
Abstract
Background
SARS-CoV-2 (COVID-19) has resulted in a widespread loss of lives, morbidity, and major disruptions to the healthcare system. Hip fractures are an emergent condition which require early intervention to reduce increased risk of mortality and morbidity. Infection of SARS-CoV-2 may contribute to increased mortality due to the role of infection and immune response. This study investigated the impact of COVID-19 infection (defined by clinical symptoms) on mortality following proximal femoral fracture (PFF) repair procedures.
Methods
This study was a retrospective cohort study. Data from the Premier Healthcare Database® was extracted for patients presenting for PFF during 2019 for control, and February 2020-September 2020 to represent a COVID time-period.
Results
A total of N = 73 953 subjects were enrolled for the 2019 period, and a total of N = 34 842 subjects were enrolled for the COVID period. For the 2019 period, subjects who had a PFF procedure and who had flu/COVID-like illness had 2.47 (CI:2.11, 2.88) times the odds of mortality compared to those who did not have flu/COVID-like illness. Subjects who had a PFF procedure and who had flu/COVID-like illness during the COVID period had 2.85 times (CI:2.36, 3.42) the odds of mortality compared to those who did not have flu/COVID-like illness. For the COVID period, within subjects who did not have a PFF procedure, those with flu/COVID-like illness had increased odds of mortality compared to those who did not have flu/COVID-like illness (OR:2.26, CI:1.57, 3.21).
Conclusions
Hip fractures present high risk for mortality and morbidity, where timely intervention is critical to improved outcomes. Presence of infection such as flu/COVID-like illness may influence mortality in patients undergoing hip fracture repair procedures. Consideration of infection status as a comorbidity is important to proper management and achieving optimal outcomes.
Introduction
SARS-CoV-2 emerged as novel coronavirus in December 2019 and quickly became a widespread pandemic with millions of cases and a large loss of lives. 1 Symptoms of COVID-19 are commonly described as flu-like but vary broadly and may include loss of smell/taste, gastrointestinal symptoms, cough, fever, fatigue, shortness of breath, pain, and others. 2 Long-term effects resulting in significant morbidity have been associated with COVID, ranging from chronic fatigue to multi-system organ damage.3,4 COVID-19 is most deadly to elder adults and those with underlying conditions such as hypertension and diabetes. 5 Elderly patients presenting with hip fractures represent an emergency and in this vulnerable population careful consideration of risks and benefits is essential. 6
Hip fractures are a critical public health concern due to significant morbidity and mortality, especially among older adults. 6 Cumulative mortality of proximal femoral fracture (PFF) 1-year post fracture is estimated to be 20-40%, with the highest risk of mortality immediately following fracture. PFF has also been associated with an increased risk of mortality from all other causes ranging from >2 to up to 8 times.7-9 A number of studies have demonstrated mortality following PFF may be increasing.8,10 Delays of >24 hours to surgery are associated with increased risk for minor complications, while delays of >48 hours are associated with major complications, with a handful of studies citing an increased risk of mortality in delays of 12-72 hours.11-13 As a result, immediate surgical intervention is recommended, though a subset of patients may not be eligible due to fragility or severe comorbidities. 14 As such, pre-operative risk assessment is critical to optimizing outcomes. 15
Given the widespread nature of COVID it is not unexpected that some patients presenting for PFF may be positive. It is therefore important to broaden our understanding of COVID’s impact on PFF so that we may better inform treatment. There is a need to determine if infection by SARS-CoV-2, in a patient with PFF but otherwise “fit for surgery” is increasing the patient’s risk for post-operative mortality and if this mortality is beyond the expected risks related to either COVID or hip surgery, separately. To assess the occurrence of these outcomes, this study utilized 2 objectives: (1) estimate mortality risk following PFFs, in patients with and without flu/COVID-like symptoms and (2) estimate mortality risk following hip fractures in patients with flu/COVID-like symptoms during the COVID epidemic vs patients with flu-like symptoms pre-dating the COVID epidemic.
Methods
Study Design and Data Sources
This study is a retrospective cohort study designed to evaluate risk of mortality of patients presenting with PFF and flu/COVID-like symptoms (ie, cough, fever, anosmia, ageusia, body aches, etc.) as defined by ICD-10 codes. Due to testing limitations in the United States, especially during the period prior to COVID specific medical codes, flu-like illness and other COVID related symptoms were defined using codes for flu, pneumonia, COVID, and associated symptoms. Classification of COVID severity was defined using codes corresponding to the NIH classification of severity of COVID which is based on presence of symptoms. 16
This study used data from the Premier Healthcare Database® (PHD). 17 The PHD is a population-based hospital research database that contains healthcare records contributed by a convenience sample of several hundred US hospitals that are members of the Premier healthcare performance improvement alliance, representing approximately 25% of annual US inpatient discharges. The PHD has been widely used for epidemiologic and health outcomes research, forming the basis of over 600 peer-reviewed publications since 2006.
Symptoms consistent with flu/COVID-like illness were used as a proxy for COVID status and were assessed in 2 cohorts representing 2 distinct time periods: 1) 2019 to represent a period without high probability of true COVID cases (Figure 1A) and 2) February 2020-September 2020 to represent a period where COVID may have occurred (Figure 1B). Diagram showing study design for A) 2019 Pre-COVID Period and B) 2020 COVID Period.
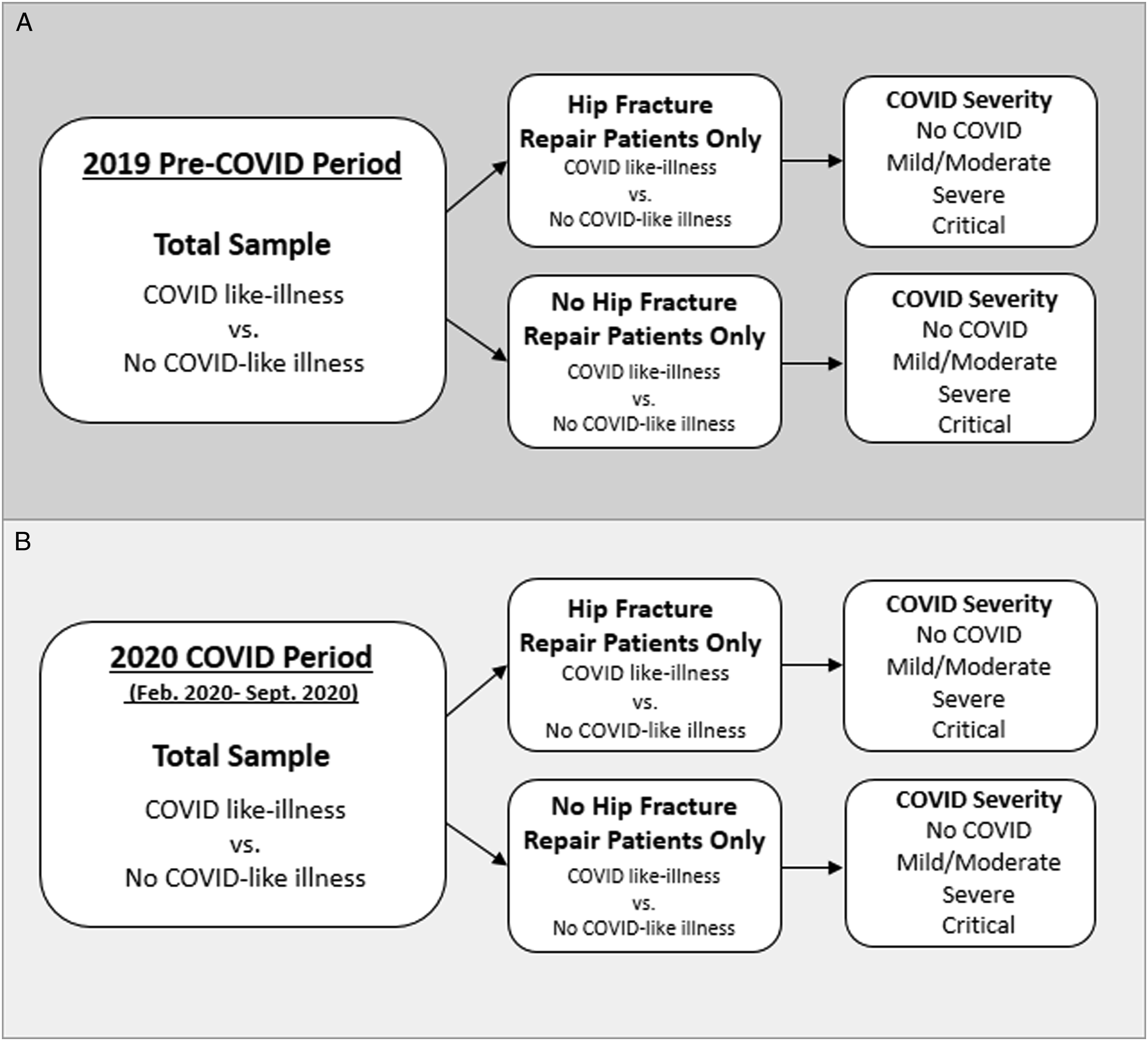
Within each time period the following groups of patients were created to assess the role of flu/COVID-like illness and the role of surgery on mortality: (1) Patients with PFF and repair with flu/COVID-like illness, (2) Patients with PFF and repair without flu/COVID-like illness, (3) Patients with PFF and no repair with flu/COVID-like illness, and (4) Patients with PFF and no repair without flu/COVID-like illness (Figure 1).
This analysis of the PHD was conducted under an exemption from Institutional Review Board oversight for US-based studies using de-identified healthcare records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46.101(b) (4)). 18 No attempts to re-identify patients were made. Only records with complete data were used for analysis.
Outcome and Covariates
The primary outcome of this study was mortality, defined as death during the hospital admission period or discharge to palliative care. Patient factors included were: age, gender, marital status and tobacco use 3 months prior to admission. Patient medical conditions were extracted from the medical record and defined using medical codes consistent with coding for the Elixhauser Comorbidity Index (ECI) and the Charlson Comorbidity Index (CCI). Most conditions were defined according to the ECI, with the exception of cancer which was defined according to the CCI due to it being more comprehensive in terms of diagnoses. 19 COVID severity was defined according to the NIH classification (see Supplemental Table 1). 16 Due to small cell counts the mild and moderate COVID severity categories were combined for the main analyses.
Statistical Analyses
Means and standard deviations were conducted for continuous values. Variables relevant for adjustment were selected according to a priori review of the literature and consideration of conditions related to COVID risk as defined by the Centers for Disease Control and Prevention (CDC). 20 Medical conditions included within the CDC list were then matched to corresponding variables including ECI or CCI values. Variables related to COVID and mortality were assessed based on a priori knowledge and existing literature. Variables related to increased mortality risk from COVID were considered within the context of the outcome mortality following PFF repair to determine variables relevant for adjustment, as presented in the adjusted models. Unadjusted and adjusted logistic regression models were used to quantify the odds of mortality associated with PFF repair surgery and flu/COVID-like status. Additional methods of model selection were employed including Backward Bayesian information criterion (BIC) selection (backward, stepwise selection) 21 which is presented alongside the adjusted models. Results from the adjusted OR models were used for discussion.
Results
Descriptive Statistics of Demographics and Covariates for the 2019 Time-Period Cohort Overall and as Stratified by Proximal Femoral Fracture Repair and Flu/COVID-like Status Groups.
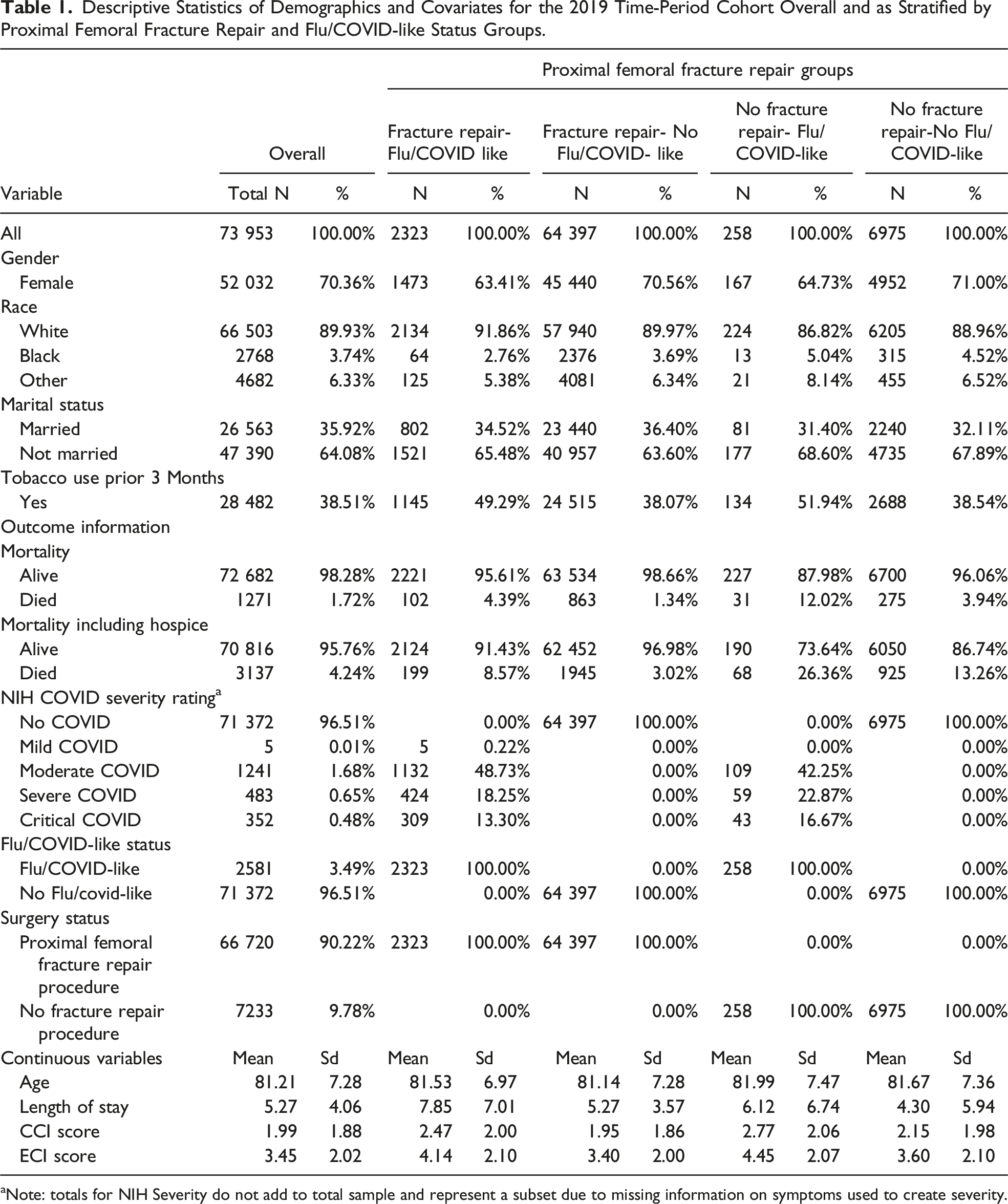
aNote: totals for NIH Severity do not add to total sample and represent a subset due to missing information on symptoms used to create severity.
Descriptive Statistics of Demographics and Covariates for February 2020-September 2020 COVID Time-Period Cohort Overall and as Stratified by Proximal Femoral Fracture Repair and Flu/COVID-Like Status Groups.

aNote: totals for NIH Severity do not add to total sample and represent a subset due to missing information on symptoms used to create severity.
Odds Ratios and 95% Confidence Intervals for Odds of Mortality Associated with Receiving a Proximal Femoral Fracture Repair Compared to Not Receiving a Repair by Time Defined Cohorts, as Stratified by Flu/COVID-Like Status.
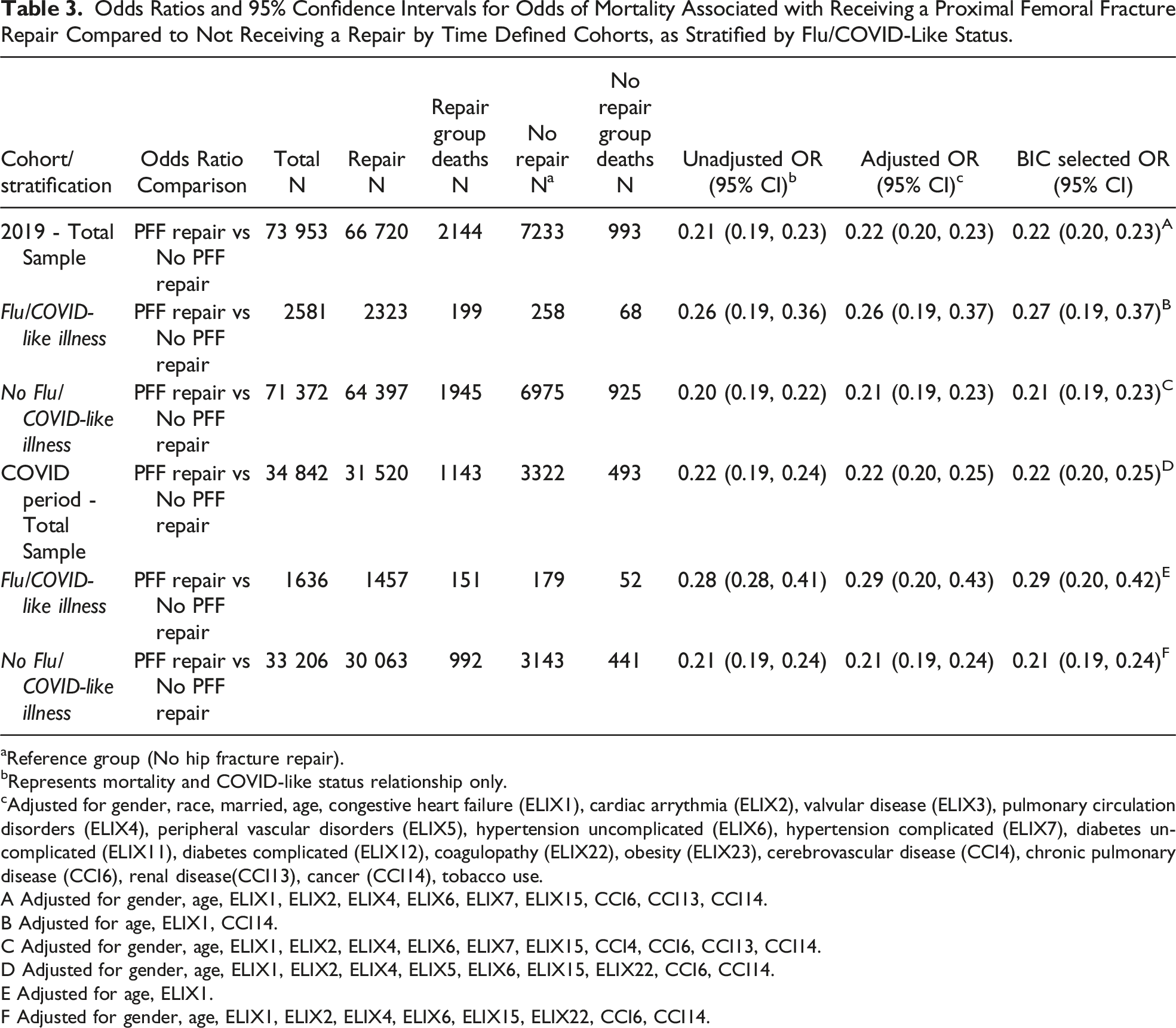
aReference group (No hip fracture repair).
bRepresents mortality and COVID-like status relationship only.
cAdjusted for gender, race, married, age, congestive heart failure (ELIX1), cardiac arrythmia (ELIX2), valvular disease (ELIX3), pulmonary circulation disorders (ELIX4), peripheral vascular disorders (ELIX5), hypertension uncomplicated (ELIX6), hypertension complicated (ELIX7), diabetes uncomplicated (ELIX11), diabetes complicated (ELIX12), coagulopathy (ELIX22), obesity (ELIX23), cerebrovascular disease (CCI4), chronic pulmonary disease (CCI6), renal disease(CCI13), cancer (CCI14), tobacco use.
A Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX7, ELIX15, CCI6, CCI13, CCI14.
B Adjusted for age, ELIX1, CCI14.
C Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX7, ELIX15, CCI4, CCI6, CCI13, CCI14.
D Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX5, ELIX6, ELIX15, ELIX22, CCI6, CCI14.
E Adjusted for age, ELIX1.
F Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX15, ELIX22, CCI6, CCI14.
Odds Ratios and 95% Confidence Intervals for Odds of Mortality Related to flu/COVID-Like Illness Compared to no flu/COVID-Like Illness by Time Defined Cohorts, and as Stratified by Proximal Femoral Fracture Repair and no Proximal Femoral Fracture Repair Patient Status.

aReference=No COVID-like illness.
bRepresents mortality and COVID-like status relationship only.
cAdjusted for gender, race, married, age, congestive heart failure (ELIX1), cardiac arrythmia (ELIX2), valvular disease (ELIX3), pulmonary circulation disorders (ELIX4), peripheral vascular disorders (ELIX5), hypertension uncomplicated (ELIX6), hypertension complicated (ELIX7), diabetes uncomplicated (ELIX11), diabetes complicated (ELIX12), coagulopathy (ELIX22), obesity (ELIX23), cerebrovascular disease (CCI4), chronic pulmonary disease (CCI6), renal disease (CCI13), cancer (CCI14), tobacco use.
A Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX7, ELIX15, CCI6, CCI13, CCI14.
B Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX7, ELIX15, CCI4, CCI6, CCI13, CCI14.
C Adjusted for gender, age, ELIX1, ELIX6, ELIX7, ELIX15, ELIX23, CCI6, CCI13, CCI14.
D Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX5, ELIX6, ELIX15, ELIX22, CCI6, CCI14.
E Adjusted for age, ELIX1, ELIX4, ELIX5, ELIX6, ELIX22, CCI6, CCI14.
F Adjusted for age, ELIX3, ELIX15, CCI6, CCI13, CCI14.
Odds Ratios and 95% Confidence Intervals for Odds of Mortality Associated with flu/COVID-Like Severity Classification by Time-Period Defined Cohort, and as Stratified by Proximal Femoral Fracture Repair and no Fracture Repair Patient Status.

This table is a subgroup analysis, as such numbers for classification are smaller than total sample.
aRepresents mortality and COVID-like status relationship only.
bAdjusted for gender, race, married, age, congestive heart failure (ELIX1), cardiac arrythmia (ELIX2), valvular disease (ELIX3), pulmonary circulation disorders (ELIX4), peripheral vascular disorders (ELIX5), hypertension uncomplicated (ELIX6), hypertension complicated (ELIX7), diabetes uncomplicated (ELIX11), diabetes complicated (ELIX12), coagulopathy (ELIX22), obesity (ELIX23), cerebrovascular disease (CCI4), chronic pulmonary disease (CCI6), renal disease(CCI13), cancer (CCI14), tobacco use.
A Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX7, ELIX15, ELIX23, CCI4, CCI6, CCI13, CCI14.
B Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX7, ELIX15, CCI4, CCI6, CCI13, CCI14.
C Adjusted for age, ELIX1, ELIX6, ELIX7, ELIX15, ELIX23, CCI6, CCI13, CCI14.
D Adjusted for gender, age, ELIX1, ELIX2, ELIX4, ELIX6, ELIX15, ELIX22, CCI6, CCI14.
E Adjusted for age, ELIX2, ELIX15, CCI6, CCI13, CCI14.
Discussion
Understanding how COVID, and potentially other infectious conditions, may impact outcomes in patients undergoing PFF repair surgery may be useful for managing the presence of disease in a similar manner that other underlying conditions are considered prior to surgery. Given the potential for significant morbidity and mortality, it may not be appropriate to warrant abstinence from repair procedures even if a patient is SARS-CoV-2 positive. As shown within our study, the odds of mortality associated with receiving a PFF repair procedure were lower compared to those who did not receive a repair procedure and were similar for the 2019 cohort (OR:0.22, CI:0.20,0.23) and the COVID period cohort (OR:0.22, CI:0.20,0.25). Further, within those who received PFF repair procedure, the odds of mortality associated with flu/COVID-like illness compared to those who did not have flu/COVID-like illness were increased in both the 2019 (OR:2.47, CI:2.11,2.88) and COVID period (OR:2.85, CI:2.36,3.42) cohort. A similar pattern was observed for those who did not have a PFF repair, though these odds were slightly attenuated compared to the previous estimates from patients who received a repair procedure (2019 OR:2.04, CI:1.50,2.75; COVID Period OR:2.26, CI:1.57,3.21). This attenuation may have resulted from reasons that the patient was not recommended for surgery and may represent biases in selection. Since we were unable to assess reasons that patients did not receive surgery, no firm conclusions can be drawn from this information. However, it should be noted that due to the high risk for morbidity and mortality without timely intervention generally only patients deemed to be too high risk for surgery do not receive surgical intervention, which may explain the association observed here.22,23 While our study found that patients with PFF and mild/moderate COVID status have increased odds of mortality compared to patients with no COVID-like symptoms, in line with previous findings, 24 our study lacks data on asymptomatic patients who may be captured in the no flu/COVID-like group. Regardless, even an asymptomatic case should be considered for its potential effect on patients undergoing PFF repair procedures to optimally manage the patient and needed healthcare resources including management and resource allocation. Further, while this study could not ascertain COVID testing status, the use of a proxy in this study may also demonstrate the potential need to consider not just COVID, but potentially any viral illness. This is supported by the similarity of estimates in the flu/COVID-like illness group for both 2019 and 2020 COVID time periods, though mortality was higher during the 2020 COVID period.
Kayani et al investigated the effects of COVID-19 status and post-operative complications in PFF patients and found that compared to COVID negative patients, COVID positive patients had significantly longer lengths of stay (13.8 days vs 6.7 days), more admissions to critical care (61.0% vs 18.2%), more complications (89.0% vs 35.0%), and increased mortality rates (30.5% vs 10.3%). Approximately half the patients who were included in the COVID positive group had negative swabs on admissions indicating that they may have contracted COVID during their stay. This study also found that positive patients who had 4 or more comorbidities had the greatest risk, a valuable finding given that hip fractures are common in the elder population where a higher number of comorbidities is expected. 25
Hall et al also assessed the effects of COVID-19 status on PFF outcomes and found that among the 27 COVID-positive patients compared to the 290 COVID-negative patients, there was significantly lower 30-day survival (64.5% (CI:45.7,83.3) vs 91.7% (CI:88.2,94.8)), though the small sample size likely contributed to relative imprecision. Hall et al 26 also noted the presence of asymptomatic carriers which should be considered. 26 Results from Muñoz-Vives et al 24 support an increase in mortality among PFF patients, noting that hospitals with more COVID cases had higher mortality rates. 24 LeBrun et al also found that despite a similar number of comorbidities between groups, positive COVID status was associated with increased mortality in PFF patients. 27
This study has several limitations that should be considered alongside its results. First, this study was unable to directly confirm SARS-CoV-2 infection due to a lack of available testing data within PHD. Instead, flu/COVID-like symptoms were used as a proxy for SARS-CoV-2 infection. In the US, there was a shortcoming of testing availability during the earlier stages of COVID-19. Use of SARS-CoV-2 infection test positive cases only may have led to an overestimation of mortality as only the COVID-19 most severe cases received tests. Thus, a broad consideration of potential cases still confers benefit to this analysis and should be interpreted in light of this limitation. The early stages of COVID also lacked a specific diagnosis code to identify COVID patents further lending to potential missed cases if diagnosis alone was considered. Finally, due to the cross-sectional nature of the Premier database, patients that may have expired at home shortly after discharge are not captured within our mortality outcome, even while accounting for discharges to palliative care. It should be considered that as a result the associations presented here may be underestimated.
Conclusions
Patients with PFF represent emergent cases with high risk for mortality and morbidity. COVID status may influence mortality in patients sent for surgical repair of PFF, though regardless of COVID status, PFF repair procedures are associated with lower odds of mortality compared to those who did not receive them. It may be beneficial to consider COVID status, for management as a comorbidity. Further, due to the similarity of estimates in mortality from the 2019 and 2020 time periods, consideration of other viral illnesses such as the flu may also be warranted to ensure optimal patient and resource management.
Supplemental Material
Supplemental Material - Risk of Mortality for Proximal Femoral Fracture in Patients With and Without COVID-19. A Retrospective Cohort Study
Supplemental Material for Risk of Mortality for Proximal Femoral Fracture in Patients With and Without COVID-19. A Retrospective Cohort Study by Ashley Holub, PhD, Montsant Jornet-Gibert, PhD, Jill Ruppenkamp, MS, Chantal E. Holy, PhD, Juan Daccach, MD, Pere Torner, MD, PhD, Pedro Caba-Doussoux, MD, and Josep Maria Muñoz Vives, MD in Geriatric Orthopaedic Surgery & Rehabilitation
Supplemental Material
Supplemental Material - Risk of Mortality for Proximal Femoral Fracture in Patients With and Without COVID-19. A Retrospective Cohort Study
Supplemental Material for Risk of Mortality for Proximal Femoral Fracture in Patients With and Without COVID-19. A Retrospective Cohort Study by Ashley Holub, PhD, Montsant Jornet-Gibert, PhD, Jill Ruppenkamp, MS, Chantal E. Holy, PhD, Juan Daccach, MD, Pere Torner, MD, PhD, Pedro Caba-Doussoux, MD, and Josep Maria Muñoz Vives, MD in Geriatric Orthopaedic Surgery & Rehabilitation
Supplemental Material
Supplemental Material - Risk of Mortality for Proximal Femoral Fracture in Patients With and Without COVID-19. A Retrospective Cohort Study
Supplemental Material for Risk of Mortality for Proximal Femoral Fracture in Patients With and Without COVID-19. A Retrospective Cohort Study by Ashley Holub, PhD, Montsant Jornet-Gibert, PhD, Jill Ruppenkamp, MS, Chantal E. Holy, PhD, Juan Daccach, MD, Pere Torner, MD, PhD, Pedro Caba-Doussoux, MD, and Josep Maria Muñoz Vives, MD in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Johnson and Johnson.
Supplemental Material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.