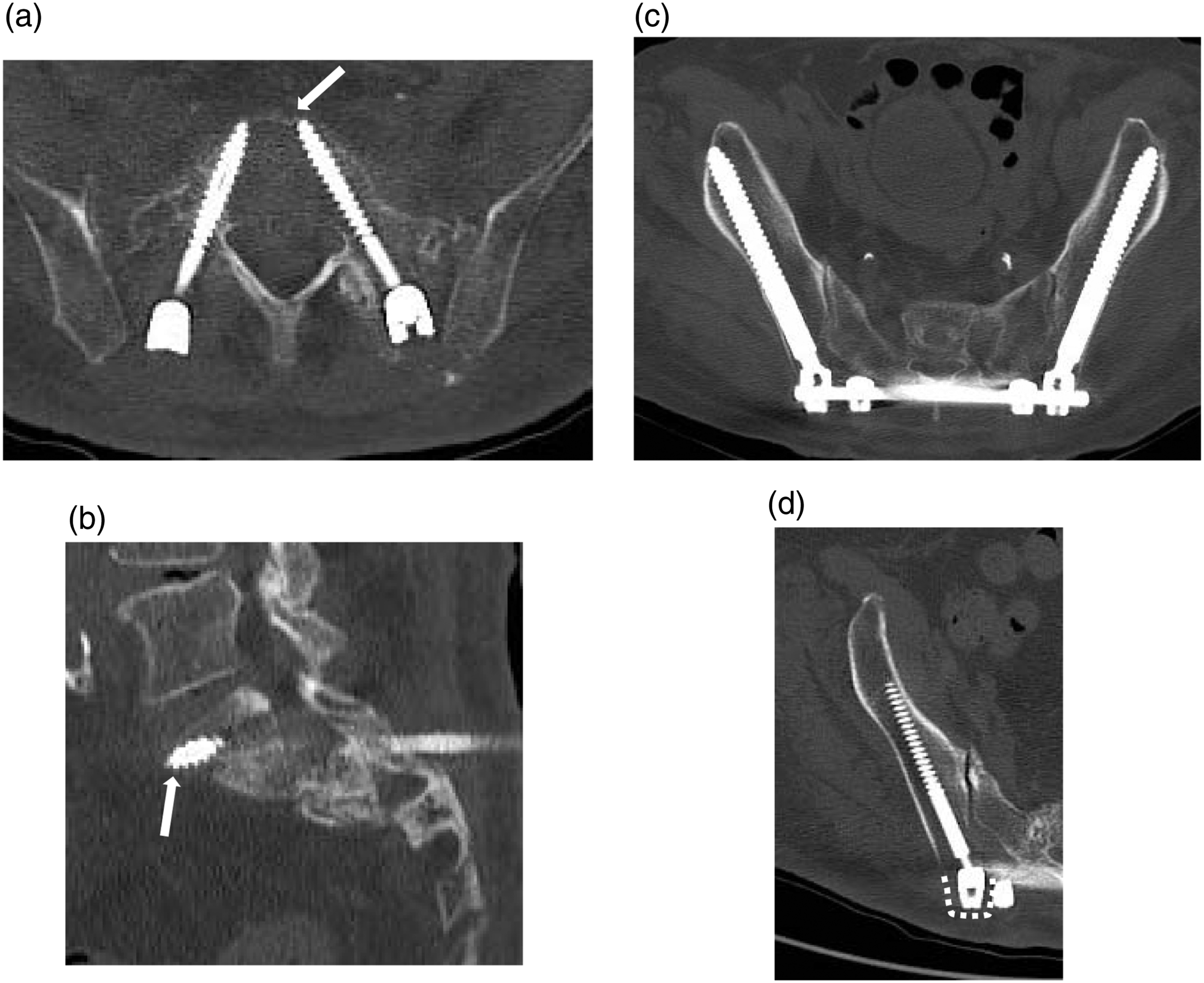
In addition, teriparatide was started in all patients after surgery as a countermeasure for elderly patients with osteoporosis. Teriparatide has been reported to be useful in spinal surgery to prevent screw loosening and in sacral fractures to improve pain early and promote bone union22-24 In this study, teriparatide was also introduced in all patients to promote bone union and prevent subsequent fractures. In all cases, bone union was achieved in an average of 4.3 months, and there was no screw loosening requiring reoperation. The patient with complications related to bone metabolism (No.1) and the patient with more severe osteoporosis (No.2) required a longer duration of bone union than other patients. Therefore, using teriparatide is important for these patients to achieve bone union, even if it takes a longer duration. Only one patient developed a T12 vertebral body fracture postoperatively, and no subsequent fracture was observed during the follow-up period in the other patients.
There were several limitations in our case series. This was a small retrospective series and patients had small displacement. In patients with large vertical displacement, SPF may be indicated by the results of biomechanical experiments. 7 Generally, the S2 alar-iliac (SAI) screw is superior to the IS in terms of complications. 21 However, we used the IS because of the possibility of screw entry through the fracture in our case series. Additional research is needed to determine whether the SAI screw or the IS is superior in SIRF. In addition, since the sacroiliac joint is included in the fixation, there is a possibility that the S1PS or IS may loosen. Long-term follow-up with more cases is necessary.
Conclusion
In conclusion, SIRF using the “within ring” concept showed good clinical outcomes in FFP type IVb, which was previously thought to require SPF. SIRF is a minimally invasive and mobile segment-preserving fixation method suitable for the elderly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics
This research has been conducted according to the World Medical Association Declaration of Helsinki. All procedures including review of patient records used in this research were approved by the institutional review board of our institution. Verbal informed consents were obtained from all patients to participate in this study. An IRB approve the study and the procedure outlined for the verbal consent obtainment.
Data Availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.