
Abstract
Introduction
Supercapsular Percutaneously-Assisted Total Hip (SuperPATH) approach is a novel minimally invasive surgical technique for total hip arthroplasty (THA). This meta-analysis was conducted to evaluate the outcomes following THA via the SuperPATH approach in elderly patients with femoral neck fractures (FNFs), compared with those via traditional surgical approaches.
Methods
Eligible studies were retrieved through searching 7 electronic databases and manually screening related references. Objectives were surgical-related parameters, functional outcomes, and incidence of postoperative complications.
Results
9 comparative studies were included. Pooled results suggested that at the cost of longer operative time (WMD: 14.25, 95% CI: 3.25 to 25.25), the SuperPATH technique was superior to traditional approaches regarding incision length (WMD: −4.51, 95% CI: −6.46 to −2.56), intraoperative blood loss (WMD: −80.47, 95% CI: −122.36 to −38.57), and hospital stays (WMD: −3.35, 95% CI: −5.05 to −1.65). SuperPATH groups exhibited significantly increased Harris Hip Scores within 1 month after surgery (7d, WMD: 9.85, 95% CI: 6.40 to 13.30; 14d, WMD: 10.68, 95% CI: 8.29 to 13.08; 1 month, WMD: 6.17, 95% CI: 3.56 to 8.78) and had a reduced incidence of overall complications (OR: .19, 95% CI: .09 to .41). No significant differences were found between the 2 groups regarding postoperative pain relief.
Conclusion
Elderly patients with FNFs are potential candidates for THA treatment via the SuperPATH technique, which is associated with improved surgical outcomes, better short-term functional recovery, and lower risk of total complications as compared to traditional approaches. Additional studies are needed to further confirm our conclusions and validate the long-term efficacy of SuperPATH.
Keywords
Introduction
Femoral neck fractures (FNFs), a major public health issue contributing substantially to morbidity and mortality worldwide, often occur in the senile population owing to decreased bone mineral density and increased rate of falling or twisting.1,2 Currently, the world is facing an aging problem and a growing trend of the incidence of FNF. 3 The treatment of FNF, therefore, remains a significant subject of contentious discussion. Total hip arthroplasty (THA), regarded as one of the most successful orthopedic surgical interventions, has been an increasingly popular option for treating FNF due to its potential for less pain, better functional outcomes, and a lower risk of revision.4,5
The most widely used surgical techniques for THA in patients with FNFs include the posterolateral and lateral (anterolateral and direct lateral) approaches.1,6-10 Despite their prevalence, these conventional methods have been reported to have an elevated risk of soft tissue damage, large perioperative blood loss, and postoperative complications such as dislocation and nerve injury. 4 Development of minimally invasive surgical (MIS) methods was therefore propelled into the forefront of current investigation for the prospects of overcoming their disadvantages. 5 Notably, the Supercapsular Percutaneously-Assisted Total Hip Arthroplasty (SuperPATH) approach, a novel MIS technique that combines elements of the Supercapsular and the PATH techniques, has aroused the interest of more and more orthopedic surgeons since its introduction by Dr Chow in 2011. 11 The SuperPATH technique is a modification of the standard posterior approach with added benefits of avoiding disturbing the iliotibial band and allowing intact external rotator muscles, which can further contribute to decreased trauma and accelerated recovery.11,12 Previous publications had demonstrated that this technique for THA could afford early mobilization, shortened length of hospital stay, and less postoperative pain, compared with traditional methods.4,5,13
However, the outcomes following THA procedures via the SuperPATH approach in elderly patients with FNFs, in comparison to normal approaches, have been inconclusive. Additional information is needed to establish the efficacy profile of this novel approach in this condition. Consequently, this meta-analysis was undertaken to collate findings across studies that focused on the comparisons between the Super PATH and conventional approaches for THA, thereby seeking evidence for the efficacy of the SuperPATH technique for the treatment of geriatric FNFs.
Methods
Literature Search
The present study conformed to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses, abbreviated as PRISMA. 14 A comprehensive search for all relevant studies up to September 2020 was performed using electronic databases including Embase, Pubmed, Scopus, Web of Science, Cochrane Library, China National Knowledge Infrastructure (CNKI), and Wanfan database. Additionally, we manually screened the bibliographies of potentially related papers for additional citations. The following keywords were used in various combinations for database-searching: supercapsular percutaneously-assisted approach, SuperPATH, hip arthroplasty, hip replacement, total hip arthroplasty, total hip replacement, hip fracture, femoral neck fracture, and femur neck fracture. After a searching process, 2 independent reviewers first scanned titles and abstracts of potentially relevant papers and then further scanned the articles by reading full texts to confirm whether these papers could meet the inclusion criteria.
Selection Criteria
Eligible studies fulfilled the predetermined criteria as per PICOS: (1) population: limited to elderly patients (aged≧60) suffering from FNFs; (2) intervention and comparison: patients receiving THA via SuperPATH approach in comparison with conventional surgical approaches; (3) outcomes of interest: reporting at least 1 outcome related to surgery, function, or postoperative complications; and (4) study design: given the paucity of data, both randomized trials and observational studies were considered eligible for inclusion. Original articles written in English or Chinese were available. Single-arm follow-up studies that lacked a control group were excluded. Any disagreement was resolved after close consultation with a third reviewer.
Data Extraction
Two reviewers independently tabulated extracted data into a predefined spreadsheet and subsequently compared results with each other for verification. In event of any discrepancy, a third reviewer was consulted. The following information was captured: first author, year of publication, location, study design, sample size, patient characteristics (e.g., age and gender), description of intervention and comparison, and outcomes of interest. Regarding surgery-related parameters, we extracted data of operation time (min), incision length (cm), intraoperative blood loss (mL), length of hospital stay (day), and pain intensity scores (Visual Analogue Scale, VAS). Harris hip scores, namely, HHS, were extracted for a functional index after surgery.
Quality Assessment
Methodological quality evaluation for each paper was 2-fold. The Cochrane Collaboration tool was used for assessing randomized controlled trials (RCT). This tool comprises 7 domains, where each study was judged as having a high, unclear, or low risk of bias. 15 On the other hand, non-RCTs were assessed with the MINORS (methodological index for non-randomized studies) scale that consists of twelve items. Each study was scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate) regarding every item. 16 The aggregate MINORS score ranges from 0 to 24 points and 1 study scoring ≧20 points was judged as a high-quality study. Two independent reviewers appraised the methodological quality, and a third reviewer was consulted for any doubts.
Data Analysis
Our objectives were surgical-associated parameters, functional outcomes, and incidence of complications after THA. During data analysis, the “control group” was defined as patients treated by THA via conventional approaches. All analyses were conducted using Stata 15.1 version (Stata Corporation). The continuous data were calculated by weighted mean difference (WMD) and their 95% confidence intervals (CIs). The odds ratio (OR) and corresponding 95% CIs were determined for dichotomous outcomes. A 95% CI without 0 for WMD or without 1 for OR was suggestive of statistical significance. A random-effect model was employed to calculate overall estimates in data synthesis where there was proof of significant heterogeneity among studies, and a fix-effect model was used otherwise. The heterogeneity of each study was measured using I2 statistics, with an I2 >50% indicating a significant degree of heterogeneity. 15 For interpretation of significant heterogeneity, sensitivity analyses were performed by sequential omission of individual studies. 15 Furthermore, Begg’s and Egger’s tests were carried out to assess the publication bias for analyses that included at least 5 studies, with a P-value <.05 serving as the evidence of publication bias. 15
Results
Study Selection
According to search strategy, 387 citations were first identified from electronic database searches and manual searches of reference lists of pertinent studies, followed by the removal of 175 duplicated records. Then, 212 records underwent screening based on titles and abstracts and 37 papers remained as potential candidates for full-text evaluation of eligibility. Ultimately, a total of 9 articles17-25 were proved eligible and included in the present meta-analysis. A detailed flowchart of study recruitment is presented in Figure 1. Flowchart of study selection process according to PRISMA statement. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; HA: Hemiarthroplasty; THA: Total hip arthroplasty.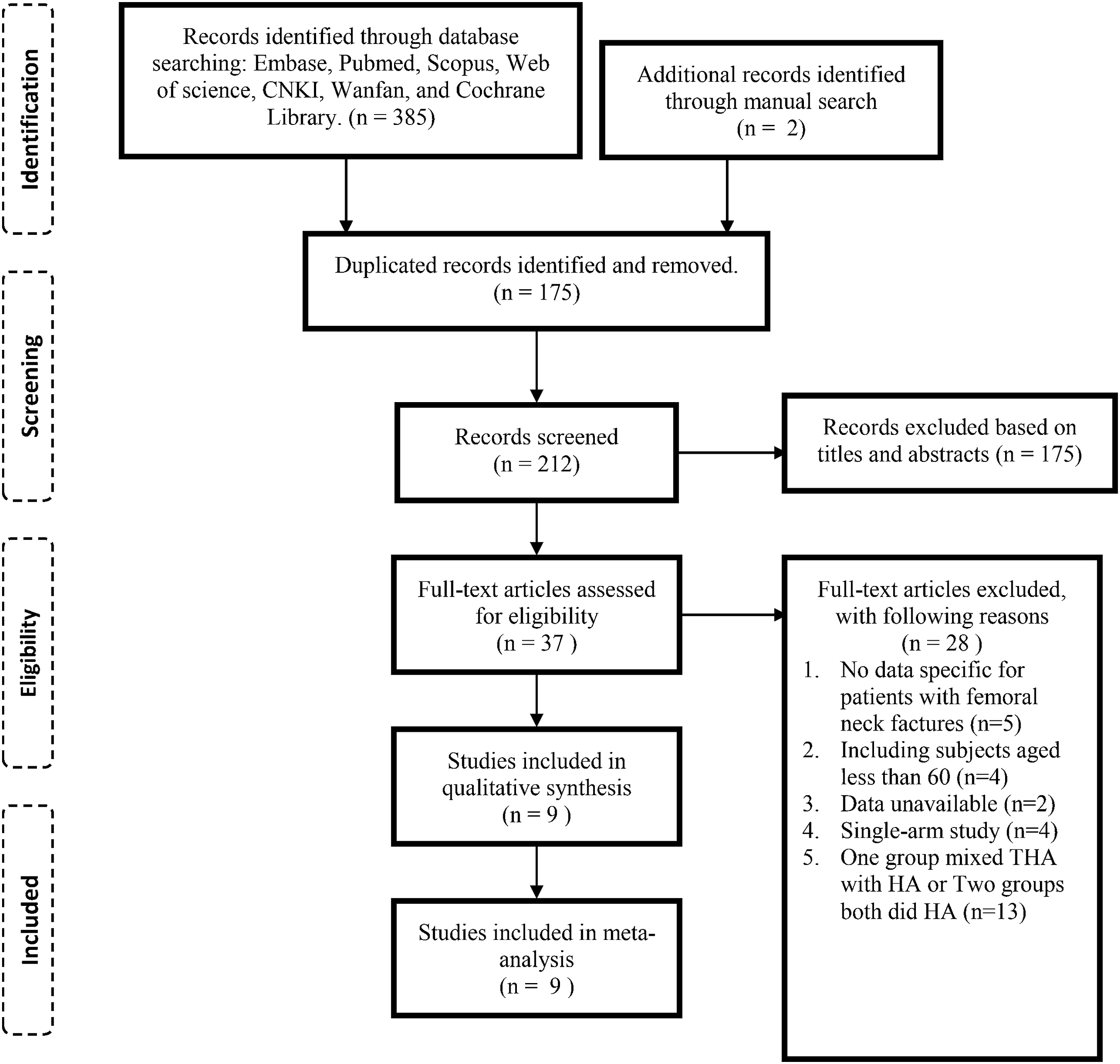
Study Characteristics
Characteristics of included studies.
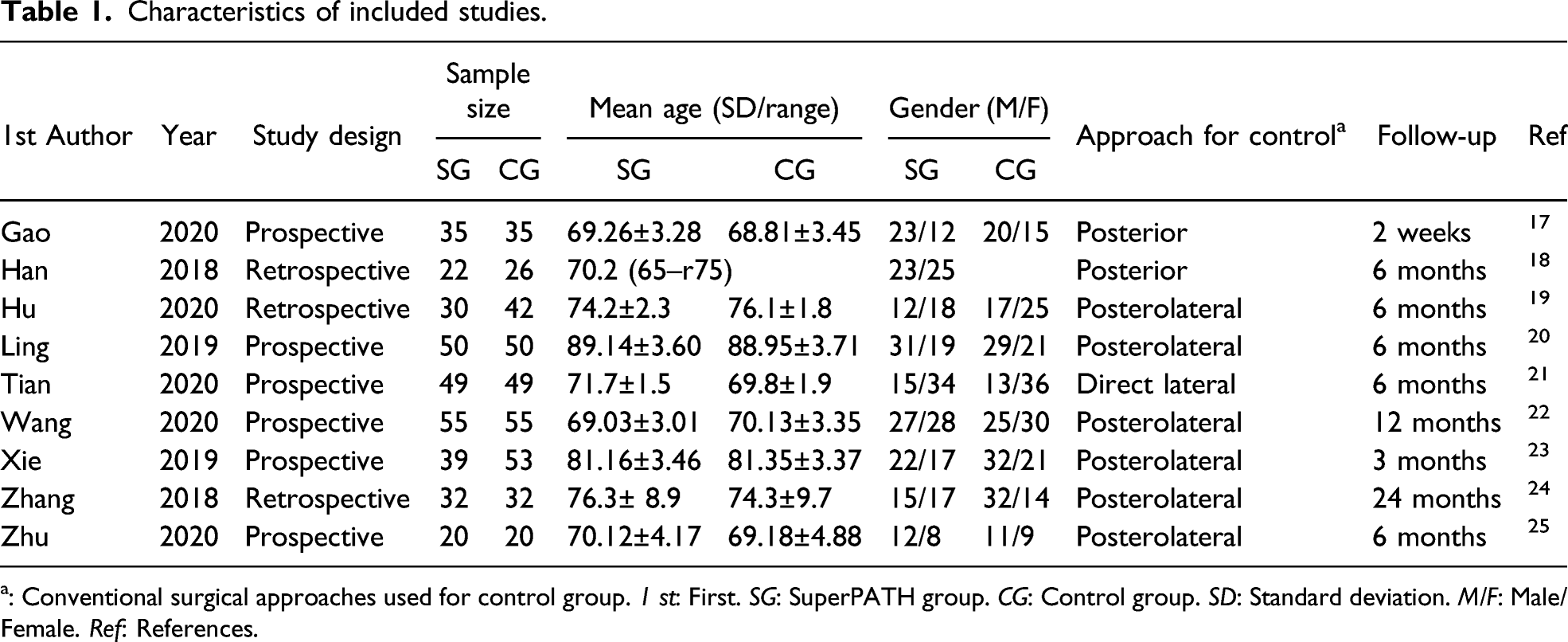
a: Conventional surgical approaches used for control group. 1 st: First. SG: SuperPATH group. CG: Control group. SD: Standard deviation. M/F: Male/Female. Ref: References.
Quality Assessment
Quality assessment of included studies according to MINORS scale.

Notes: MINORS stands for methodological index for non-randomized studies. Each item is scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). The ideal total MINORS score is 24 points
Surgery-Related Outcomes
Data of incision length (7 studies), intraoperative blood loss (9 studies), operation time (8 studies), and length of hospital stay (5 studies) were captured. Among included studies, the SuperPATH group had an average incision length in the range of 6.65–7.60 cm, an average intraoperative blood loss in the range of 88.62–515.60 mL, an average operation time in the range of 66.06–118.25 min, and an average hospital length of stay in the range of 7.77–14.62 d. Those above in the control group were in the range of 7.58–17.08 cm, 108.27–484.40 mL, 61.56–102.51 min, and 8.96–14.62 d, respectively. Pooled results suggested that THA via SuperPATH approach significantly contributed to favorable surgical outcomes, including smaller inclusion (Figure 2a; WMD: −4.51, 95% CI: −6.46 to −2.56), reduced intraoperative blood loss (Figure 2b; WMD: −80.47, 95% CI: −122.36 to −38.57), and shortened hospitalization period (Figure 2d; WMD: −3.35, 95% CI: −5.0 to −1.65); however, it entailed significantly longer procedure time (Figure 2c; WMD: 14.25, 95% CI: 3.25 to 25.25). Sensitivity analyses demonstrated that no individual study impacted pooled data, so the results were proved to be robust. Overall estimates for incision length (a), intraoperative blood loss (b), operation time (c), and length of hospital stay (d). WMD: weighted mean difference; CI: Confidence intervals.
Furthermore, consolidated results regarding postoperative pain that was measured using a VAS among 9 studies are displayed in Figure 3. No significant differences were generated in favor of SuperPATH groups in terms of postoperative pain intensity scores 7 days (WMD: −.41, 95% CI: −.97 to .14), 1 month (WMD: −.15, 95% CI: −.33 to .03), 6 months (WMD: −.13, 95% CI: −.28 to .02), or 12 months (WMD: −.14, 95% CI: −.27 to −.00). According to sensitivity analyses, the pooled estimates for postoperative 7-day VAS became significant (WMD: −.67, 95% CI: −1.25 to −.10) and the heterogeneity decreased to a moderate degree (from 79.5 to 63.0%), after omitting the study of Zhang et al.
24
who attributed the non-superiority of SuperPATH regarding postoperative pain relief to the inexperience in this novel surgical technique in the discussion. Overall estimates for pain intensity scores (VAS) at postoperative 7 days, 1, 6, and 12 months. WMD: weighted mean difference; CI: Confidence intervals; post-op: postoperatively.
Hip Functional Outcomes
Functional outcomes were measured using HHS among included trials. As reported by 5 studies,17,18,20,21,25 significant differences were found in the HHS before and after surgery, indicating that both the SuperPATH and conventional surgical approaches could help improve the functional quality. Combined estimates for HHS after 7 days, 14 days, 1, 3, 6, and 12 months are summarized as a forest plot in Figure 4. The superiority of SuperPATH in terms of functional outcomes was apparent within the first month postoperatively, based on significantly higher HHS points postoperative 7 days (WMD: 9.85, 95% CI: 6.40 to 13.30), 14 days (WMD: 10.68, 95% CI: 8.29 to 13.08), and 1 month (WMD: 6.17, 95% CI: 3.56 to 8.78) in favor of the SuperPATH. Subsequently, the SuperPATH and control groups attained comparable HHS values after 3 months (WMD: 3.23, 95% CI: −.82 to 7.28); 6 months later, the results remained balanced (WMD: 1.68, 95% CI: −.09 to 3.45). As for long-term efficacy, HHS following 12 months in both groups was at the more similar levels based on 2 studies (WMD: .09; 95% CI: −.90, 1.08). Besides, there was 1 study suggesting no significant difference between 2 groups under a 24-month follow-up (P = .86).
24
Overall estimates for the Harris Hip Scores at postoperative 7 days, 14 days, 1, 3, 6, and 12 months. WMD: weighted mean difference; CI: Confidence intervals; post-op: postoperatively.
A summary of sensitivity analyses on function outcomes.

awithout 0 indicating the existence of significant differences between 2 groups.
HHS: Harris hip score; WMD: Weighted mean differences; CI: confidence intervals; BMI: body mass index.
Postoperative Complications
Three studies22,24,25 reported no occurrence of complications such as infection, extremity venous thrombosis, prosthesis loosening, periprosthetic fracture, or dislocation during the follow-up period. Meta-analysis was performed based on the remaining 6 studies (560 patients) and the overall incidence of post-surgical complications is presented in Figure 5. Elderly patients receiving THA via the SuperPATH approach rather than traditional surgical approaches had a significantly decreased risk of complications following operation (OR: .19, 95% CI: .09 to .41, I2: 0%); however, when data were further stratified according to common complications: dislocation, infection, urinary retention, wound bleeding, and deep venous thrombosis (DVT) of the lower extremity, no significant differences were demonstrated between 2 groups. Summarized outcomes are shown in Table 4. Overall estimates for the incidence of total complication after surgery. OR: odds ratio; CI: Confidence intervals. Summarized outcomes of postoperative complications between SuperPATH and control groups. Ref: References; OR: odds ratio; CI: confidence intervals; DVT: deep venous thrombosis; FE: fixed-effect.

Publication Bias
No publication bias was detected based on the following results under Begg’s and Egger’s test: incision length (7 studies, P = .340); intraoperative blood loss (9 studies, P = .358); operative time (8 studies, P = .104); length of hospital stay (5 studies, P = .826); postoperative 1-month HHS (6 studies, P = .270); postoperative 6-month HHS (6 studies, P = .620); and total complications (6 studies, P = .072).
Discussion
THA remains the main treatment option for elderly patients with FNF and the choice of surgical technique can serve as one factor potentially associated with failed THA treatment.22,26 As a novel MIS technique, the SuperPATH is gaining growing popularity, especially among Chinese surgeons since its introduction to China in 2014. 5 However, the benefit of the SuperPATH in orthopedic trauma surgery has yet to be elucidated. To our knowledge, this is the first meta-analysis to collate findings across studies that compared the outcomes between the SuperPATH technique and traditional surgical approaches for elderly FNFs treated by THA. On the basis of 9 included studies involving 694 elderly patients aged 60 or more, our analysis indicated that at the expense of longer operative time, the SuperPATH technique exhibited significant advantages over conventional approaches in terms of intraoperative bleeding, incision length, hospital stays, short-term functional recovery, and the risk of total complication events; no significant difference, however, was found in favor of the SuperPATH regarding pain relief.
Conventional surgical approaches for THA have their shortcomings, such as larger incisions, increased muscular damage, increased amount of bleeding, and delayed postoperative recovery.4,5 Our results pertaining to surgical parameters suggested that the SuperPATH could effectively help overcome these disadvantages. Sensitivity analyses did not identify the clear source of high heterogeneity, for which a mixture of prospective and retrospective study designs among included studies could be responsible; no individual study was found to affect the combined results, which further confirmed the stability of results. The SuperPATH technique allows preservation of short external rotators and then provides smaller soft tissue dissection, which contributes greatly to decreased trauma, less bleeding, and reduced length of stay in hospital. Surgical blood loss is always a matter of great concern among orthopedic surgeons due to its close association with blood transfusion and blood-related complications. Furthermore, Gofton and Fitch 27 reported that the adoption of SuperPATH led to in-hospital cost reductions of over 28% as compared to the traditional method. Notably, enough decreases in length of stay and transfusions could account for the majority of savings. Hence, the SuperPATH may come as a boon for the elderly population with a higher surgical risk. 28
Of note, we observed remarkably prolonged operation time and no superiority of pain relief in the SuperPATH group, which were associated with the learning curve of surgeons’ proficiency in adopting this novel technique. The SuperPATH technique is still in its infancy in the field of orthopedics and surgeons inevitably require longer time learning, adapting, and performing this approach. The pooled result suggested that after omitting the study of Zhang et al., 24 there was a significant difference between the 2 groups in terms of 7-day VAS. According to Zhang et al., 24 unfamiliarity with the surgical process and related surgical instruments might lead to no superiority of this tissue-sparing technique in terms of early pain relief, implying that the analgesic efficacy of SuperPATH was associated with the skilled operation. Besides, two previous studies focusing on its learning curve demonstrated that the operative time of the SuperPATH continued to decrease by case 5012 and by case 4029, respectively, where surgeons achieved more familiarity with this technique. Also, there existed relatively short length of stay and low complication rates even during the learning curve. It is therefore suggested that the SuperPATH could be generalized to orthopedic surgeons. Additional studies are encouraged to take the learning curve into consideration and better define its additional benefit of relieving pain in the future.
In addition, our analysis suggested that elderly patients with FNFs treated by THA via the SuperPATH technique achieved significantly better functional outcomes within the first month after surgery, as compared to those in control groups. This result was in conflict with what Ramadanov et al. 30 had analyzed in their meta-analysis, 30 which compared the SuperPATH with conventional approaches in the setting of hip replacement for treating hip joint diseases and fractures based on several RCTs and reported that no significant differences were found between the 2 groups with regard to HHS at 14 days or 1 month postoperatively. However, consistent with Ramadanov et al., 30 we also found that the subsequent HHS at 3, 6, and 12 months postoperatively were similar in the 2 groups, indicating that the SuperPATH is associated with better short-term functional recovery, and there is weak evidence of a link between this technique and long-term functional improvement. It is well noted that our results regarding hip function should be viewed with caution. Discrepancies in eligibility criteria for enrolled subjects among studies are likely to cause heterogeneity in the analyses of functional endpoints based on our sensitivity analyses. More importantly, there existed limited value of HHS which consisted of function and pain domains, in evaluating the functional outcome in elderly patients with FNFs treated by THA. HHS is a simple rating system most widely used for the disabled hips, which was used as a function index among our included papers considering some factors such as the education and participation levels of the senile. However, Reuling et al. 31 suggested that a patient receiving a pain-free arthroplasty but having an impaired hip function still could attain a reasonable HHS, which indicated that pain section would lead to reduced reliability of HHS for measuring hip functions. Based on this limitation, future studies should consider using a modified HHS omitting pain for more accurate confirmation of the functional outcomes following THA via SuperPATH.
Although the total number of patients who experienced postoperative complications significantly reduced in the SuperPATH group compared to those in the control group, the 2 groups shared similarities when data were stratified according to 5 common complications (Table 4). Notably, the SuperPATH approach was able to avoid dislocation of the hip during THA, which could theoretically contribute to a lower dislocation risk. 11 An early report of the SuperPATH THA for femoral neck fragility fractures had suggested a low dislocation rate, 4 but we found no superiority of the SuperPATH in terms of dislocation when compared with conventional approaches in the present study. The reason for this might be that the complications could be underestimated due to relatively short follow-up periods among our included studies, half of which just had a 6-month follow-up period. Further studies are needed to establish a more robust profile for this novel technique pertaining to its contribution to decreased dislocation risks.
Attention should be paid to performing this MIS technique. The mere pursuit of a short incision is no guarantee of satisfactory results. The SuperPATH has the potential for inaccuracy of cup position owing to the narrowed field of vision caused by minimal dissection. Therefore, the SuperPARH THA should be conducted with the aid of sufficient exposure to C-arm fluoroscopy and detailed plans should be established in preparation for the surgery, such as estimating the length of femoral necks and selecting the impact design.17,24,29 Moreover, future research should document the cup and stem positioning and highlight any positioning issue such as varus stems and vertical cups during SuperPATH procedures, so as to help surgeons incorporate this innovative technique into their own practice more safely. In addition, the surgeons should equip themselves with enhanced knowledge of anatomical landmarks and enriched experience in THA surgery. Based on the fact that the SuperPATH technique processes extendability to the classic posterior approach, it is recommended to convert the SuperPATH approach into the traditional method to avoid errors if failed incision minimalization occurs during the learning curve.11,12,29
Several limitations to the present investigation should be listed: (1) a limited number of non-randomized comparative studies contributed data (collected prospectively or retrospectively) to the meta-analysis and there was insufficient data for measuring some endpoints, such as postoperative VAS (only 2–4 studies included); (2) there was inadequacy of eligible RCTs, which resulted in our weakened power to make a rigorous conclusion, and meanwhile, an unclear risk existed in most of the studies due to blind assessment of endpoints not being stated, except for 1 study 19 ; (3) the English literature available related to the SuperPATH was sparse and all our selected studies were conducted in China and almost written in Chinese, which could engender some bias in the analysis; and (4) there were relatively small sample sizes and short follow-up periods among included papers (only 1 study 24 having a 2-year follow-up), leading to a lack of comprehensive evaluation of this technique regarding its long-term effects. With the rise of this novel MIS technique, more prospective randomized comparative studies, enrolling more patients and with a long-time follow-up period, are needed to provide more robust evidence for the application of SuperPATH in THA for the treatment of elderly FNFs.
Conclusion
In summary, this meta-analysis was here to validate the role of the SuperPATH in the setting of elderly FNFs. Elderly patients with FNFs are potential candidates for the treatment of THA via the SuperPATH technique, based on the results that the SuperPATH is associated with smaller incision length, reduced intraoperative blood loss, shortened hospital length of stay, short-term functional improvement, and decreased risk of overall complications, in comparison to conventional surgical approaches. No superiority of SuperPATH was found in terms of postoperative pain relief. As a novel surgical technique, the SuperPATH is linked to prolonged surgical time and attention should be paid during the operation. Outcomes should be viewed with caution due to heterogeneity, the limited value of HHS, and limited included studies. More RCTs with larger sample sizes and longer follow-up periods are encouraged to provide more robust evidence for our conclusions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.