
Abstract
Introduction
Increasing incidence of fragility fractures has spurred development of protocols, largely focused on peri-operative care, with numerous proven benefits. The purpose of this investigation was to evaluate outcomes of our hip fracture treatment program regarding successful protocol implementation, compliance, effect on subsequent fracture rates, and mortality during the first decade of adoption.
Methods
A retrospective review identified patients >65 years old with fragility hip fractures between 2010 and 2022. The HiROC (+) cohort consisted of patients who received a “High-Risk Osteoporosis Clinic” (HiROC) referral for bone health evaluation and bisphosphonate initiation as indicated. Additional fracture rates and mortality at 3 years were calculated. Protocol implementation and compliance over the first 10 years was analyzed in the four identified cohorts.
Results
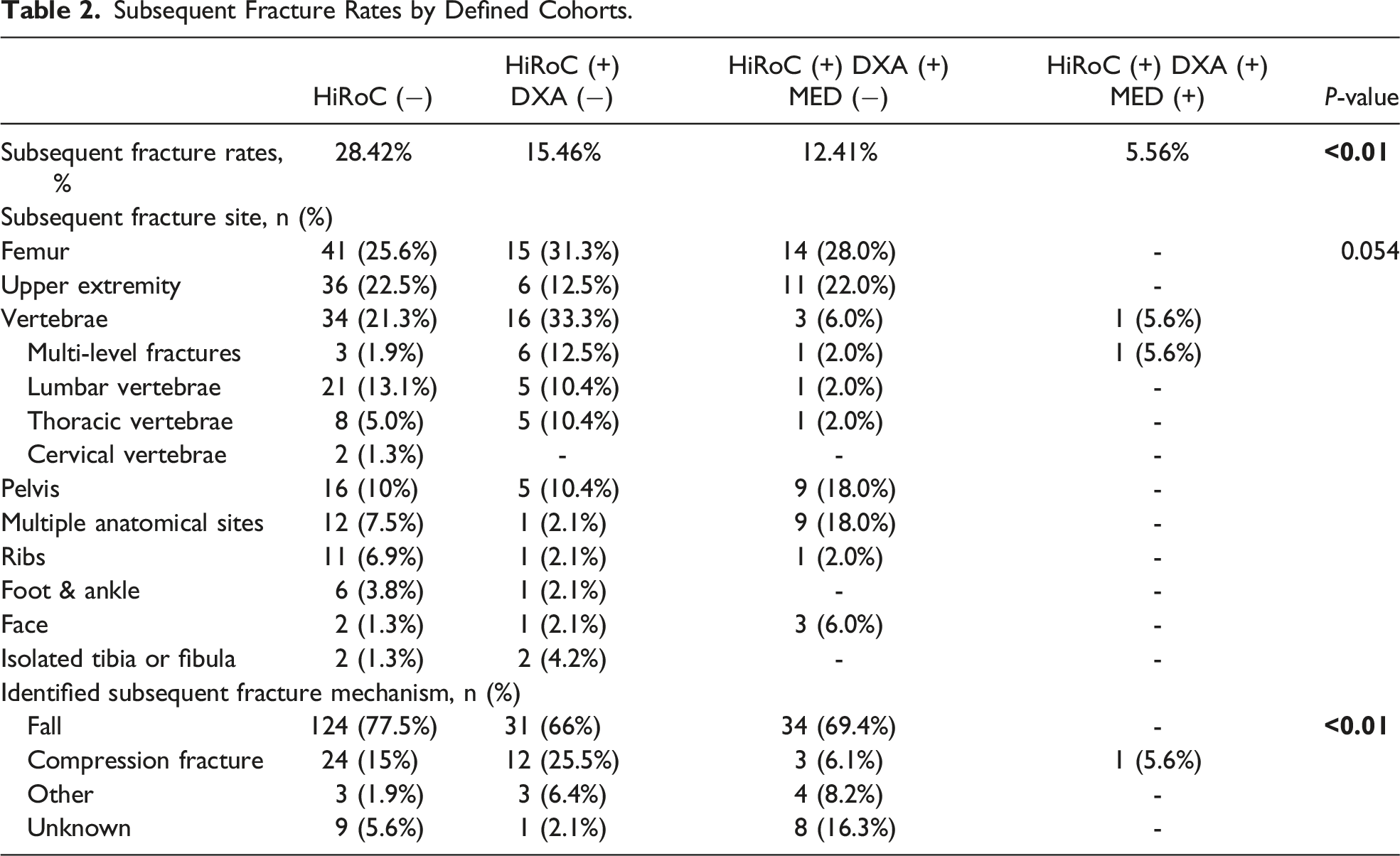
A total of 1671 fragility hip fractures were identified, with 386 excluded due to insufficient follow-up, with an average age of 81.6 years and a median follow-up of 36.4 months. Of the 1280 included cases, 56% (n = 717) had a HiROC referral placed. HiROC(+) groups had lower subsequent fracture rates at two years, compared to those without referral (28% vs 13%, P < 0.0001) and those completing more steps of the protocol had lower subsequent fracture rates (28% vs 15% vs 13% vs 5%, P < 0.0001). No statistically significant difference was observed between the cohorts for anatomic site of subsequent fractures.
Discussion
Greater than half of all eligible patients were successfully captured by the protocol. Patients completing more steps of the protocol had lower subsequent fracture rates. Captured patients demonstrated reduced mortality rates when compared to current literature.
Conclusion
Successful implementation of this geriatric hip fracture protocol was associated with reduced additional fractures and mortality rates. Identifying steps of process failures in the protocol can provide opportunities for increased compliance and reduction in future fracture occurrences.
Introduction
Each year, greater than 300,000 geriatric Americans sustain a hip fracture, creating an estimated $5.96 billion financial burden.1,2 Beginning at age 50, there is an increased risk for a fragility fracture, defined as low-energy trauma that most commonly results in a hip, vertebral, wrist, or proximal humerus fracture.3-5 While bone mineral density is a strong predictor of future fragility fracture, risk of fragility fracture sharply increases in those ≥65 years of age, independent of their bone mineral density.3-6 Recent literature supports a trend towards a decreasing incident rate of hip fractures, likely attributable to a better understanding of risk factors, prevention strategies, and pharmaceutical prophylaxis. 7 However, the overall number of hip fractures is expected to increase due to the growth of the geriatric population. In 2010, there were approximately 40.5 million persons over the age of 65 living in the United States.8,9 By 2040, that number is projected to nearly double to include 80.8 million elderly Americans.
There is a substantial amount of literature describing factors that can improve outcomes in fragility hip fracture patients including multidisciplinary care, medical optimization, surgery within 24 hours, regional nerve blocks, early mobilization, and nutritional optimization.10-14 While articles on treatment far outnumber available literature on fracture prevention, the high mortality rate and financial burden associated with fragility hip fractures make it important to identify effective prevention strategies. One method is the creation of multi-disciplinary fragility fracture programs. Recent literature following fragility hip fracture patients before and after implementation of a protocol demonstrated a significant increase in prescription of anti-osteoporotic medications and medication adherence. 15 These programs have shown reduced healthcare facility admissions and increased hospital-free survival times.13,14 Furthermore, studies with 3 to 5-year follow-up found all-cause mortality to be lower in patients after protocol initiation.13,14 However, literature varies regarding fragility fracture program effectiveness on the incidence of subsequent fractures.13,14,16-18
Reported success of international programs, benefitted by centralized healthcare with standardized treatment protocols, spurred US efforts to bring attention to and address fragility fractures beginning in 2009 with the American Orthopaedic Association “Own The Bone” campaign.18-21 This program is a nationwide, systems-based multidisciplinary fragility fracture prevention initiative. 21 The International Geriatric Fracture Society was created in 2012 to address fragility fractures through collaboration and distribution of proven principles and protocols. 22 While current AAOS clinical guidelines support evidence-based osteoporosis management, they lack further recommendations on successful implementation of such programs in institutions without existing protocols, particularly those with fewer available resources 23 Our integrated healthcare system provides ease of access to diagnostic studies and an environment that allows a comprehensive continuum of care for management of bone health.
This study aimed to assess successful enrollment to our institution’s standardized fragility hip fracture protocol. Secondary aims included compliance with diagnostic testing, utilization of pharmaceutical treatment, subsequent fracture rates, and mortality. We hypothesized that successful implementation of the institutional geriatric fragility hip fracture protocol would be associated with reduced subsequent fracture rates.
Methods
Design
An IRB exemption was obtained for this retrospective study. A review was performed of fragility hip fractures that presented to our rural healthcare institution, which is a tertiary care facility in the northeast U.S. For this study, a fragility hip fracture was defined as any proximal femur fracture secondary to low-energy trauma. The institution’s protocol was designed to capture geriatric patients, therefore individuals aged 65 years or older were included. A subsequent fracture was defined as any fracture, fragility or traumatic, that occurred within two years of the initial fragility hip fracture.
Study Population
Patients evaluated and treated for hip fractures were identified by ICD-10 codes related to femur fracture, hip fracture, and age-related osteoporosis with current femur fracture. The list of ICD 10 codes used can be found in Appendix 1. All persons aged less than 65 years or patients with less than 2 years of follow-up were excluded. The study timeframe began with the implementation of the program on 07/01/2010 through 12/31/2022, allowing a decade of patients with minimum 2 year follow up.
Protocol
All eligible patients were to receive a HiROC (High Risk Osteoporosis Clinic) referral within 90 days of the initial fracture. Patients were then seen by rheumatology via telehealth or in office. The HiROC medical consultants initiated a bone health evaluation which included patient history, pertinent medical information, laboratory testing (calcium, 25-hydroxyvitamin D, alkaline phosphatase, PTH (intact), and TSH), bone density DEXA scans, and risk scoring using the Fracture Risk Assessment Tool (FRAX). 24 Upon completion of the laboratory testing and DEXA scan, patients were to follow up with the HiROC medical consultants for osteoporosis pharmacotherapy initiation, if indicated.
Patients who received a HiROC referral by the managing provider within 90 days of their presenting hip fragility fracture comprised the “HiROC (+)” cohort. Patients without a referral within 90 days of their initial fragility hip fracture constituted the HiROC (−) cohort. Similarly, patients with a subsequent DEXA scan comprised the “HiROC (+), DEXA (+)” cohort. The same nomenclature was applied to bisphosphonate orders: patients with a bisphosphonate order formed the “HiROC (+), DEXA (+), MED (+)” cohort (Figure 1). A flow chart illustrating the protocol pathway and sample size in each cohort. HiROC, High risk osteoporosis clinic; DXA, dual-energy x-ray absorptiometry; MED, medication.
Outcome Measures
The primary aim of the study was evaluation of successful recruitment to the fragility fracture program, defined as a provider compliance with placement of the HiROC referral order within 90 days of fracture presentation. Secondary aims included the percentage of patients who completed their DEXA scan, those started on osteoporosis pharmacotherapy, rate of subsequent fracture, and 3-year mortality rate.
Statistical Analysis
Descriptive statistics were utilized for patient demographics and subsequent fracture rates. Frequency and percentages were reported for categorical variables, and the mean and standard deviation (SD) were reported for continuous variables. Statistical comparisons between groups were made using chi-square, Fisher’s exact test, and student t-test where appropriate. P-values of <0.05 were considered statistically significant. All statistical analyses were performed using SPSS version 28.0.0.0 (IBM Corp., Armonk, NY).
Post-Hoc Power Analysis
A post-hoc power analysis was performed for the comparison of subsequent fracture rates between the patients with and without a HiROC referral. Given the sample size and proportions in the study, the post-hoc power analysis showed 100% for detecting subsequent fracture rates between patients with and without a HiROC referral. Additional post-hoc power analyses were performed for a comparison of subsequent fracture rates for patients with a referral placed but with different levels of the treatment protocol completed. These power calculations revealed that our investigation was underpowered to detect statistically significant differences given the sample size and proportions for these secondary comparisons. All power analyses were performed using G-power, a free-to-use power analysis program.25,26
Results
Demographics of the Included Patient Population.

Subsequent Fracture Rates by Defined Cohorts.
Discussion
The results indicate that our protocol was successfully initiated in more than half of hip fragility fracture patients. With a referral rate of 56%, the placement of HiROC referral orders offers the greatest opportunity for improvement. A study by Vranken et al found a 53% successful recruitment to fracture liaison services. 14 Another study by Nakayama et al found an 80% successful recruitment rate. 16 In our study, from the year 2010 to 2018, fragility hip fracture patients were admitted to the institution’s hospitalist service. Starting in 2018, these patients were admitted to the trauma service due to institutional protocol policy change. This shift in care may have resulted in fewer HiROC referrals due to inadequate interdisciplinary communication of the protocol and eligibility criteria.
Regarding the patient’s progression through the protocol, 58% of patients that received the HiROC referral completed their DEXA scan. This rate of compliance reinforces that initial recruitment remains a critical step for success. While there are many pharmacotherapies available, first line treatment remains Vitamin D and Calcium supplementation and a bisphosphonate, when indicated by the current clinical guidelines.5,21,27 Increased medication initiation rates from 12% to 78% have been attributed to the implementation of an effective fragility fracture protocol. 15 After investigating prescription data at our institution, we found a 4.3% bisphosphonate initiation rate. Renal disease is a contraindication to bisphosphonates, however, our rate of 4.3% is significantly lower than Vranken et al who reported 40% initiation of anti-osteoporotic medication. 14 While there are risks associated with bisphosphonate treatments, the HORIZON study of over 1000 patients demonstrated no impact on fracture healing, osteonecrosis of the jaw, nor difference in renal or cardiovascular adverse events between groups. 28 Moreover, Teriparatide has been shown to benefit bone healing and alendronate improved femoral head screw fixation in the setting of osteoporotic fracture.3,29,30
When stratified by implementation of sequential steps of HiROC protocol, patients completing more steps had lower subsequent fracture rates. In patients receiving the HiROC referral (HiROC(+)), there was a 15% decrease in subsequent fracture rate. The landmark HORIZON study, a randomized, double-blinded, placebo-controlled trial, found a subsequent fracture risk reduction of 35% in patients started on annual zoledronic acid within 30 days of a geriatric hip fracture. 28 Our findings are consistent with other retrospective studies reporting 30%-50% decreased risk of subsequent fractures.14,16,17
Our study population averaged a 15.6% mortality rate at three years. Reported mortality rates at 3-years have ranged from 33-40% in recent literature, in the absence of a hip fracture protocol.31-34 Compared to these prior reports, the significant reduction in our mortality rate may reflect the effectiveness of protocol initiation in promoting longevity after sustaining a fragility hip fracture. While groups that completed more steps of the protocol demonstrated decreased mortality rates, the pharmacotherapy group was underpowered for further statistical analysis.
As a retrospective study, identifying patients for inclusion is limited by the accuracy of documentation in the electronic medical record and may not capture all eligible patients. A challenge in this study, and commonly encountered in other geriatric fracture studies, is the substantial number of patients lost to follow-up. 35 While the rate of HiROC consult placement is impacted by provider consistency, the secondary aims of DEXA completion and bisphosphonate initiation may be subject to selection bias with healthier patients having greater physical capability and access to resources to complete these steps.
Literature strongly supports co-management of fragility hip fracture patients with geriatric teams throughout treatment. 36 Due to lack of geriatric specialists at the study institution, the rheumatology department served as the HiROC medical consultants executing the testing, diagnosis, and treatment of osteoporosis. Preliminary quality improvement efforts to identify obstacles to successful implementation at this institution suggested scheduling to be a significant barrier. Access to HiROC consultants within 90 days of the fracture was challenged by provider availability. Those patients successfully scheduled for evaluation may have encountered difficulty attending these appointments due to ongoing inpatient status or lack of transportation from rehabilitation facilities. Patient “no-shows” may also be attributed to lack of patient understanding or education regarding the intended purpose and importance of follow-up appointments. Many successful fracture liaison programs include a team dedicated solely to coordination of protocol steps. 13 These programs have demonstrated particular usefulness in overcoming non-clinical, educational, and financial barriers, with earlier recruitment to fracture programs and greater patient retention throughout the follow-up period. 13 Institutions have been limited by lack of physician extenders to assume nurse navigator or coordination roles. 4 While the timeframe of the inclusion criteria preceded the onset of COVID-19, the follow-up period did overlap with the pandemic which may have altered care pathways. 37 Future studies should include a focus on identifying obstacles in the protocol to enhance the program’s success, including implementation of a nurse navigator to guide care coordination and patient education.
The strengths of this study include: a 10-year evaluation of institutional geriatric hip fracture program, a minimum of two years follow-up and a large population size that was treated at a single integrated healthcare system.
Conclusion
This study supports the value of institutional fragility hip fracture programs. Patients obtaining a HiROC referral demonstrated a lower subsequent fracture rate at a minimum of two years follow-up. Despite this demonstrated benefit, our institution only achieved a 56% referral rate for patients presenting with a fragility hip fracture. Initial HiROC referral placement and subsequent patient compliance are key to potentially achieve better bone health as demonstrated by decrease subsequent fracture and mortality rates. Future investigations to identify specific process failures will allow opportunities for improvement in both provider and patient compliance with implemented protocols.
Footnotes
Acknowledgement
We would like to thank all the clinicians and patients who participated in our study.
Author Contributions
AH interpreted the data, wrote the first draft of the manuscript and subsequent revisions. OY analyzed and interpreted the data, provided statistical analysis, and assisted in manuscript revisions. DK designed and directed the project and assisted with manuscript revisions. JW and AP performed data collection. KK designed and directed the project. B designed and directed the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Statement
This was a retrospective review and deemed eligible for IRB exemption as defined in the U. S. Department of Health and Human Services Regulations for the Protection of Human Subjects [(45 CFR 46.104)].
Presentations
The study was presented at the American Academy of Orthopaedic Surgeons 2024 Annual Meeting (Podium presentation, San Francisco, CA, 02/15/2024).
Appendix
List showing the included ICD10 codes for identifying hip fracturtes.
S72.001A
M80.00XA
M80.059A
S72.002A
S72.92XA
S72.142A
M80.052S
M80.051D
M80.052G
M80.051A
M80.059S
S72.001A, S72.002A
M80.052D
M80.052A
M80.051S
S72.092A
M80.011D
M80.052K
M80.851A
M80.851D
M80.851S
M80.851P
S72.141 A, S72.142A
M80.852D
M80.051K
M80.052P
M80.059D