
Abstract
Background
In elderly tibial plateau fractures (TPFs), the lateral condyles are involved frequently. This study aimed to compare the outcomes of open reduction and internal fixation (ORIF) and double reverse traction repositor (DRTR) assisted closed reduction and internal fixation (CRIF) in elderly patients with lateral TPFs.
Methods
From January 2015 to July 2020, we retrospectively reviewed 68 patients treated surgically at our trauma center for lateral TPFs (Schatzker type I-III). 31 patients were eventually assigned to the DRTR assisted CRIF group, whereas 37 patients were assigned to the ORIF group. The primary outcomes included surgical details, radiological assessment, follow-up knee function, and complications.
Results
The DRTR assisted CRIF group experienced a 43.6 mL decrease in intraoperative blood loss (161.3 mL vs 204.9 mL, P = .033), and the operation duration was 32.1 min shorter than the ORIF group (83.8min vs 115.9min, P < .001). No statistical difference was found between the two groups in terms of transfusion rate (3.2% vs 8.1%, p = .394), and postoperative hemoglobin level was lower in the ORIF group than in the DRTR assisted CRIF group (111.8±13.3 g/L vs 104.5±12.7 g/L, p = .025). There was no statistically significant difference in terms of widening of the tibia plateau (WTP), depth of articular depression (DAD), medial proximal tibial angle (MPTA) and posterior tibial slope angle (PTSA) preoperatively, immediately after surgery and at the last follow-up. No differences in malreduction (P=.566) or reduction loss (P =.623) were observed between the groups, and Lysholm and HSS scores were similar between the two groups (83.6 ± 15.8 vs 83.4 ± 5.1, P = .934; 89.3 ± 7.8 vs 86.9 ± 6.2, P = .172; respectively). However, ORIF was associated with a greater increase in postoperative complications than DRTR assisted CRIF (3.2% vs 27%, P = .008).
Conclusion
Both types of internal fixation provide good radiological outcomes and knee function in the treatment of lateral TPFs in the elderly. However, DRTR assisted CRIF has the advantage of a shorter duration of surgery, less blood loss, and fewer postoperative complications, and appears to be a better treatment option for elderly patients with lateral TPFs.
Keywords
Introduction
Tibial plateau fractures (TPFs) are not rare among the elderly, accounting for about 8% of all geriatric fractures. 1 These injuries are becoming more common in the elderly as life expectancy increases. In contrast to younger patients, who frequently sustain fractures as a consequence of high-energy injuries, elderly patients frequently sustain TPFs as a result of low-energy injuries. 2 Elderly TPFs exhibit varied degrees of articular depression and displacement, as well as a variety of fracture patterns, and are caused by an overloaded tibial plateau combined with compression and varus or valgus. 3 The lateral condyles are the most involved. 4 There are several treatment options for fractures in the elderly, and the ideal treatment is not always univocal, depending on a range of factors such as fracture type, bone quality, surgeon preference, and experience. 5
Despite the increased interest in primary total knee arthroplasty (TKA) for TPFs in the elderly, poor soft tissue envelope and multi-plane malalignment make TKA more difficult in elderly patients, 6 and some studies have shown that TKA performed following a TPF has a higher rate of complications than TKA performed for primary osteoarthritis. 7 Additionally, recent studies indicate that older patients will still have good, if not better outcomes than young patients following open reduction and internal fixation (ORIF) of TPFs, and ORIF remains an effective treatment option for elderly patients.8,9 The DRTR-assisted CRIF has been successfully used to treat a variety of lower limb fractures and has been shown to have the advantages of minimal trauma, consistent joint anatomical restoration, and a low complication rate for treating TPFs.10-12 Despite these advantages of DRTR, no direct comparison of surgical outcomes for elderly TPFs between ORIF and DRTR-assisted CRIF has been performed.
The objective of this study was to assess the outcomes of elderly patients who had lateral TPFs treated with ORIF or DRTR-assisted CRIF.
Methods
Study Design and Patients
The purpose of this retrospective case-control study was to compare the outcomes of ORIF and DRTR-assisted CRIF in the treatment of elderly patients with lateral TPFs. This study was approved by our institutional ethics committee and conducted in accordance with the Helsinki Declaration. All patients signed informed consent. Between January 2015 to July 2020, we retrospectively enrolled 68 patients with TPFs at a Level I Trauma Center. The following criteria were met by all of the patients in this study: Patients were (i) aged > 60 years, (ii) diagnosed with unilateral closed lateral TPFs, and (iii) followed-up for at least 12 months. The exclusion criteria were as follows: (i) associated neurovascular injury, (ii) polytrauma, (iii) Schatzker IV-VI, (iv) open and/or pathologic fractures, (v) pre-existing limited range of motion of the knee, and (vi) incomplete patient data. Patients were divided into two groups based on their choice of treatment. Patients treated with DRTR-assisted CRIF were included in group 1, while those treated with ORIF were included in group 2 (Figure 1). Flowchart showing screening of patients (patients may be excluded for a variety of reasons).
Surgical Treatment and Post-operative Care
Double reverse traction repositor is a traction reduction device originally developed in our center, and the surgical procedure that it facilitates for the treatment of TPFs has been extensively reported in previous literature.
13
The two opposing traction forces generated by DRTR, along with the squeezing and repositioning action of the soft tissues surrounding the knee joint, serve to reduce and maintain the displaced fracture fragment. In the case of an articular surface depression, the depressed fracture was reduced and elevated using a customized bone tamp inserted via the tunnel formed by step drilling. Meanwhile, autogenous iliac bone was obtained and inserted into the bone tunnel to provide support for the repaired joint surface. Finally, minimally invasive percutaneous plate osteotomy (MIPPO) was performed on the lateral cortex using a locking compression plate (LCP). (Figure 2). In group 2, patients received a traditional anterolateral approach to the proximal tibia with submeniscal arthrotomy for lateral injuries. Case of a 66-year-old male Schatzker II patient treated with DRTR assisted closed reduction and internal fixation. (a) The general preoperative view of the DRTR. (b-c) Percutaneous reduction of the compressed fracture with a customized bone tamp (AP and lateral views). (d-e) Intraoperative fluoroscopic view showing satisfactory position of internal fixation (AP and lateral views). (f-g) Immediate postoperative radiographs (AP and lateral views). DRTR = double reverse traction repositor. AP Use the “Annotate” button to place an annotation on (a section of) the figure.
In all patients, a single shot of antibiotic was given preoperatively and continued for 24 hours postoperatively. Thromboprophylaxis was by use of low-molecular-weight heparin. Non-weight-bearing joint activities were started on the second postopera-tive day, and weight-bearing exercises were not allowed until the 8 weeks after surgery.
Data Collection
We collected and compared demographic data, the energy of trauma, mechanism of injury, type of fracture, surgical data, radiological parameters, functional outcomes, and postoperative complications between the two groups. Preoperative and postoperative imaging data were assessed by two independent radiologists with expertise in orthopedic trauma, each with over 5 years of experience and blinded to additional patient information. In cases of disagreement, another senior radiologist was consulted. The Schatzker classification system, 14 classified lateral TPFs as types I, II, and III.
The depth of articular depression (DAD), widening of the tibia plateau (WTP), posterior tibial slope angle (PTSA), and medial proximal tibial angle (MPTA) were all assessed using standard anteroposterior and lateral radiographs preoperatively, immediately after surgery and at final follow-up. The quality of reduction was considered satisfactory if the DAD was ≤2 mm, the WTP was ≤5 mm, the PTSA was 9° ± 5°, and the MPTA was 87° ± 5°, otherwise it was malreduction. Reduction loss was defined as DAD > 3 mm, WTP > 5 mm, and a coronal malalignment greater than 5° towards varus or valgus at the last follow-up compared to the immediate postoperative radiographs. The functional outcome was evaluated using the Lysholm score and Hospital for Special Surgery (HSS) score at the final follow-up.
Statistical Analysis
Data analysis was performed by an independent statistician using SPSS (Version 26.0; IBM Corp, USA). For categorical data, descriptive statistics were calculated using frequency distributions, while for continuous data, means, standard deviations, and ranges were used. For continuous data, the Student’s t-test and one-way analysis of variance were used; for categorical data, the Chi-square test was used. A P-value < .05 was considered statistically significant.
Results
Demographic Characteristics.
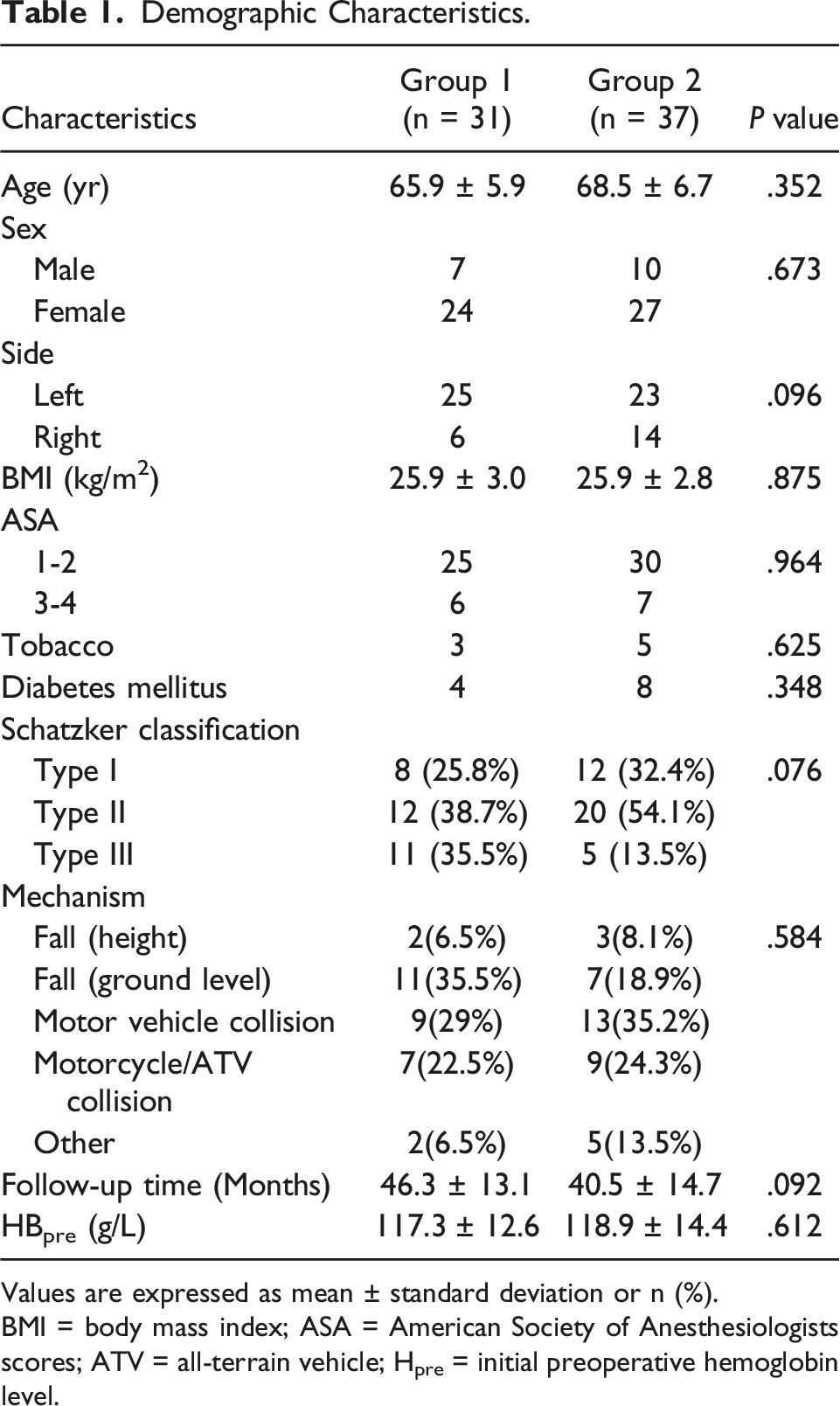
Values are expressed as mean ± standard deviation or n (%).
BMI = body mass index; ASA = American Society of Anesthesiologists scores; ATV = all-terrain vehicle; Hpre = initial preoperative hemoglobin level.
Clinical Results of Two Groups.

Values are expressed as mean ± standard deviation or n (%).
HBpost-1 = hemoglobin level of first postoperative day, DVT = deep vein thrombosis, HSS = Hospital for Special Surgery.
Results of Radiological Assessment.

Values are expressed as mean ± standard deviation or n (%).
WTA = Widening of the tibia plateau, DAD = Depth of articular depression, MPTA = Medial proximal tibial angle, PTSA = Posterior tibial slope angle.
Discussion
To the best of our knowledge, this is the first study that compares ORIF and DRTR-assisted CRIF for lateral TPFs in the elderly. The study’s most significant finding was that radiological outcomes and knee function were comparable in elderly patients treated with ORIF and DRTR-assisted CRIF. However, the DRTR-assisted CRIF had the advantages of a shorter operating time, less intraoperative blood loss, and fewer associated complications.
Indeed, DRTR-assisted CRIF has been widely used to successfully treat lower extremity fractures.10,11,15 Unfortunately, none of the previous reports specifically focused on elderly patients with TPFs. Despite recent advancements in surgical procedures and fixation techniques that allow for accurate reduction and stabilization of fractures, treating TPFs in the elderly continues to be a problem for orthopedic surgeons. There are two main difficulties: 1) the difficulty in achieving secure fixation to accomplish early knee motion and 2) the high risk of complications following internal fixation due to the fragile and friable skin and soft tissue envelope. 16 Additionally, elderly patients have poor bone quality and are more likely to experience increased bone loss following TPFs. 17 However, Kim JK et al 9 recently concluded that age ≥60 years was not an independent risk factor of poor radiographic outcomes following ORIF for TPFs and that ORIF remained an effective treatment option for elderly patients.
Our results showed no statistical differences in preoperative WTA, DAD, MPTA and PTSA between the two groups and that DRTR-assisted CRIF was similar to ORIF in terms of both the rate of malreduction in the immediate postoperative period and the loss of reduction at the final follow-up. A well-positioned intraoperative bone graft can directly replace lost subchondral bone, allowing the fixation device to be implanted in a region of sufficient bone quality to avoid malreduction or reduction loss.18,19 The DRTR-assisted CRIF group received bone grafting through a tunnel produced by step drills, whereas the ORIF group had bone grafting under direct view, both of which effectively fill the bone defect and maintain the restored joint level. There was no significant difference in the rate of bone grafting between the two groups. In addition, the ORIF group provided effective fracture reduction under direct view, while the DRTR-assisted technique allowed equally effective closure reduction of fracture displacement and malalignment through skeletal traction and soft tissue compression. 12 Both types of internal fixation provided comparable radiological outcomes.
The goal of surgical treatment of TPFs, in addition to restoring the plateau congruity and re-establishing mechanical alignment of the limb, should allow patients to return to full knee function sooner. 2 A recent study found no difference in knee function scores between patients with lateral TPFs treated with ORIF or CRIF. 13 Similarly, Wang, Z et al 20 demonstrated that both CRIF and ORIF were effective in treating Schatzker I–IV TPFs. The present study found no statistically significant difference in knee function between the ORIF and DRTR-assisted CRIF groups with similar Lysholm and HSS scores, which was consistent with previous studies. However, Wang, Y. et al 21 reported that arthroscopically assisted CRIF had a superior functional outcome to ORIF in treating low-energy tibia plateau fractures. We hypothesize that the discrepancy can be explained by the fact that their study subjects were younger and more active that may have higher functional demands, and arthroscopically assisted CRIF can treat TPFs along with concomitant meniscal or ligament injuries, improving postoperative functional outcomes. In comparison, the osteoporotic bone tissue in elderly patients absorbs the majority of the mechanical energy from the trauma, resulting in significantly less meniscal or ligament damage, 22 and therefore, it is likely that the effect of meniscal or ligament-related differences on postoperative function may be smaller. Moreover, consequent decline in knee function may be less restrictive due to lower functional demands of the elderly. Overall, we concluded that ORIF and DRTR-assisted CRIF can yield comparable functional knee outcomes in the treatment of TPFs in the elderly.
In addition to decreased bone quality, elderly patients have fragile and friable skin and soft tissue envelopes and often suffer from chronic diseases. In this study, patients who underwent CRIF had less intraoperative blood loss and shorter operative times, which might improve the safety of the procedure in elderly patients with special physical characteristics. DRTR allowed the lower extremity to be kept in traction from the beginning to the end of the surgery, effectively reducing the fracture displacement through skeletal traction and other soft tissue (muscles, ligaments, etc.) compression, which makes the surgery easier, shorter and less blood loss. Similarly, Chang et al, in a study of 21 bicondylar TPFs treated with a DRTR, also found shorter operative times and less blood loss with traction repositioning compared to arthrotomy. 12 In addition, Deng et al 23 reported less intraoperative blood loss in CRIF, which was consistent with our findings, but also found no statistical difference in operative time between CRIF and ORIF. This may be due to the fact that their operative time included arthroscopy, whereas the operative time in our and Chang et a l.’s study did not include the time of arthroscopic examination. Both shorter operative times and less intraoperative blood loss are critical for elderly patients, allowing for a safer and more reliable procedure. In this regard, we considered CRIF to be superior to ORIF in the treatment of TPF in the elderly.
Additionally, we compared the groups in terms of complication rate, which is often cited by orthopedists to support the use of ORIF vs CRIF. Overall, we found a 16.2% complication rate: 10 complications in 37 patients in the ORIF group and one complication in 31 patients in the CRIF group. Fewer post-operative complications were significantly observed in the DRTR-assisted CRIF group than in the conventional ORIF group. Similarly, a recent study comparing ORIF with CRIF for the treatment of lateral TPFs found four complications in a total of 40 patients, with all of them occurring in the ORIF group. 24 In a meta-analysis including 10 trials, 21 postoperative complications totaled 36 in ORIF and 12 in CRIF, with surgical site infection being the most common complication, and the risk of postoperative complications was statistically significantly lower in the CRIF group than in the ORIF group, consistent with our results. The conventional ORIF treatment requires excessive soft tissue dissection, which may increase the risk of neurovascular injury, postoperative infection, thrombosis, and other complications,25-27 while DRTR-assisted CRIF for TPFs avoids extensive incision and large soft tissue dissection. Especially in elderly patients with poor bone quality, the absence of massive soft tissue dissection will minimize potential soft tissue complications.28,29 Additionally, less disturbance expedited fracture healing and allowed early mobilization which enabling the reduction of postoperative complications. 30 This study revealed that the operative time of ORIF was significantly longer than that of DRTR-assisted CRIF, and the longer the operation, the greater the possibility of knee infection. 31 As they age, increasing complications may affect their postoperative well-being and satisfaction. Therefore, DRTR-assisted CRIF with a low complication rate appears to be a more suitable option for treating TPFs in elderly patients.
To the best of our knowledge, this is the first study comparing the outcomes of ORIF and DRTR assisted CRIF in elderly patients with TPFs. Moreover, this study has a high follow-up rate. Despite these strengths, several limitations exist. The first limitation is the retrospective design of the study. Second, the number of patients included in the study was relatively small. Third, the follow-up period was short, which may have compromised the ability to draw accurate conclusions regarding the development of late complications, particularly post-traumatic osteoarthritis and the need for TKA. In addition, the imaging measurement was performed using radiographs, which have limited sensitivity and specificity. Finally, as blood routine examination is routinely performed at our trauma center on the first postoperative day, only hemoglobin level of first postoperative day was measured, and more data on postoperative hemoglobin levels are not available. Further prospective studies are warranted to validate our findings.
Conclusion
When treating elderly patients with lateral TPFs, DRTR-assisted CRIF is as effective as ORIF in terms of radiological outcomes and knee function and has the advantages of requiring shorter operative time, less blood loss, and has fewer postoperative complications. DRTR-assisted CRIF is a minimally invasive procedure, that would be a good treatment option for elderly patients with lateral TPFs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Education of Hebei Province (CXZZBS2021083).