
Abstract
Introduction
The Disabilities of the Arm, Shoulder and Hand (DASH) survey estimates the upper limbs’ dysfunction in one score, but limited evidence exists to justify use of DASH to screen older adults for shoulder dysfunction at routine health maintenance primary care visits. We sought (1) to determine if the DASH, American Shoulder and Elbow Surgeons (ASES) and Simple Shoulder Test (SST) surveys are related to one another and (2) to determine the relationship of DASH, ASES and SST scores with 36-Item Short Form (SF-36) subscales, shoulder forward flexion range of motion (FF-ROM) and abduction (ABD-ROM) in older adults.
Methods
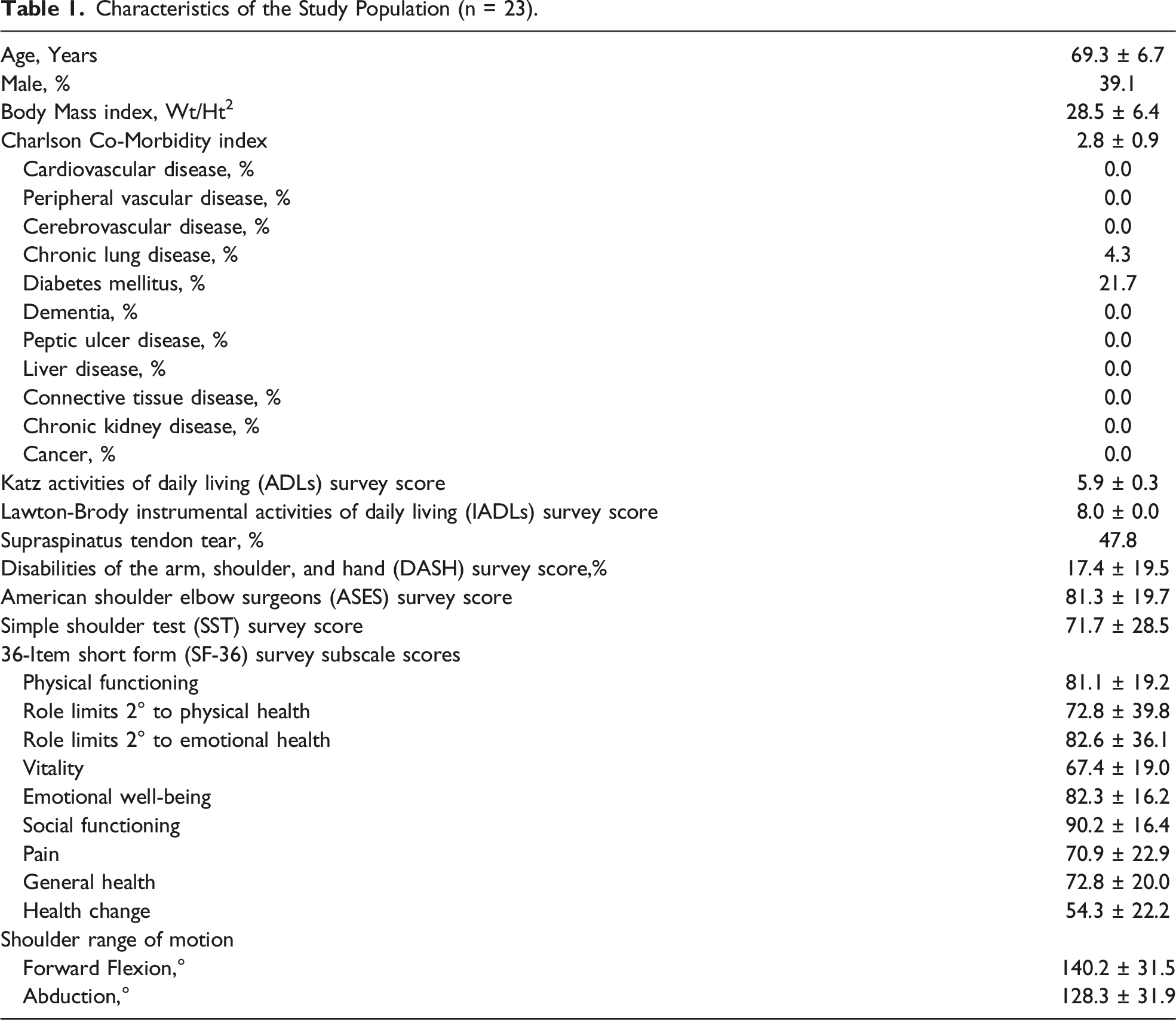
Prospective pilot study of 23 community-dwelling adult volunteers [mean age (± standard deviation), 69.3 ± 6.7 years; range, 61-84 years, with no rotator cuff repair or joint replacement. Shoulder MRI, ROM testing, DASH, ASES, SST, SF-36, Katz activities of daily living (ADLs), and Lawton-Brody instrumental ADLs (IADLs) were completed at one time point. Descriptive and correlation analyses were performed.
Results
Means: DASH, 17.4 ± 19.5; ASES, 81.3 ± 19.7; SST, 71.7 ± 28.5; Katz ADLs, 5.9 ± .3; Lawton-Brody IADLs, 8.0 ± .0; FF-ROM, 140.2° ± 31.5°; and ABD-ROM, 128.3° ± 31.9°. Nearly 48% had supraspinatus tendon tear. Correlation among DASH, ASES, and SST was strong (|rho ≥.88|; P < .001). DASH, ASES, and SST had strong correlation (|rho ≥.71|;P < .001) with shoulder FF-ROM and ABD-ROM. DASH had near equivalent or slightly stronger correlation for all SF-36 subscales relative to ASES and SST. DASH showed strong or moderate correlation (P < .05) to most SF-36 subscales.
Conclusion
DASH, ASES and SST strongly correlated with one another. DASH, relative to ASES and SST, has similar correlation to shoulder FF-ROM, ABD-ROM and SF-36 subscales in older adults. Our pilot study suggests that the DASH survey has potential utility to identify occult shoulder dysfunction in community-dwelling older adults who have normal Katz ADLs and Lawton-Brody IADLs if administered during routine health maintenance primary care visits.
Introduction
Shoulder dysfunction is common and may hasten functional decline in vulnerable older populations. Common associations with shoulder dysfunction include subjective pain or structural pathology such as rotator cuff tear or osteoarthritis. Nearly 20% of adults 65 years and older reported shoulder pain in the 2011 National Heath and Aging Trends Study. 1 One in four older adults in the general population has a rotator cuff tear, with the majority involving the supraspinatus tendon.2,3 The prevalence of glenohumeral osteoarthritis among older adults in the general populations has been estimated to be as high as 17%. 4
Routine screening designed to identify occult shoulder dysfunction in older populations during health maintenance primary care visits is not the standard of care, and the burden of shoulder dysfunction on public health remains poorly understood. Nearly one-half of older adults with shoulder pain do not report their symptoms to healthcare providers during routine primary care visits.5,6 Also, older adults who are not experiencing pain may harbor structural shoulder abnormalities that contribute to functional decline. 7
Novel routine screening programs designed to identify shoulder dysfunction among older adults in primary care settings should be time efficient. Vidt et al recently suggested that the American Shoulder and Elbow Surgeons (ASES) and Simple Shoulder Test (SST) surveys, brief self-reported instruments, have utility for estimating the degree of shoulder dysfunction in populations of community-dwelling older adults who present with clinical symptoms of rotator cuff tear; each of these shoulder-specific surveys has moderate to strong correlation with shoulder range of motion (ROM) and 36-Item Short Form (SF-36) survey subscale scores. 8 However, ASES and SST surveys address unilateral shoulder function only, limiting their utility for efficient routine screening of both shoulders in the primary care setting. By contrast, the self-reported Disabilities of the Arm, Shoulder and Hand (DASH) survey estimates bilateral shoulder function in one composite score, offering potential utility for a routine screening program. The DASH survey is a 30-item tool quantifying symptoms and ability to perform upper extremity activities of daily living (ADLs), with each response rated on a 5-point ordinal scale.9-11 The DASH survey is commonly employed to estimate upper extremity functional performance and recovery following trauma, surgery, or acquired functional disability.12-15 There is no upper age limit for the DASH survey, but there is currently limited evidence to support potential utility for screening populations of community-dwelling older adults during routine health maintenance visits with their primary care provider. McMahon et al showed the DASH survey’s potential utility for screening community-dwelling older adults, in a study of 132 adults ≥ 60 years who were participating in the 2005 Senior Olympics and not seeking medical care for their shoulders, by showing significantly inferior DASH scores among senior athletes who reported shoulder pain as compared those who did not. 16 Similarly, Oh et al, in a population-based study of 679 community-dwelling adults ≥ 65 years designed to estimate the prevalence of shoulder osteoarthritis among older adults in the general population, demonstrated that older adults with shoulder osteoarthritis had significantly inferior functional status by the DASH score as compared to those without shoulder osteoarthritis. 4
The first objective of our pilot study is to determine if the DASH, ASES and SST surveys are related to one another in a population of community-dwelling older adult volunteers. We hypothesize that the DASH survey will have similar utility in estimating the degree of shoulder dysfunction, as compared to the ASES and SST surveys. Our second objective is to determine the relationship of the DASH, ASES and SST survey scores with (1) health-related quality of life via SF-36 subscale scores and (2) physical function via shoulder forward flexion ROM and abduction ROM on physical examination. We hypothesize that the DASH, ASES and SST survey scores will demonstrate a similar relationship to the SF-36 subscale scores, shoulder forward flexion ROM and abduction ROM, in a population of community-dwelling older adult volunteers.
Methods
Study Population
This study was approved by the authors’ institutional review board and complied with the Health Insurance Portability and Accountability Act. All study participants provided written informed consent. From March 2019 to November 2019 a convenience sample of 23 community-dwelling adult volunteers were enrolled at the University of Maryland Baltimore following recruitment by local advertisements (Figure 1). Study participants received shoulder magnetic resonance imaging (MRI); shoulder ROM testing; and completed the DASH, ASES, and SST surveys during a single visit. Inclusion criterion was age between 60 and 85 years. Exclusion criteria were (1) contraindication to MRI, (2) history of prior rotator cuff repair surgery or joint replacement ipsilateral to the shoulder MRI, (3) active worker’s compensation claim, (4) upper extremity paralysis, (5) shoulder injury or shoulder rehabilitation in the prior 3 months. A total of 4 study participants were excluded: 2 study participants did not receive shoulder MRI, and an additional 2 study participants declined to complete the SST survey in its entirety. Therefore, a total of 23 study participants were included in the analysis. STROBE flow diagram.
Clinical Assessment
Study participants completed a medical history questionnaire to record demographics and to determine their (1) Charlson Co-Morbidity Index; (2) Katz ADLs [0, worst; 6, best]; and (3) Lawton-Brody Instrumental Activities of Daily Living (IADLs) [0, worst; 8, best]. The Charlson Co-Morbidity Index included questions screening for history of cardiovascular disease, peripheral vascular disease, cerebrovascular disease, dementia, chronic lung disease, connective tissue disease, peptic ulcer disease, liver disease, diabetes mellitus, hemiplegia, kidney disease, and cancer. The total Charlson Co-Morbidity Index score also assigned one point for every decade over the age of 50 years; therefore the minimum score would be 2, 3, and 4 for participants aged 60-69 years, 70-79 years and 80-85 years, respectively.
All study participants completed the shoulder-specific ASES [0, worst; 100, best] and SST [0, worst; 100 best] surveys. The ASES and SST surveys are specific to estimating functional performance at the shoulder. The ASES survey estimates disability ipsilateral to the shoulder of concern based on 10 questions, specific to shoulder function and each measured by a 4-point level of difficulty ordinal scale, and a single pain question measured by an 11-point ordinal scale.8,9,11 The SST survey estimates ipsilateral shoulder disability based on 12 questions, specific to shoulder function and pain, each measured by 2-point (yes/no) Likert scale.8,11 All study participants completed the DASH survey [0, best; 100, worst]. To provide an estimate of their self-perception of health-related quality of life, study participants completed the SF-36 survey. All self-reported assessments were performed on the same date as shoulder MRI.
A single clinical research specialist performed ROM testing, for the shoulder ipsilateral to the MRI, with a portable hand-held goniometer. Shoulder forward flexion ROM was tested with the ipsilateral hand placed adjacent to the thigh in the starting position. Study participants were asked to raise their upper limb straight out and up in front of them as high as they could reach to record the maximum degree of the shoulder’s forward flexion in one trial. Shoulder abduction ROM was tested with the ipsilateral hand placed next to the thigh in the starting position. Study participants were then asked to abduct their upper limb from their side as high as could be reached to record the maximum degree of the shoulder’s abduction in one trial. All objective clinical assessments were performed on the same date as shoulder MRI. Height and weight were recorded to determine body mass index (BMI).
Shoulder MRI
All shoulder MRI examinations were performed at 3.0 Tesla (Magnetom Prismafit, Siemens HealthCare, Erlangen, Germany). The protocol included 2-dimensional (2D) short tau inversion recovery (STIR) sequences in the oblique coronal, oblique sagittal and axial planes, and a 2D turbo spin echo (TSE) oblique sagittal T1 sequence. Shoulder MRI was performed ipsilateral to the dominant hand, if study participants reported no subjective shoulder complaints. Study participants with subjective shoulder symptoms received MRI ipsilateral to the symptomatic shoulder. A single board-certified musculoskeletal radiologist evaluated each shoulder MRI independently to review the status of the supraspinatus tendon at the rotator cuff. The musculoskeletal radiologist classified the status of the supraspinatus tendon into one of two classes: intact (normal or tendinopathy), or tear (partial-thickness tear or full-thickness tear).
Statistical Analysis
Descriptive statistics were performed as appropriate to characterize the study population, with categorical variables reported as n and continuous variables as mean ± standard deviation. Spearman rank-order correlation (rho) was used to determine (1) the correlation of scores among the DASH, ASES and SST surveys and (2) the correlation of each survey with the subscales of the health-related quality of life SF-36 survey scores, shoulder forward flexion ROM and shoulder abduction ROM. Partial spearman correlations controlling for supraspinatus tendon tear status (tear present or tear absent) also were performed for the DASH, ASES and SST survey scores with the SF-36 survey subscale scores, shoulder forward flexion ROM and shoulder abduction ROM. Correlation was interpreted as .00 to .35, weak; .36 to .67, moderate; and .68 to 1.00, strong. 8 A P value < .05 was considered to indicate significance. Statistical analysis was performed using SAS statistical software version 9.4 (SAS, Cary, North Carolina).
Results
Characteristics of the Study Population (n = 23).
Correlation of Scores Among the Disabilities of the Arm, Shoulder, and Hand (DASH), American Shoulder Elbow Surgeons (ASES), and Simple Shoulder Test (SST) Surveys for the Study Population (n = 23).
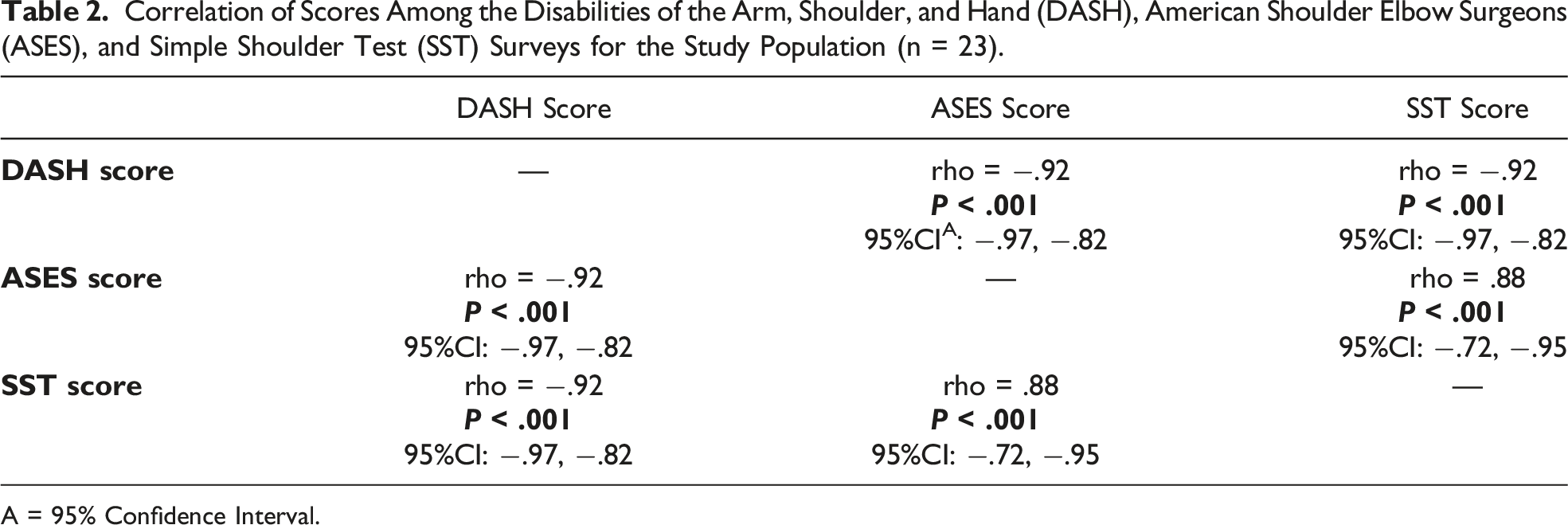
A = 95% Confidence Interval.

Scatterplots showing the relationship of scores among the Disabilities of the Arm, Shoulder, and Hand (DASH), American Shoulder Elbow Surgeons (ASES), and Simple Shoulder Test (SST) surveys for the study population (n = 23).
Correlation of 36-Item Short Form (SF-36) Subscale Scores and Shoulder Range of Motion Performance With the Disabilities of the Arm, Shoulder, and Hand (DASH); American Shoulder and Elbow Surgeons (ASES); and Simple Shoulder Test (SST) Survey Scores for the Study Population (n = 23).

A = 95% Confidence Interval.
DASH score showed statistically significant (P < .05) moderate correlation with role limitations 2° to emotional health (rho = −.67), vitality (rho = −.53), emotional well-being (rho = −.49), and pain (rho = −.51). ASES score showed statistically significant (P < .05) moderate correlation with role limitations 2° to emotional health (rho = .66), vitality (rho = .44), and pain (rho = .42). SST score showed statistically significant (P < .05) moderate correlation with role limitations 2° to emotional health (rho = .60), emotional well-being (rho = .45), and pain (rho = .48).
Partial Correlation of 36-Item Short Form (SF-36) Subscale Scores and Shoulder Range of Motion Performance With Disabilities of the Arm, Shoulder, and Hand (DASH); American Shoulder and Elbow Surgeons (ASES), and Simple Shoulder Test (SST) Survey Scores for the Study Population, Controlling for Supraspinatus Tendon Tear Status (n = 23).

A = 95% Confidence Interval.
Discussion
Our study shows strong correlation among the self-reported DASH, ASES, and SST surveys in a population of community-dwelling older adult volunteers. Our study suggests that the DASH survey is on par with the ASES and SST surveys for identifying shoulder dysfunction in community-dwelling older adults. The DASH survey’s estimation of bilateral upper extremity function in a single composite score provides a feasible tool for a potential routine shoulder screening program in older populations in the primary care setting. The DASH survey shows strong correlation with shoulder forward flexion ROM and abduction ROM, as well as strong or moderate correlation with seven out of nine SF-36 subscale scores, including physical functioning, role limitations 2° to physical health, role limitations 2° to emotional health, vitality, emotional well-being, social functioning, and pain. Overall, our study suggests that the DASH score is similar to, or slightly outperforms the ASES and SST scores, regarding correlation with shoulder ROM and SF-36 subscale scores in community-dwelling older adults.
Shoulder pain is most commonly associated with rotator cuff disease in populations without recent acute injury and has been posited to be a primary determinant of health status in clinical patients.17-21 Vidt et al found that older adults with symptomatic partial-thickness or full-thickness rotator cuff tear showed altered shoulder ROM when performing upper extremity ADLs, as compared to asymptomatic controls. 22 Osteoarthritis, adhesive capsulitis, and rheumatologic disorders are additional common pain sources at the shoulder. 18 The presence of pain, and not the intensity of pain, is theorized to be the most salient factor. Bryant et al reported that pain intensity may have no independent effect on decline in physical performance in older populations. 23
A subset of older populations also exhibit disability in the absence of shoulder pain. Moosmayer et al investigated a cohort of adults with non-painful shoulders, aged 50 to 79 years, and identified a 7.6% prevalence of full-thickness rotator cuff tear. Study participants with full-thickness tear demonstrated a statistically significant deficit in objective shoulder flexion strength on physical examination compared to study participants without full-thickness rotator cuff tear. 7 Burner et al in a study of adults > 60 years reporting for routine primary care visits without shoulder-related chief complaints, demonstrated deficits in shoulder ROM on physical examination in nearly 40% of cases. 5 Similar to Burner et al, our study population of community-dwelling older adult volunteers presented with an average deficit of ≥ 40° for shoulder forward flexion ROM or abduction ROM.
Older populations with no apparent self-reported shoulder symptoms in a variety of circumstances may harbor occult shoulder dysfunction and physical limitations when evaluated.7,24 Even relatively high functioning community-dwelling older adults may harbor potential occult shoulder pathology. For instance, McMahon et al reported a 60% prevalence of rotator cuff tear among older adults ≥ 60 years participating in the 2005 Senior Olympics, not dissimilar to the 50% prevalence of rotator cuff tear in our study sample. 16 Yamamoto et al estimated that nearly 36% of adults older than 60 years in the general population with full-thickness rotator cuff tear have shoulder pain and/or disability. 25
Older adults who do not proactively complain of shoulder symptoms directly to their healthcare providers are unlikely to receive purposeful medical screening to assess for occult shoulder disorders during primary care visits. Burner et al found that less than 50% of older adults at a primary care practice reported their shoulder pain to a healthcare provider. 5 Similarly, Chard et al, in a community survey random sample of 644 community-dwelling adults ≥70 years recruited from the registry of 2 primary care medical practices, reported that < 40% of study participants who self-identified as having shoulder symptoms had actually sought medical evaluation for this specific problem. 6
Katz ADL and Lawton-Brody IADL surveys are traditional tools used to screen for disability in older populations. The community-dwelling older adult volunteers in our study showed near perfect Katz ADL scores and perfect Lawton-Brody IADL scores, consistent with a study population with no traditional definition of disability. Investigators have posited that an ASES score ≥ 90 should be considered “normal” in older adults who do not proactively report shoulder symptoms.7,26-28 In contrast, our study sample had an average ASES score of 81.3. Our study highlights the ceiling effect limitation of the Katz ADL and Lawton-Brody IADL surveys to identify potential shoulder dysfunction.
Chronic shoulder dysfunction also negatively influences their health-related quality of life. Uchida et al, in a study sample of 194 community-dwelling older adults ≥ 65 years with a 25% prevalence of chronic shoulder pain, found that chronic musculoskeletal ailments contribute to poorer self-reported quality of life. 29 Goldberg et al reported that patients presenting to an orthopaedic clinic with symptomatic full-thickness rotator cuff tear and a mean age of 65 years had statistically significant lower SF-36 scores in 5 subcategories, as compared to age- and gender-matched controls. 30 These SF-36 subcategories included physical functioning, role limits 2° to physical health, role limits 2° to emotional health, social functioning and pain. Similarly, Vidt et al showed that older adults with symptomatic partial-thickness or full-thickness rotator cuff tear showed significantly lower scores, as compared to controls, for the physical functioning, role limits 2° to physical health, role limits 2° to emotional health, and pain SF36 subscales. 8 Our study showed strong or moderate correlation between the DASH survey and seven out of nine SF-36 subscales, even when controlling for supraspinatus tendon tear status, which was on par or slightly outperforming the ASES and SST surveys.
The novelty of our study is the concept that the DASH survey has utility to screen for shoulder dysfunction in older populations who present without a chief complaint of shoulder symptoms during routine health maintenance primary care visits. The standard of care for health maintenance visits in primary care generally does not advise screening of patients for shoulder dysfunction, and typically the shoulder is only assessed if the patient presents with a chief complaint of shoulder pain or disability. This is a problem since prior studies report that shoulder dysfunction among older adults is too often under-reported to their healthcare providers.5,6 In a hypothetical routine screening program with the DASH survey, patients could complete the screening tool ahead of time, allowing healthcare providers the opportunity to review the DASH score at the health maintenance primary care appointment, similar to how results from routine laboratory and imaging studies are typically reviewed. When an abnormal DASH score is identified, the healthcare provider would be alerted to perform a targeted history and physical of the shoulder. The decision for potential further management would ideally be decided on a case-by-case basis, after discussion between the patient and healthcare provider. Some patients will need no further intervention, while others may require medication, imaging, referral to physical therapy, and/or consultation with an orthopaedic surgeon.
Limitations include the relatively small sample size of a pilot study, although our sample was still able to identify several statistically significant observations. Our study was cross-section in design. Future longitudinal studies will be necessary to evaluate test-retest reliability. The study sample was a convenience sample, and our results may not be generalizable to the general population. Selection bias was also possible, with participants self-selecting to join the study in order to receive a shoulder MRI at no cost. Study participants displayed low levels of comorbidity, and our study may lack generalizability to older populations with higher levels of comorbidity. Another limitation was the fact that we did not perform range of motion testing or shoulder MRI for the contralateral shoulder, with only one shoulder received objective testing. The DASH survey also is not specific to the shoulders, but instead is designed to evaluate function of the entirety of both upper limbs. However, discovery of an unexpectedly abnormal DASH score would still be beneficial to older adult populations, since recognition of any previously undiagnosed upper-extremity disability is also in patients’ best interest. Future larger studies will be necessary to determine cut-offs for DASH score which would inform healthcare providers when additional proactive shoulder evaluations are appropriate. Future studies also will be needed to estimate what percentage of older adults, with an abnormal DASH score discovered during routine health maintenance primary care visits, would choose further clinical evaluation vs those who would decline any further work up.
Conclusion
The DASH, ASES and SST scores correlate strongly with one another. The traditional approach to quantification of disability in older populations, the Katz ADLs and Lawton-Brody IADLs surveys, were limited by a ceiling effect and failed to identify symptoms of shoulder dysfunction in our study sample of community-dwelling older adult volunteers. The DASH survey showed strong correlation with shoulder forward flexion ROM and abduction ROM, and also strong or moderate correlation with seven out of nine subscales of the SF-36 survey. Our pilot study suggests that the DASH survey has utility as a screening instrument to identify occult shoulder dysfunction in older populations. Future larger studies that evaluate the utility and feasibility of the DASH survey for routine screening in the population of older adults who receive routine health maintenance from primary care providers is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Aging [3P30AG028747]; and the University of Maryland Claude D. Pepper Center Older Americans Independence Center [3P30AG028747].
Authors’ Note
Please be aware that the data was presented as a poster presentation during the 10th International Conference on Frailty & Sarcopenia Research: Davis DL, Almardawi R, Gullapalli R, Terrin ML. Identification of Community-Dwelling Older Adults with Shoulder Dysfunction: Evaluation of the DASH survey (digital poster) 10th International Conference on Frailty & Sarcopenia Research, Toulouse, France, March 11-13, 2020.