
Abstract
Introduction:
This study sought to investigate whether a validated trauma triage tool can stratify hospital quality measures and inpatient cost for middle-aged and geriatric trauma patients with isolated proximal and midshaft humerus fractures.
Materials and Methods:
Patients aged 55 and older who sustained a proximal or midshaft humerus fracture and required inpatient treatment were included. Patient demographic, comorbidity, and injury severity information was used to calculate each patient’s Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA). Based on scores, patients were stratified to create minimal, low, moderate, and high risk groups. Outcomes included length of stay, complications, operative management, ICU/SDU-level care, discharge disposition, unplanned readmission, and index admission costs.
Results:
Seventy-four patients with 74 humerus fractures met final inclusion criteria. Fifty-eight (78.4%) patients presented with proximal humerus and 16 (21.6%) with midshaft humerus fractures. Mean length of stay was 5.5 ± 3.4 days with a significant difference among risk groups (P = 0.029). Lower risk patients were more likely to undergo surgical management (P = 0.015) while higher risk patients required more ICU/SDU-level care (P < 0.001). Twenty-six (70.3%) minimal risk patients were discharged home compared to zero high risk patients (P = 0.001). Higher risk patients experienced higher total inpatient costs across operative and nonoperative treatment groups.
Conclusion:
The STTGMA tool is able to reliably predict hospital quality measures and cost outcomes that may allow hospitals and providers to improve value-based care and clinical decision-making for patients presenting with proximal and midshaft humerus fractures.
Level of Evidence:
Prognostic Level III.
Keywords
Introduction
Proximal humerus fractures account for 4-5% of all fractures and are the third most common fracture in older patients with the highest incidence occurring among individuals aged 73-78 years old. 1 -3 In older patients, low velocity falls are the most common mechanism of injury with 87-93% of all proximal humerus fractures sustained secondary to falls from standing height. 1,3 -5 Similarly, midshaft humerus fractures account for approximately 2% of all fractures with older patients often sustaining injuries secondary to low energy falls. 6,7 Standard treatment for many nondisplaced or minimally displaced proximal and midshaft humerus fractures is nonoperative management with focused physiotherapy and appropriate time for healing. 8,9 However, large scale studies have demonstrated a rise in the surgical management of proximal and midshaft humerus fractures. 10,11
Upper extremity fractures in older patients account for considerable health care costs, often leading to prolonged hospitalization related to advanced age and living conditions. 12 Estimates from the United States Census Bureau project the population aged 65 and older to nearly double from 2012 to 2050, and the expanding older population has necessitated an increase in the number of proximal and midshaft humerus fractures requiring inpatient care. 11,13 -15 Yet, only 43% of patients aged 65 and older are discharged home following admission for a proximal humerus fracture. 16 Coupled with the rising costs of post-acute care facilities, relative to home discharge, older patients with humerus fractures face a potentially significant economic burden. 17
Given the foreseeable transition from fee-for-service toward a bundled payment model in the field of orthopedic trauma, it is also important that providers and hospital systems be able to predict patient outcomes and quantify excess cost expenditures to optimize value-based care. 18 Although several studies have identified risk factors affecting hospital length of stay, complications, discharge disposition, and cost following humerus fractures, these studies provide little functional and clinical value because they do not collectively integrate variables into a single usable scoring system to risk stratify patients. 19 -21 Risk stratification of middle-aged and geriatric patients with fractures has identified a number of differences between hospital quality outcomes, discharge disposition distributions, and cost across the spectrum of minimal to high risk patients. 22 -27 Therefore, the primary aim of this study is to demonstrate whether a validated trauma triage tool can be used to stratify middle-aged and geriatric patients with proximal and midshaft humerus fractures regarding hospital quality metrics, discharge disposition, readmission rate, and cost. Secondarily, this study sought to quantitatively characterize these metrics for this subset of patients after stratifying by surgical management.
Materials and Methods
Research was performed at an urban, academic hospital with level I trauma center designation. Between September 2014 and September 2018, patients aged 55 and older who presented to the emergency department and sustained a proximal (OTA 11-A/B/C) or midshaft (OTA 12-A/B/C) humerus fracture that required inpatient admission were eligible for this study. Patients with concomitant fractures or those who underwent surgical management for any concomitant injury (e.g. hemoperitoneum) were excluded. Humerus injuries occurred following low or high energy mechanisms of injury. Low energy mechanisms of injury included falls from standing or ≤ 2 stairs. High energy mechanisms of injury included falls from height > 2 stairs, motor vehicle accidents, motorcycle accidents, motor vehicle pedestrian collisions, or motorcycle pedestrian collisions. All relevant information from the initial emergency department assessment and subsequent hospitalization was extracted from electronic medical records and recorded in an IRB-approved database.
Patient demographic, comorbidity, and injury severity information was collected on initial emergency department evaluation. Study variables included age, Glasgow Coma Scale (GCS) at presentation, Charlson Comorbidity Index (CCI), as well as Abbreviated Injury Severity sub-scores for the Head & Neck (AIS-HN), Chest (AIS-Chest), and Extremity & Pelvis (AIS-EP). These variables were used to calculate each patient’s Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA), which represents the predicted risk of inpatient mortality during the index hospitalization (scale: 0-100%). As previously described, patients were stratified into 4 groups based on these scores to create a minimal risk (< 1.2%), low risk (1.2-3.2%), moderate risk (3.2-9.4%), and high risk group (> 9.4%). 23
Information on length of stay (LOS), complications, surgical management, need for intensive care unit (ICU) or step-down unit (SDU) level care, and discharge disposition was gathered throughout the index hospitalization. Criteria for ICU/SDU-level care included critical illnesses/injuries that acutely impair one or more vital organ systems (e.g. changes in hemodynamic, pulmonary, and neurologic function). Complications included acute renal failure, surgical site infection, decubitus ulcer, urinary tract infections, acute anemia, sepsis, pneumonia, acute respiratory failure, myocardial infarction, deep vein thrombosis, pulmonary embolism, cardiac arrest, stroke, and inpatient mortality. Patients were followed for 30 days after discharge to monitor for unplanned readmission. Aggregate hospitalization cost data was obtained from the hospital finance department and subdivided into the following categories: room/board, emergency department (ED), pharmacy, laboratory/pathology, radiology, dialysis, cardiology, procedural, allied health, and other (e.g. blood products).
As appropriate, analysis of variance (ANOVA), independent samples t-, chi-square, and Fisher exact tests were used to determine differences across risk groups and within risk groups on subanalysis with statistical significance set a priori at P < 0.05. All statistical analysis was performed using IBM SPSS Statistics version 26 (IBM Corporation, Armonk, NY).
Results
During the study period, we identified 280 patients who presented to our emergency department and were diagnosed with a proximal or midshaft humerus fracture. One hundred eighty-three patients (65.4%) were treated and discharged directly from the emergency department, while 97 (34.6%) were admitted for further workup and management. Twenty-three patients requiring inpatient care had a concomitant fracture or underwent surgical management for a concomitant injury and were excluded. Therefore, a total of 74/280 patients (26.4%) met final inclusion criteria for this analysis. Distribution of injuries in the cohort included: 58 (78.4%) patients who presented with isolated proximal humerus fractures and 16 (21.6%) who presented with isolated humeral shaft fractures (Figure 1).

Research methodology flow chart.
The mean age of the cohort was 75.0 ± 11.7 years. The majority (73.0%) of injuries occurred secondary to low-energy mechanisms. There were no open fractures. The mean GCS was 14.8 ± 0.7. The mean CCI was 1.4 ± 1.6 with 27 (36.5%) patients having a CCI of 0. The mean AIS subscores were: 0.4 ± 0.9 for AIS-HN, 0.2 ± 0.5 for AIS-Chest, and 2.4 ± 0.6 for AIS-EP. The mean STTGMA score was 3.0 ± 6.5. Using calculated STTGMA scores, 37 (50.0%) patients were classified as minimal risk, 22 (29.7%) were low risk, 11 (14.9%) were moderate risk, and 4 (5.4%) were high risk. 23 Baseline risk group characteristics are further described in Table 1.
Baseline Characteristics by Risk Group.

Abbreviations: GCS, Glasgow Coma Scale; CCI, Charlson Comorbidity Index; AIS-HN, Abbreviated Injury Severity Head & Neck; AIS-Chest, Abbreviated Injury Severity Chest; AIS-EP, Abbreviated Injury Severity Extremity & Pelvis; STTGMA, Score for Trauma Triage in the Geriatric and Middle-Aged.
Bold value denotes statistically significant result at P < 0.05.
The mean LOS for the entire cohort was 5.5 ± 3.4 days with a significant difference across risk groups (P = 0.029). Patients in the minimal risk group had a mean LOS of 4.9 ± 3.2 days, compared with 9.0 ± 3.2 days in the high risk group. The mean number of complications was 0.2 ± 0.5 with no significant difference across risk groups. There were no cases of inpatient mortality. Seventeen (23.0%) patients underwent surgical management of their proximal or midshaft humerus fracture during the index hospitalization with a significant difference in use of surgery across risk groups (P = 0.015). In the minimal risk group, 14 (37.8%) patients underwent operative management while all patients in the high risk group were managed nonoperatively. In the total cohort, 7 (9.5%) patients required ICU/SDU-level care with a marked difference across risk groups (P < 0.001). Three (75.0%) patients in the high risk group required this level of advanced care, compared with 2 (5.4%) patients in the minimal risk group. This difference across risk groups was further seen in the need for post-acute care facilities (e.g. subacute rehabilitation and skilled nursing facility) following discharge (P = 0.001). While 26 (70.3%) minimal risk patients were discharged home, all high risk patients were discharged to post-acute care facilities. The overall unplanned readmission rate within 30 days of discharge was 8.1% with no difference across risk groups (Table 2).
Hospital Quality Measures, Discharge Disposition, and Readmission Rate of Risk Groups.

Abbreviations: LOS, length of stay; ICU, intensive care unit; SDU, step-down unit.
Bold value denotes statistically significant result at P < 0.05.
Subanalysis of risk groups stratified by surgical management demonstrated a significant difference in complications between nonoperative and operative low risk patients (P = 0.008). The mean number of complications for patients in the nonoperative low risk group was 0.1 ± 0.3, compared with 1.0 ± 0.0 in the operative low risk group. There was a significant difference in need for ICU/SDU-level care for nonoperative patients across risk groups (P = 0.001), but no difference between nonoperative and operative patients within any of the same risk groups. There were significant differences in home discharge for nonoperative and operative patients across risk groups (P = 0.020 and P = 0.029, respectively), but no difference between nonoperative and operative patients within any of the same risk groups. All other within group and between group comparisons were noncontributory (Table 3).
Hospital Quality Measures, Discharge Disposition, and Readmission Rate of Risk Groups Stratified by Surgical Management.a

Abbreviations: LOS, length of stay; ICU, intensive care unit; SDU, step-down unit.
a P value* analyzes differences across STTGMA groups. P value† analyzes differences within a specific STTGMA group.
Bold value denotes statistically significant result at P < 0.05.
In the entire cohort, there was no difference in total inpatient cost among risk groups. With respect to subdivisions of care, there were significant differences in room/board (P = 0.013), pharmacy (P = 0.001), and procedural costs (P = 0.034) between risk groups. Compared to the minimal risk group, high risk patients experienced 118.9% higher room/board and 280.3% higher pharmacy costs. While the mean procedural cost was $6575 for the minimal risk group, there were no procedural costs for the high risk group (Table 4).
Index Admission Costs of Care of Risk Groups.

Abbreviations: LOS, length of stay; ICU, intensive care unit; SDU, step-down unit.
Bold value denotes statistically significant result at P < 0.05.
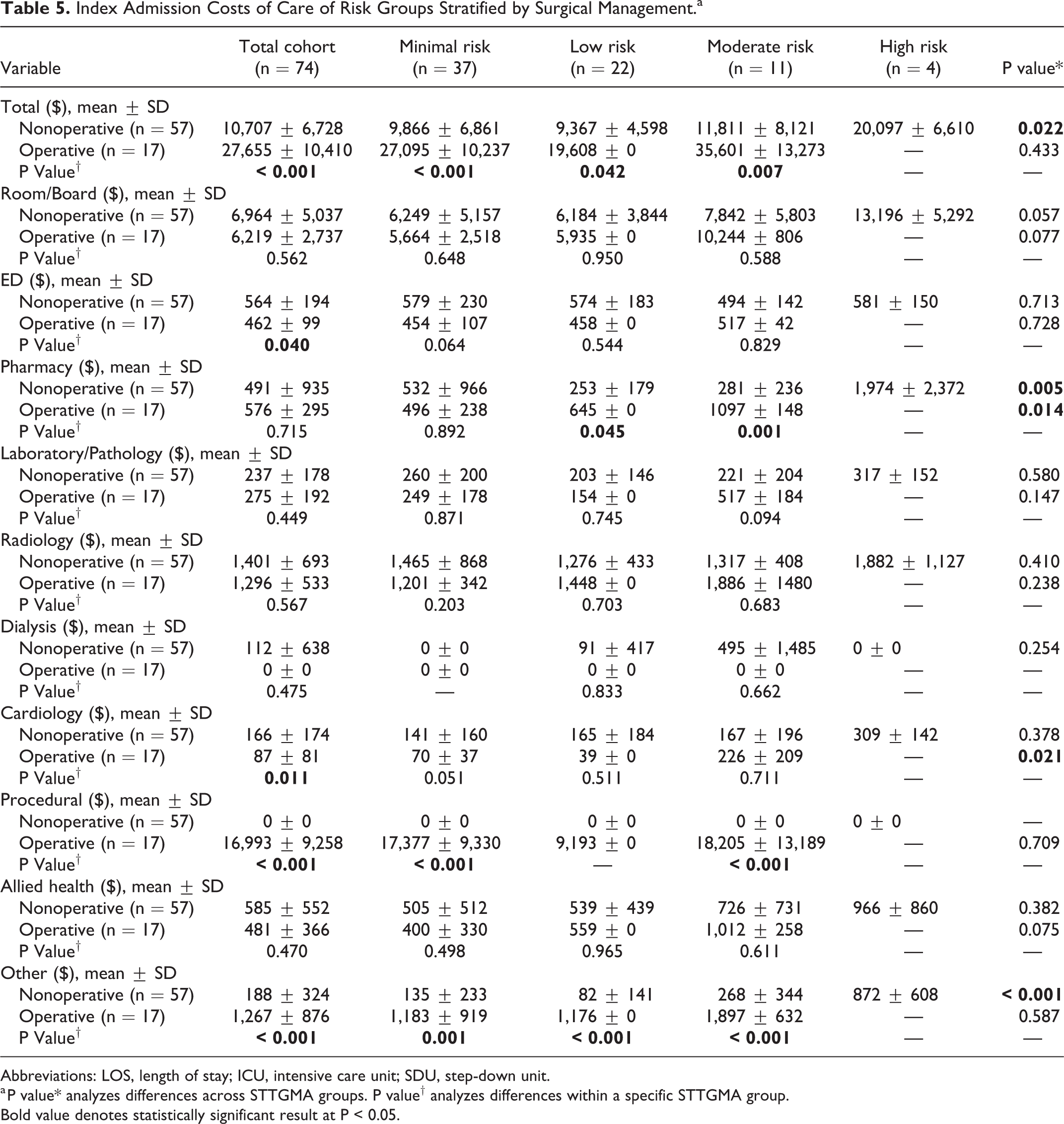
After stratifying risk groups by surgical management, there was a large difference between the total inpatient cost among nonoperative risk groups (P = 0.022). Nonoperative high risk patients experienced 103.7% higher total cost relative to the nonoperative minimal risk group. The mean total inpatient cost difference between operative and nonoperative patients was $16948 (P < 0.001). This difference was significant for all within STTGMA group comparisons, rising from $17229 between minimal risk patients to a difference of $23790 between operative and nonoperative moderate risk patients. Remaining detailed cost differences within and between risk groups are reported in Table 5.
Index Admission Costs of Care of Risk Groups Stratified by Surgical Management.a
Abbreviations: LOS, length of stay; ICU, intensive care unit; SDU, step-down unit.
a P value* analyzes differences across STTGMA groups. P value† analyzes differences within a specific STTGMA group.
Bold value denotes statistically significant result at P < 0.05.
Discussion
In this study, we sought to use a mortality risk stratification tool to predict hospital quality metrics and direct variable costs incurred for patients experiencing proximal and midshaft humerus fractures. Patients with higher STTGMA risk scores experienced longer hospital stays and were more likely to receive nonoperative management. They also had a greater need for ICU/SDU-level care and were less often discharged home compared to patients with lower scores. Additionally, STTGMA stratification demonstrated significant cost differences in room/board, pharmacy, and procedural subdivisions of care across risk groups. After stratifying patients based on surgical management, there were significant differences in need for ICU/SDU-level care and post-acute care facilities following discharge across operative and nonoperative risk groups. Subanalysis further demonstrated within- and across-group differences pertaining to total inpatient cost and the following subdivisions of care: ED, pharmacy, cardiology, procedural, and other (e.g. blood products).
The STTGMA risk prediction tool originated with the goal of real-time use in the emergency department to triage patients experiencing orthopedic trauma. Since its inception, it has demonstrated efficacy in stratifying hospital quality measures (e.g. LOS, ICU/SDU-level care, and complications), discharge disposition, inpatient direct variable costs, and long-term functional outcomes in middle-aged and geriatric patients experiencing orthopedic trauma. 24 -31 Similarly, this tool has demonstrated utility when applied to hip and femur fractures, ankle fractures, and tibial shaft and plateau fractures. 22,23,29 The STTGMA score is calculated using factors determined at the time of presentation to the emergency department including age, medical comorbidities, mechanism of injury, and concomitant injuries and severity. Using these metrics, all of which are typically available at presentation, early decision-making processes can be implemented to tailor care to patients that may be at risk for longer hospital stays with increased complications and greater utilization of post-acute care facilities.
In the aggregate cohort of patients with proximal and midshaft humerus fractures, those with higher STTGMA scores experienced longer lengths of index hospitalization. Given that hospital LOS is a large contributor to cost, it is important to identify factors that influence LOS to both improve patient outcomes and conserve hospital expenses. The LOS outcomes (mean 5.5 days) among all proximal and midshaft humerus fracture patients in our study are consistent with the ranges seen in other analyses. For instance, a recent study identified a mean LOS of 4.5 days for all patients aged 65 and older who sustained an isolated proximal humerus fracture and were admitted at a single level I trauma center. 32 Similarly, a separate study found a mean LOS of 4.4 days for all patients aged 60 and older who presented with isolated proximal humerus fractures and were admitted from the ED at a community-based level I trauma center. 33 Notably, in a large database study of 42511 patients aged 60 and older who were admitted for a proximal humerus fracture, the mean LOS of operatively treated patients was 6.1 days while the mean LOS of nonoperatively treated patients was 7.3 days. 34 Furthermore, a prospective, observation cohort study of humeral midshaft fracture patients found a median LOS of 7.3 days for those treated operatively and a median LOS of 5.2 days for those treated nonoperatively after adjusting for recorded additional injuries and pre-existing medical conditions. 35 Given this, it is important to identify other factors that can be modified to reduce LOS.
Conversely, there was no difference in overall complication rates between STTGMA groups. However, when stratified by treatment (operative vs. nonoperative), patients in the STTGMA low risk group that underwent operative treatment had a significantly higher rate of complications secondary to surgical intervention compared to those that were managed nonoperatively. These findings are similar to those previously described, wherein more in-hospital complications were reported for patients undergoing surgical fixation for proximal humerus fractures than for those treated nonoperatively. 36 Additionally, the complication rate observed throughout the STTGMA strata is consistent with the number of previously reported in-hospital complications occurring in patients with humeral injuries. 36
Moreover, patients with higher STTGMA scores were less likely to undergo operative management. Use of the STTGMA tool for treatment planning with regard to operative and nonoperative management of minimal, low, moderate, and high risk patients is a novel, but important concept. This is the first study to directly compare outcomes in a cohort of both operative and nonoperative patients using the STTGMA tool. Operative treatment of proximal and midshaft humerus injuries has been demonstrated to be equally effective with regard to patient satisfaction measures and longitudinal outcomes when compared to nonoperative treatment. 37 However, up to 40% of complications in operatively treated humerus injuries are related to improper surgical technique. 38 By using the STTGMA tool upon presentation, higher risk patients initially considered as operative candidates may be presented with nonoperative treatment options to avoid unnecessary risk of excess complications and poor outcomes.
Additionally, patients with higher STTGMA scores more frequently required ICU/SDU-level care. Upon further inspection, only patients in the nonoperative group were found to require this advanced level of care. Because the STTGMA score provides a profile of the patient upon presentation, it can be inferred that patients less suitable for surgical candidacy may be at a higher risk for requiring advanced care and should be followed more closely during their hospitalization. ICU/SDU-level care has been associated with an increased need for post-hospitalization resources, readmission, and a reduction in patient-reported quality of life. 39,40 As has been previously demonstrated, the STTGMA tool can predict which patients may require advanced levels of care during their index hospitalization to allow for appropriate preparation and setting of patient and provider expectations. 26
In this study, patients with greater STTGMA scores were also less frequently discharged home and more often required post-acute care following their hospitalization. Discharge to post-acute care facilities is related to poorer outcomes including an increased risk of future complications, readmission, and mortality. 41 -43 Previous reports demonstrate that defined post-acute care pathways can result in lower expenditures and decreased resource use. 44,45 Additionally, providing patients with realistic expectations regarding the course of their care facilitates increased satisfaction after hospitalization. 46 Because the STTGMA tool is able to accurately predict discharge disposition for older patients with proximal and midshaft humerus fractures regardless of treatment intervention, discharge planning can be started early after injury to minimize resource utilization and improve patient satisfaction.
Although readmission after traumatic hospitalization has been associated with discharge location, even after accounting for injury severity and comorbidities, this study found no significant difference in the number of readmissions after hospitalization across STTGMA risk groups. 47 However, after stratifying patients based on operative vs nonoperative management, all patients who required readmission were in the nonoperative cohort. These readmissions were unplanned, and mostly occurred secondary to altered mental status. Additionally, there was no difference between readmission rates across risk groups for the nonoperative cohort. Collectively, these findings may demonstrate that patients who require inpatient care for their proximal or midshaft humerus fracture but are not healthy enough to undergo surgical management are at a higher risk for readmission compared to their surgically treated counterparts.
To ultimately improve value-based care, hospital systems and providers must also understand the principle drivers of inpatient cost. Unfortunately, the direct variable costs associated with proximal and midshaft humerus fractures are not commonly reported. Hasty et al. found that mean Medicare reimbursements for surgically treated proximal humerus fractures ranged from $10368 to $12133. 48 However, these findings are limited because reimbursements are not equivalent to direct variable costs. Additionally, Thorsness et al. used a Medicare claims database to evaluate cost drivers following surgical management of proximal humerus fractures in the Upstate New York area, reporting median in-hospital costs to range from $14967 to $20508. 49 Of note, Thorsness et al. considered in-hospital costs to comprise both initial admission cost and 90-day readmission cost. 49 Moreover, there has been limited investigation of cost implications regarding operative and nonoperative management of humeral shaft fractures. Although one group is conducting a single-center prospective randomized controlled trial to evaluate these parameters, their results have not yet been reported. 50
In the analysis of our entire cohort, room/board was the largest monetary contributor to inpatient care, comprising over 45% of the total index admission cost. This finding corroborates other studies that have described the main contributing factors to inpatient cost for middle-aged and geriatric patients with orthopedic trauma. 22,23 When patients were stratified by operative vs nonoperative management, room/board accounted for appropriately 65% of the inpatient cost for the nonoperative cohort and 22% of the inpatient cost for the operative cohort. Interestingly, after stratifying by treatment type, the percent contribution of room/board to total inpatient cost remained stable across STTGMA risk groups. This finding signifies that as room/board cost steadily increases throughout the hospitalization, there is a parallel rise in other costs of care (e.g. pharmacy, laboratory/pathology, radiology, etc.). Furthermore, patients who underwent surgical treatment accrued significantly higher inpatient costs across all risk groups relative to nonoperatively treated patients. Therefore, establishing baseline expected treatment pathways for proximal and midshaft humerus fracture patients upon admission may allow for early optimizing of factors that greatly contribute to inpatient cost and are prone to overuse. In addition, the creation of risk stratified cost thresholds will allow providers to more accurately determine whether they are over- or undertreating proximal and midshaft humerus fracture patients based on calculated STTGMA scores.
While previous studies have been limited to using claims data as a proxy for cost, a strength of this study includes the use of direct variable cost. 48,49 This information allowed us to precisely identify high utilization areas that we may better target to provide cost-effective care. Yet, despite its strengths, this study still has limitations. The reduced sample size collected over a 4-year period reflects the stringent exclusion of patients under the age of 55 and those who underwent operative management for any concomitant injury. Because of the bimodal distribution of proximal and midshaft humerus fractures with most younger patients experiencing high-energy mechanisms of injury and older patients experiencing low-energy fractures, some patients were excluded secondary to our study’s age requirement. 15,51,52 Additionally, many of the patients who initially presented to our ED where treated without the need for inpatient services, aligning with findings from other previous studies. 33,53 As a result, the sample size was not large enough to detect differences across STTGMA groups that trended toward significance (e.g. LOS and room/board cost) after separating operative from nonoperative patients. Moreover, our findings are only informative regarding individuals treated in an inpatient setting and are not generalizable to the entire population which includes individuals treated on an outpatient basis. Additionally, given the retrospective nature of this study, we were unable to report indications for inpatient admission because they were not consistently specified. Furthermore, since this study took place at an academic medical center, cost data findings may not be consistent with findings at nonacademic institutions. Finally, even though all patients were followed closely throughout hospitalization, it is possible that patients may have sought subsequent care at another institution within the 30-day period following hospitalization, thereby falsely reducing our center’s readmission rate.
Conclusion
In conclusion, the STTGMA tool is able to accurately predict several key hospital quality measures that will allow clinicians to make informed choices in the treatment of proximal and midshaft humerus fracture patients.
Footnotes
Authors’ Note
This study was approved by the Jamaica Hospital Medical Center Institutional Review Board, Queens, NY. Investigation performed at Jamaica Hospital Medical Center, Queens, NY. All conflicts of interest are unrelated to this work. Sanjit Konda, MD, is a paid consultant and receives research support from Stryker. Kenneth Egol, MD, is a committee member of the Orthopaedic Trauma Association, a paid consultant for Exactech, a paid speaker for Smith & Nephew, and receives research support or publishing royalties from Acumed, Synthes, SLACK Incorporated, and Wolters Kluwer.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.