
Abstract
Background
Hip fracture in elderly patients is associated with a significant mortality which may be worsened by COVID-19 infection.
Objective
To undertake a systematic review and meta-analysis of studies assessing the effect of COVID-19 infection and mortality rates in hip fracture patients in the United Kingdom (UK) during the first surge of the pandemic.
Design
A systematic literature search of 9 online databases was undertaken independently by 2 reviewers using the Cochrane methodology for systematic reviews. Eligibility criteria were any study of an adult population with a hip fracture that assessed the relationship between COVID-19 infection and 30-day mortality in the UK. Meta-analysis was conducted using a random-effects model.
Results
Out of 309 identified articles, 10 studies reporting on 2448 hip fracture patients met the inclusion criteria. Meta-analysis showed that the estimated mortality rate in patients with laboratory confirmed COVID-19 infection was 32.5% (95% CI= 28.3 to 37.0) compared to 8.6% (95% CI= 6.3 to 11.6) in COVID-19 negative patients. Meta-analysis of 9 comparative studies showed a significantly higher mortality in patients with laboratory confirmed COVID-19 infection as compared to patients without (RR=3.937, 95% CI= 2.867 to 5.406, P<.001). Similar findings were obtained when comparing mortality in COVID-19 laboratory confirmed or clinically suspected infected vs non-infected patients (RR=4.576, 95% CI = 3.589 to 5.835, P <.001).
Conclusions
COVID-19 infection is associated with a 4-fold increase in mortality risk in hip fracture patients. Every effort should be made to avoid COVID-19 infection and nosocomial exposure in this highly vulnerable patient group.
Introduction
Infection with COVID-19 is associated with high mortality rates, especially in elderly male patients with comorbidities such as diabetes, hypertension, cardiovascular and respiratory disease. 1 Similarly, in the pre-COVID-19 era, a higher mortality in hip fracture patients has been associated with older age, male gender, dementia, cardiovascular disease, renal disease and malignancy. 2
In the UK, in recent years, there have been substantial improvements in hip fracture care and reduced mortality rates with the implementation of early orthogeriatric input, early surgery and prompt post-operative mobilisation. The National Hip Fracture Database (NHFD) collects data from 175 trauma units in England, Wales and Northern Ireland and since its inception in 2007 has demonstrated a steady decline in hip fracture mortality, with a 30-day mortality of 6.1-6.9% during 2016-2018. 3 Similarly, in Scotland, the Scottish Hip Fracture Audit (SHFA) reported a 7.7% 30-day mortality in 2019. 4
The NHFD and SHFA has largely standardised care, enabling a more uniform assessment of the effect of COVID-19 on mortality. We have undertaken a systematic review and meta-analysis to assess the early mortality rate of hip fracture patients in the UK, with and without COVID-19 infection.
Methods
A systematic literature search was performed following the Cochrane methodology for systematic reviews on 19th October 2020. The following bibliographic databases and COVID-19 resource sites were searched with no publication or language limit: Pubmed, EMBASE, CINAHL, CENTRAL (Cochrane Library), COVID-19 research database WHO, Lancet COVID-19 research centre, JAMA network, NEJM, COVID-19 Open Research Dataset Challenge. The November 2020 issues of the Bone and Joint Journals and Journal of Bone and Joint Surgery (Am) were also searched. The reference lists of included studies were examined for any additional studies. The search in all databases was performed with a combination of key-words “covid” and “fracture”.
Inclusion Criteria
• Study design: Any study design • Population: Patients with a hip fracture • Comparators: COVID-19 infection (based on testing or clinical suspicion) vs no infection • Outcomes: Studies reporting on “30-day” mortality
Exclusion Criteria
• Case reports, reviews, editorials, commentaries, personal opinions, surveys and case series reporting on a total of less than 10 patients.
Based on the above eligibility criteria, 2 reviewers independently screened the titles and abstracts of all identified studies. Duplicates were removed. The full texts of studies considered eligible were independently reviewed by the 2 reviewers. Any disagreements were discussed between the 2 reviewers and with a senior author.
Data Extraction
Two reviewers independently extracted relevant data (demographics and outcomes) from the included studies. Any disagreements in the eligibility assessment or data extraction were discussed between the 2 reviewers and with a senior author if differences were still unresolved. Where further clarification of data was needed, the authors of the included studies were contacted.
The design methodology of each study was determined using the guidelines described by Mathes and Pieper. 5
Assessment of Methodological Quality of Studies
The methodological quality of the included studies was assessed using the Methodological Index for Non-Randomised Studies (MINORS criteria). 6
Statistical Analysis
An initial descriptive analysis of the studies was performed, presenting study characteristics, populations and outcomes.
Meta-analysis was conducted using a random-effects model, due to the inherent heterogeneity encountered in clinical studies. Mortality rates, Risk Ratios (RRs) and 95% confidence intervals (CIs) were calculated and reported. Heterogeneity was assessed using tau2, I2, Q and P values. Funnel plots were plotted for the studies comparing mortality rates between groups with and without COVID-19 infection, and visual assessment of these funnel plots was undertaken to look for asymmetry. No formal testing for funnel plot asymmetry was performed due to the small number of studies analysed. Data were analysed with Comprehensive Meta-analysis version 2 (Biostat, Englewood, NJ, USA).
Results
The search returned 309 articles, of which 28 were duplicates and 244 failed to meet the inclusion criteria and were excluded. Full-text review of the remaining 37 articles resulted in further exclusions. Ten studies including 2448 hip fracture patients met the inclusion criteria (Figure 1).7-16 Flow diagram for meta-analysis.
Demographic and treatment data.

NP= information not provided.
Fracture type and surgical management in included studies.

N/A= Not applicable NP= information not provided.
Definitions of 30-day mortality and of clinical suspicion of COVID-19 status.
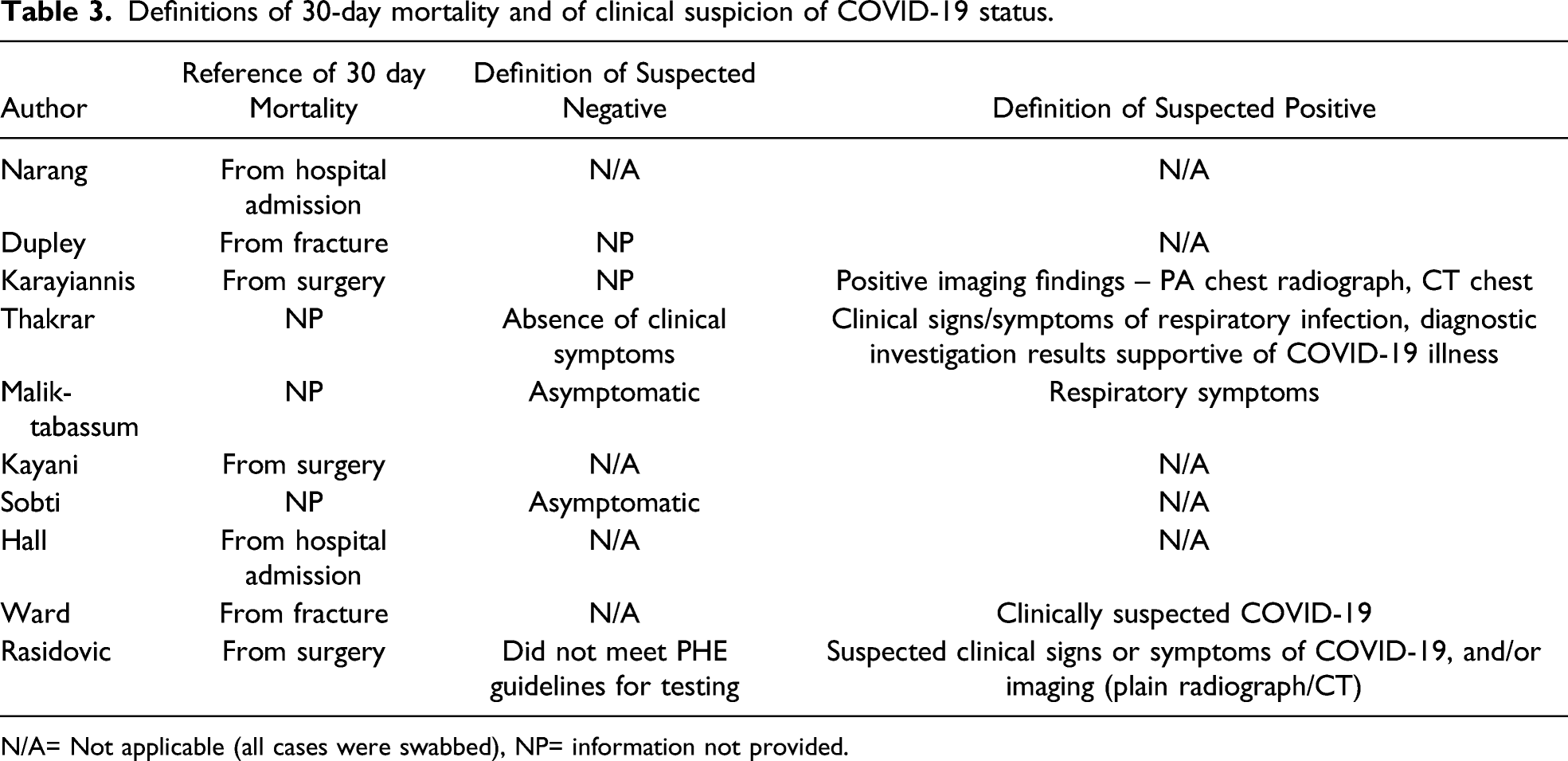
N/A= Not applicable (all cases were swabbed), NP= information not provided.

Location of the hip fracture hospitals described in the included studies. (larger markers represent the hospital of the lead author and the smaller markers represent other units included in each multicentre study).
Summary of mortality rates in included studies.
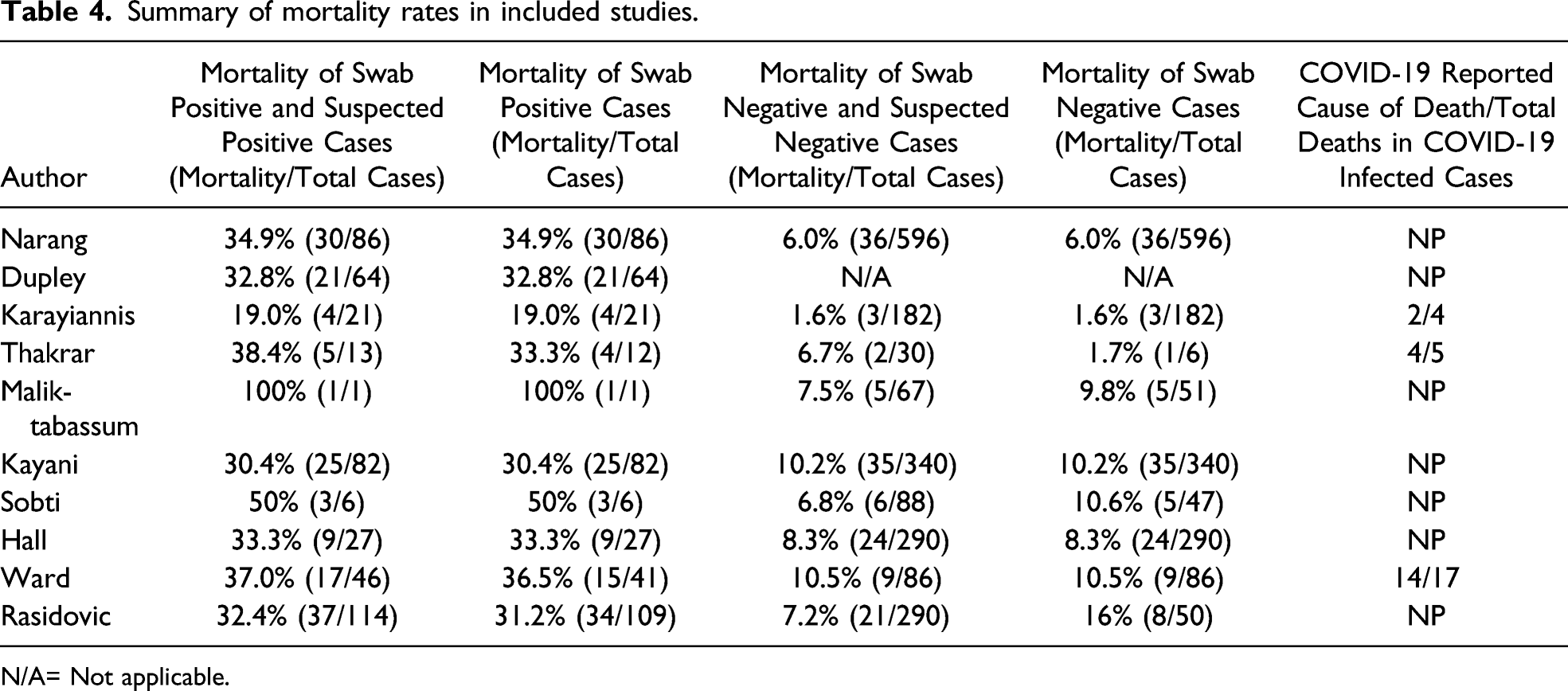
N/A= Not applicable.
Mortality
Meta-analysis showed that the estimated overall mortality rate in patients with COVID-19 infection (laboratory confirmed with a positive oropharyngeal or nasopharyngeal swab test with real-time reverse transcription polymerase chain reaction (RT-PCR)) was 32.5% (95% CI= 28.3 to 37.0, heterogeneity tau2=.00, I2=.00, Q=3.25, P=.92) and was higher than the estimated mortality rate in patients without COVID-19 infection with a mortality rate of 8.6% (95% CI= 6.3 to 11.6, heterogeneity tau2=.13, I2=58.71, Q=19.38, P=.01). Mortality rates were similar when COVID-19 diagnosis was based on laboratory testing or clinical suspicion - 33.1%, (95% CI= 28.9 to 37.5, heterogeneity tau2=.00, I2=.00, Q=3.41, P=.91) vs 7.4% (95% CI= 5.8 to 9.4, heterogeneity tau2=.06, I2=44.27, Q=14.35, P=.07).
Meta-analysis of the 9 studies that directly compared mortality rates showed that COVID-19 infection (based on laboratory RT-PCR testing) was associated with a higher mortality risk compared with no infection, with an estimated RR of 3.937 (95% CI= 2.867 to 5.406, P<.001, heterogeneity tau2=.08, I2=35.61, Q=12.42, P=.13). This was similar when COVID-19 diagnosis was based on laboratory testing or clinical suspicion (RR=4.576, 95% CI = 3.589 to 5.835, P <.001, heterogeneity tau2=.02, I2=13.08, Q=9.20, P=.33). (Figures 3 and 4) Meta-analysis of studies comparing laboratory confirmed COVID-19 infected vs non-infected patients. Meta-analysis of studies comparing laboratory confirmed or clinically suspected COVID-19 infected vs non-infected patients.

Funnel plot analysis did not show a small study effect for the studies comparing laboratory confirmed cases but suggested a small study effect for studies that combined laboratory testing and clinical suspicion.
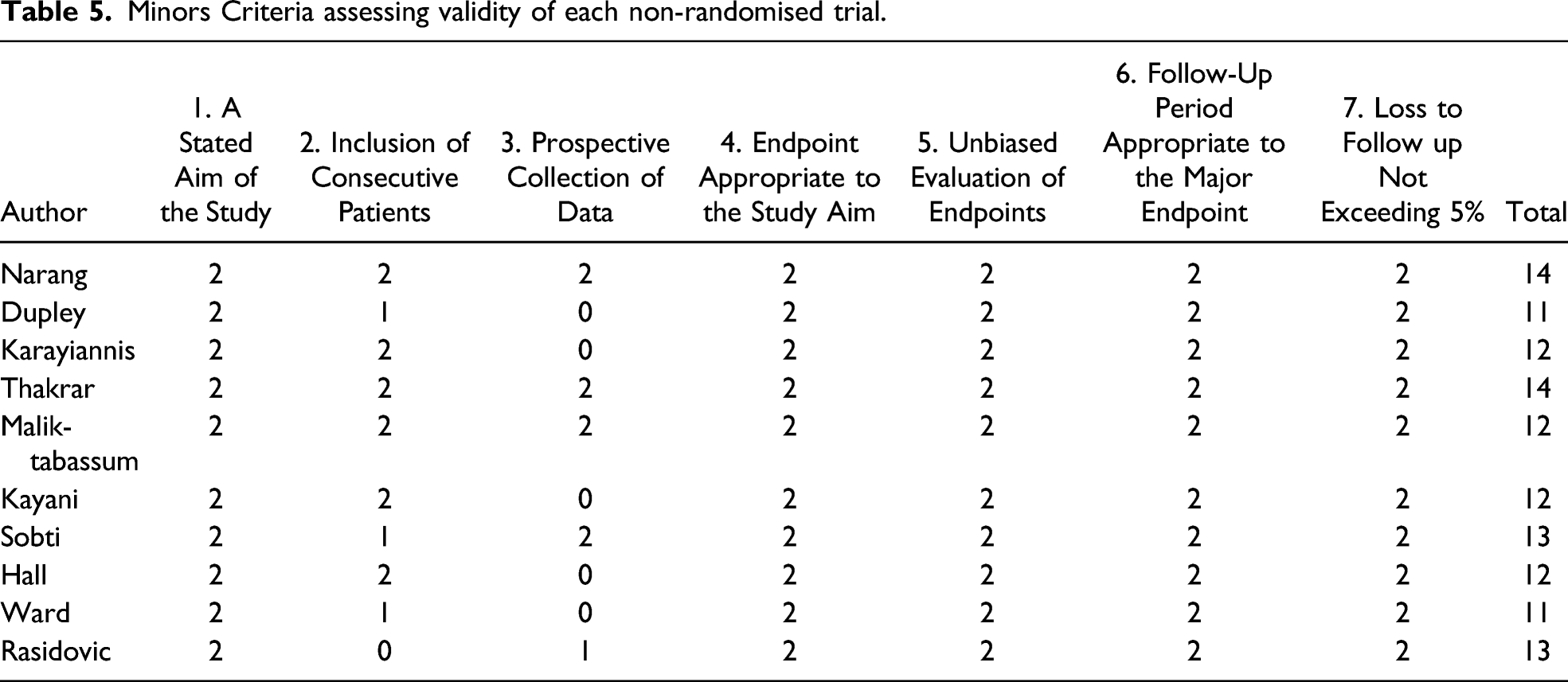
Assessment of Methodological Quality of Included Studies
Minors Criteria assessing validity of each non-randomised trial.
Discussion
We show that the first surge of the pandemic COVID-19 infection was associated with a high mortality rate of about 33%, and an estimated 4-fold increase in 30-day mortality risk in hip fracture patients in the UK.
It was reassuring that the early mortality rate in non-COVID-19 hip fracture patients in our meta-analysis was estimated at 8.6% which is only marginally higher compared to the 30-day mortality of 6.1% in the NHFD and 7.7% in the SHFA reported in 2019.3,4 This may suggest that although systemic changes in the provision of care could be related to the observed increased mortality, COVID-19 infection per se was the major contributor.
In the UK, the overall mortality rate of patients with a confirmed labarotory test for COVID-19 is reported as .8%. 17 The mortality of patients admitted to hospital with symptomatic COVID-19 infection during the first surge of the pandemic in the UK was about 33%. 18 Whilst, the hip fracture patients included in this study were admitted to hospital due to their fracture, and COVID-19 may have been an incidental finding, they had a similar mortality rate. This would suggest that hip fracture patients are a highly vulnerable group with regards to the effects of COVID-19 infection in the perioperative period.
Our reported relative risk is lower than the results of a recent international meta-analysis which reported a 7-fold increase in mortality risk in patients with hip fracture and COVID-19 as compared to non-infected patients. However, the authors of that study, did not define the duration of follow up with regards to mortality, and only included 4 studies in their analysis with just 1 study from the UK. 19
Delays to surgery has been linked to increased mortality in hip fracture patients,20,21 hence timing to surgery for hip fracture is a main performance indictor for NHS services in the UK. The NHFD gather data on the timing of surgery from first presentation with a hip fracture to hospital. In the NHFD 69% of patients in 2018 had surgery on the same day or on the day following injury. 3 The average wait for surgery was 33.1 hours in 2017 and 2018. Similarly, in 2019, in the SHFA, 72% of hip fracture patients had surgery within 36 hours of admission. 4 In our meta-analysis, time to surgery was available for 5 studies, which seemed similar to that achieved in the pre-COVID-19 hip fracture databases.
Several possible reasons may explain the increased mortality observed in our meta-analysis, including the enhanced coagulopathy in COVID-19, 22 combined with reduced mobility associated with hip fractures which may increase the risk of venous thromboembolism and disseminated intravascular coagulation. Anticoagulation in patients with more severe COVID-19 infection has been associated with reduced mortality. 23 The hip fracture and associated surgery per-se may also induce the release of inflammatory cytokines which may potentiate COVID-19 induced inflammation 24 leading to cytokine storm, acute respiratory distress syndrome and multi-organ failure. 25 Of course several factors including older age, obesity, diabetes and cardiovascular disease commonly coexist in patients with hip fracture and are associated with increased mortality of COVID-19.26,27 In line with this, Mi et al looked at 10 patients with a fracture and symptomatic COVID-19 in the Hubei province in China. They reported lymphopenia (<1.0 × 109 cells/L) in 6 of 10 cases, and high D-dimer and C-reactive protein levels in 9. Four of their patients died within 2 weeks of admission. They concluded that the clinical characteristics and early prognosis of COVID-19 in patients with a fracture tended to be more severe than those reported for patients with COVID-19 without fracture and that surgical treatment should be carried out cautiously or non-surgical care should be chosen for such patients. 28
Given the markedly increased mortality in patients with COVID-19 and hip fracture, every effort should be made to avoid nosocomial COVID-19 infection. Ward et al reported that only 19.6% of their COVID-19 infected hip fracture patients had symptoms on admission and the timing of diagnosis for most of their patients (60.8%) suggested nosocomial infection. 14 Kayani et al 12 reported that about 50% of their COVID-19 cases had a negative swab on admission, suggesting a subsequent nosocomial infection. Heneghan et al 29 estimated at around 17.6% of COVID-19 hospitalised cases in England fit the definition as being hospital acquired. In a recent study we have shown substantial deficiencies in the measures adopted to limit nosocomial COVID-19 infection in hip fracture patients in hospitals in the North West of England. 30 Public Health England (PHE) published guidelines for hospital care with high, medium and low COVID-19 risk pathways. 31 Acute hip fracture patients would qualify as high risk patients and therefore should be nursed in a single room or specific area until their laboratory test results is known.
The proportion of COVID-19 cases reported in the included studies varied substantially. Karayiannis et al showed that 10.4% of their hip fracture patients were COVID-19 positive, 9 whereas in the study by Kayani 12 at the proportion was almost double at 19.4%. This may be due to different rates of community prevalence in the country regions examined, or due to different rates of nosocomial infection. Hall et al compared patients who were COVID-19 infected on admission vs those who became infected post-surgery and did not find any difference in mortality, suggesting that both groups are similarly exposed to the detrimental effects of COVID-19 infection. 14
This meta-analysis has certain limitations, including the retrospective nature of some of the studies and their heterogeneity with regards to the reference time point of the 30-day mortality and definition of the COVID-19 status. Similarly, time to surgery was not clearly defined in our included studies. The limited information in the publications did not allow us to identify subgroups of hip fracture patients with more severe COVID-19 infection or determine the cause of death in patients with COVID-19. Nevertheless, despite these limitations we feel that our findings, through the meta-analysis of multiple studies carried out in the UK, where hip fracture care is highly standardised, are robust enough to guide management of this fracture group.
In conclusion, COVID-19 infection in hip fracture patients in the UK is associated with a 4-fold increase in mortality risk. Every effort should be made to minimise infection with COVID-19 in this highly vulnerable group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.