
Abstract
Objective
In recent years, many studies have reported good results with total hip arthroplasty (THA) for displaced femoral neck fractures (FNFs). However, no study has reported the clinical outcomes of the anterolateral modified Watson–Jones THA (MWJ-THA) for displaced FNFs. This study aimed to investigate the clinical results of THA for displaced FNFs at our hospital and to discuss the advantages of MWJ-THA over THA with other approaches for displaced FNFs.
Methods
Forty-three patients who underwent MWJ-THA for displaced FNFs were included in this study. Patient characteristics, preinjury walking ability, activities of daily living, implants used, walking ability (at 1, 3, and 6 months after surgery), cup placement angle, clinical hip score, surgical complications, revision surgery, and death within 1 year after surgery were investigated.
Results
The mean age of the 43 patients was 63.3 years, and the mean body mass index (kg/m2) was 21.1. Regarding the heads used, 28-mm heads were used in 4 patients, 32-mm heads were used in 32 patients, and 36-mm heads were used in 7 patients. The cups were placed in the Lewinnek safety zone (93.0%). Four patients had stem sinkage of a few millimeters. 6 months postoperatively, 38 patients walked unaided, and 4 patients walked with a cane. The Harris Hip Score averaged over 90 points at all time points. No postoperative dislocation was observed. Two patients died within 1 year postoperatively.
Conclusion
In this study, MWJ-THA was performed for displaced FNFs and resulted in no postoperative dislocations. Furthermore, more than 90% of the patients regained their preinjury walking ability at 6 months postoperatively. MWJ-THA has great dislocation control and is effective in treating displaced FNFs.
Keywords
Introduction
The number of femoral neck fractures (FNFs) in the elderly has been increasing in recent years and is expected to continue to increase. 1 Surgical intervention, such as osteosynthesis, hemiarthroplasty (HA), and total hip arthroplasty (THA), is recommended as the treatment method. When arthroplasty is chosen, hip hemiarthroplasty is recommended for those with low physical activity due to debate over unipolar vs bipolar hemiarthroplasty. However, THA has better long-term results than HA and is often performed in highly active patients, particularly because of less cartilage damage on the postoperative acetabular side. 2
In recent years, the use of THA for FNFs has been increasing because of the increase in healthy life expectancy and the number of highly active elderly patients. 3 However, high postoperative dislocation rates have become a problem. The early postoperative dislocation rate of THA for FNFs was 3.4%, 4 which is 2 to 4 times higher than that of THA for osteoarthritis.4,5 In particular, the posterior approach has been reported to have a dislocation rate of 3%–8%.5,6 Several studies that compared the postoperative dislocation rates of THA and HA reported dislocation rates of 4%–6% for THA and 0%–2.5% for HA.7-9
In our hospital, we chose HA for displaced FNFs in elderly patients with low activity and THA for displaced FNFs in elderly patients with high activity, patients with rheumatoid arthritis, and patients with developmental dysplasia of the hip (DDH). In most cases, we used the anterolateral modified Watson–Jones (MWJ) approach, which is a musculotendon-sparing approach described by Röttinger et al. 10
In recent years, many studies have reported good results with THA for displaced FNFs, but no study has reported the clinical results of MWJ-THA for displaced FNFs. This study aimed to investigate the clinical results of THA for displaced FNFs at our hospital and to discuss the advantages of MWJ-THA over THA with other approaches for displaced FNFs.
Subjects and Methods
This was a retrospective analysis of 59 patients who were admitted to a single institution between April 2008 and March 2021, diagnosed with displaced FNFs, and underwent THA. Two patients underwent THA via a posterior approach were excluded from this study. 57 patients underwent THA via MWJ-THA. The exclusion criteria were having less than 12 months of follow-up (n = 5) and the use of dual mobility cups (DMCs) for comparison with previous studies which used fixed-bearing cups for displaced FNFs (n = 9). Ultimately, 43 patients were included in the study (Figure 1). The investigative protocol was approved by the Institutional Ethics Committee. All patients provided informed consent in accordance with the requirements of this review. Patient’s selection study flow chart.
Evaluation and Outcomes
We assessed patient characteristics such as age, sex, body mass index (BMI), comorbidities (other trauma, mental disorders, neuromuscular disorders, rheumatoid arthritis, and history of steroid use), pre-injury walking ability, activities of daily living (ADLs), and surgical risks determined by the anesthesiologist according to the American Society of Anesthesiologists (ASA) classification. 11 Surgical information, such as the waiting period for surgery, surgical time, blood loss, use of tranexamic acid, perioperative blood transfusion, and discharge destination, was investigated. Finally, implant information was evaluated.
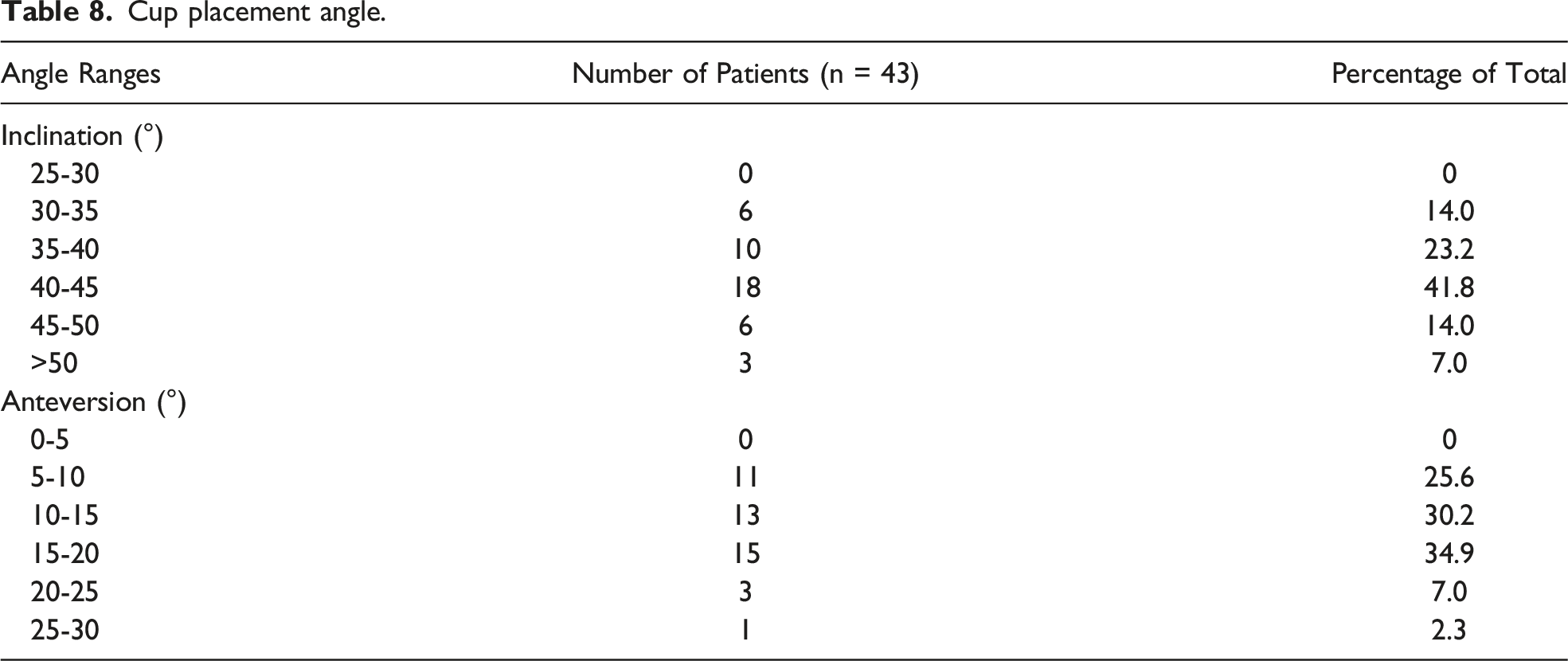
For the cup placement angle, the following method was used to evaluate the cups: 1 week after surgery, anteroposterior (AP) radiographs of the pelvis were obtained by focusing on the superior border of the pubic symphysis and were used to evaluate the cup alignment. One examiner (NT) measured cup alignment using Lewinnek’s method. 12 Whether the cup was tilted anteriorly or posteriorly was determined using lateral radiographs of the cross table. To measure cup alignment, the method of Lewinnek et al 12 (anteversion: 5°–25°; inclination: 30°–50°) was used as a safety zone.
Walking ability was assessed 1, 3, 6, and 12 months postoperatively. Walking ability was stratified into the following 5 categories: (1) use of a wheelchair or no walking, (2) use of a walker, (3) use of crutches, (4) use of a 1 stick, and (5) independent gait. The clinical hip score (Harris Hip Score [HHS]) was assessed at 3 months, 6 months, 12 months, and at the last follow-up after 12 months postoperatively. Complications from surgery (dislocation, nerve injury, intraoperative fracture, and postoperative fracture), revision surgery, and death within 1 year postoperatively were investigated. The cup placement angle and stem sinking/loosening were investigated using imaging evaluations.
Operative Procedure
MWJ-THA is a lateral supine anterolateral musculotendon-sparing procedure that was reported by Röttinger et al. 10 A unique feature of this surgical entry technique is intermuscular entry, which is performed from the anterolateral side between the gluteus medius and tensor fasciae latae. Although not described in the original technique, the incised capsular ligament was preserved and repaired. The cups were set with reference to the alignment guide (operative anteversion, 20°; operative inclination, 40°). The surgery was performed or supervised by an experienced hip surgeon.
Results
Patient Characteristics, Operative Information, and Implant Information
Patient Characteristics.

Operative Information.
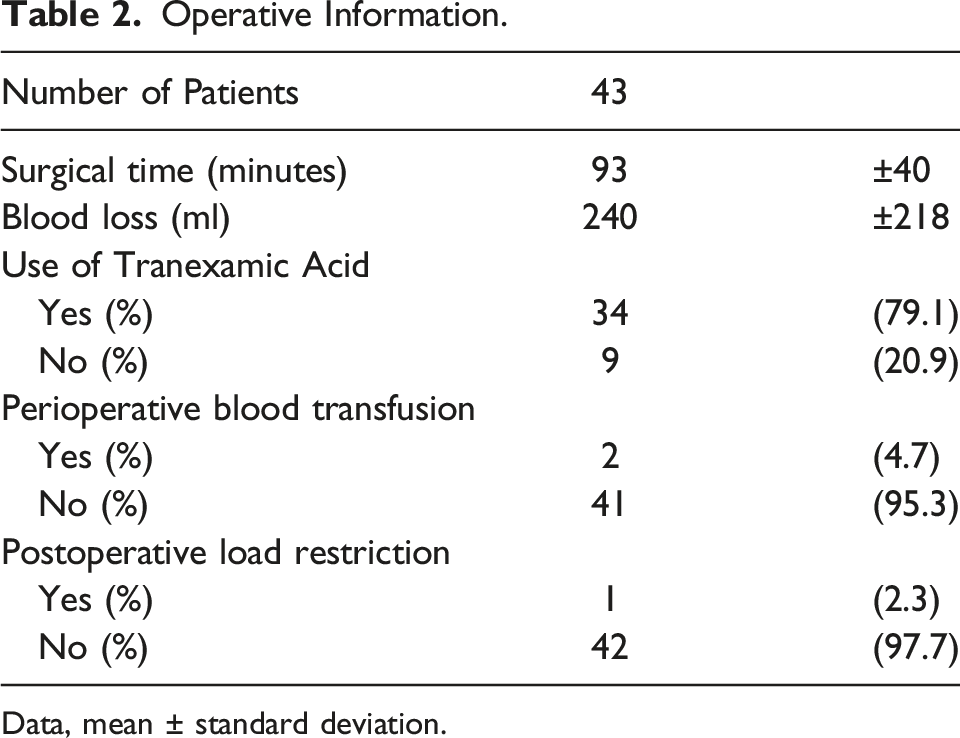
Data, mean ± standard deviation.
The mean operative time was 91 min, and the mean blood loss was 266 mL. Tranexamic acid was administered during surgery starting in September 2013, and no patient required a blood transfusion after the administration of tranexamic acid. Postoperatively, all patients were allowed to walk with full load from the day after surgery, except for 1 patient who had multiple lower extremity injuries. All patients were rehabilitated beginning from the day after surgery without any limitation of the range of motion.
Implant Information.

Outcomes
Walking Ability.

Clinical hip score (Harris Hip Score).

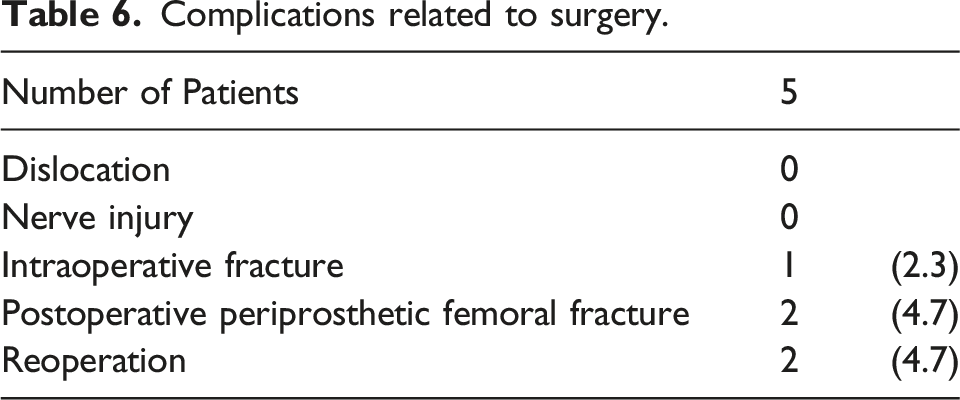
Complications related to surgery.
Deaths within 1 year after surgery.

Cup placement angle.
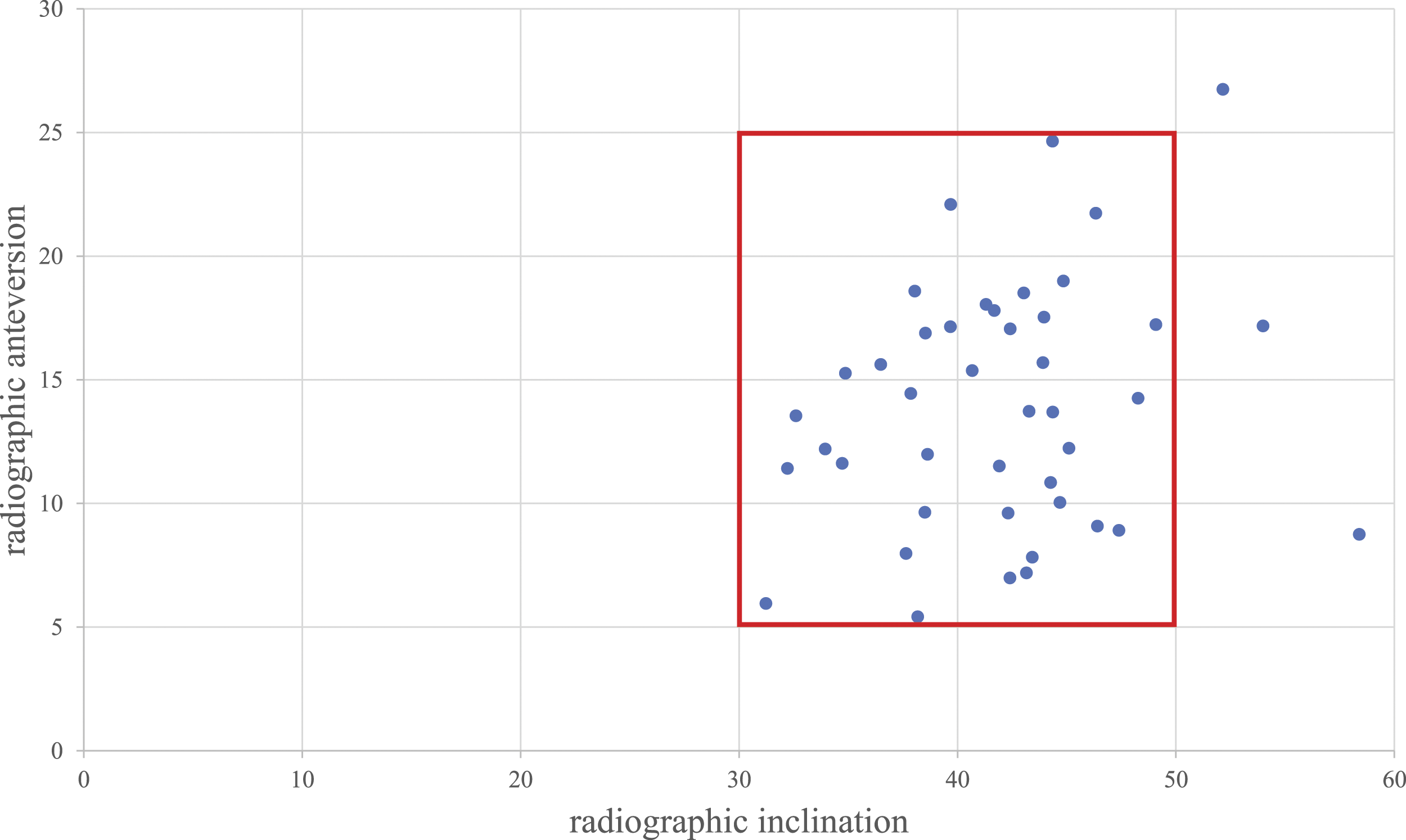
Scatter diagram of cup orientation. The y-axis shows radiographic inclination and the x-axis shows radiographic anteversion. The red box shows the Lewinnek safe zone.
Discussion
We studied the clinical outcomes of 43 patients who underwent MWJ-THA with fixed-bearing cups for displaced FNFs. There were no postoperative dislocations, and the mean HHS score was more than 90 points at 3 months postoperatively. In terms of walking ability, 90.5% of patients were able to walk independently at 6 months postoperatively, and 92.9% of patients regained their preinjury walking ability.
THA for FNFs is known to have a higher postoperative dislocation rate than THA for osteoarthritis4,5 and is associated with higher dislocation rates than HAs.7-9,14 There are several reasons for this finding. First, the soft tissues and muscles around the hip play an important role in joint stability; however, displaced fractures of the femoral neck are considered acute trauma, and damage to this area can lead to postoperative instability.15-17 Second, a good preoperative range of motion was maintained postoperatively with THA.7-9,14 Third, THA is more prone to dislocations than HA because the former uses a smaller head than the latter.7-9,14
Dislocation rates differ depending on the surgical approach used. The anterior approach has been reported to have a lower dislocation rate than the posterior approach. 18 Noticewala et al 19 studied 66 patients who underwent THA with a posterior approach for FNFs. Four cases (6.1%) of dislocations occurred within 6 months postoperatively. The head size was similar to that of the current study. 19 Patient age and BMI were higher than those in the current study, but previous large-scale studies have shown that age and BMI are not risk factors for dislocation.20,21
Summary of the Literature on the Mortality and Dislocation Rates in Different Approaches.

BMI, Body Mass Index; MWJ, Modified Watson–Jones approach; DAA, Direct Anterior Approach
MWJ-THA has the potential to solve these problems. We believe that it offers good protection against posterior dislocation because it preserves the posterior muscle groups, and impingement in the extended position can be checked intraoperatively because the surgery is performed in the lateral supine position.
In addition, proper cup placement is essential to prevent dislocation. In this study, it was placed in 93.0% accuracy within the Lewinnek safety zone. 12 Cup placement with an alignment guide in the lateral supine position is inferior to that in the supine position. However, in our previous report, the accuracy of freehand cup placement in the MWJ approach was 92.8% in the Lewinnek safe zone and 74% in the Callanan safe zone. This indicates that our cup installation was sufficiently accurate. 27 A similar result was observed in the present study. Also, through this approach there were no cups placed in retroversion, which is likely approach-related and contributes to the lack of dislocations.
The HHS in this study averaged >90 points at all time points. In a study comparing the anterior approach with other approaches, no significant differences were found; however, the median HHS score was higher in the anterior approach (94 points). The length of hospital stay was significantly shorter with the anterior approach than with the posterior approach, and better results were attributed to earlier ambulation and rehabilitation. 28
In this study, periprosthetic fractures due to falls were observed in 2 patients after surgery: 1 occurred at 3 weeks post-surgery, and the other occurred at 5 months post-surgery. These patients required reoperation. Patients with proximal femoral fractures have a higher risk of falling within the first month after surgery 29 and that a second fracture at the same site is more likely to occur within 48 months after injury. 30 Patients who sustain proximal femoral fractures should be cautious about postoperative falls and fractures.
This study had several limitations. First, this was a retrospective cohort study, and it is possible that some information was incomplete. However, because patient data were recorded and available in the electronic medical records used in our hospital, there were no significant differences and the overall outcome was not affected. Second, this study did not include a control group that received other treatments. Considering that the posterior approach has been reported to have a high dislocation rate, we could not use such a technique in the control group because of ethical issues. Therefore, we compared MWJ THA and HA using the posterior approach performed at our hospital. Third, the follow-up period in this study was relatively short. However, given that most complications in trauma patients occur in the early postoperative period, the present results may have been sufficient to examine the clinical outcomes of MWJ-THA for FNFs. Fourth, we cannot rule out the possibility of patient selection bias. At our institution, THA for displaced FNFs is limited to highly active patients and those with rheumatoid arthritis and DDH. The mean and median patient ages in our study were 63.3 and 65 years, respectively, which are lower than those reported in other studies. The relatively low age may have affected the results because older patients tend to have more comorbidities and higher mortality rates than younger patients.
Conclusion
We investigated the clinical outcomes of MWJ-THA for displaced FNFs at our institution. There were no cases of postoperative dislocation. Furthermore, more than 80% of the patients regained their preinjury walking ability and had good clinical scores. We will continue to follow-up patients and compare their results with those of other approaches and implants.
Footnotes
Acknowledgments
We thank to Department of General Affairs in Toyama Prefectural Central Hospital for data organization.
Authors contribution
All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors. All authors are in agreement with the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.