
Abstract
Introduction:
This study sought to investigate whether a validated trauma triage risk assessment tool can predict time to surgery and delay to surgery.
Materials and Methods:
Patients aged 55 and older who were admitted for operative repair or arthroplasty of a hip fracture over a 3-year period at a single academic institution were included. Risk quartiles were constructed using Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA) calculations. Negative binomial and multivariable logistic regression were used to evaluate time to surgery and delay to surgery, respectively. Pairwise comparisons were performed to evaluate 30-day mortality rates and demonstrate the effectiveness of the STTGMA tool in triaging mortality risk.
Results:
Six hundred eleven patients met inclusion criteria with mean age 81.1 ± 10.5 years. Injuries occurred mainly secondary to low-energy mechanisms (97.9%). Median time to surgery (31.9 hours overall) was significantly associated with STTGMA stratification (P = .002). Moderate-risk patients had 33% longer (P = .019) and high-risk patients had 28% longer time to surgery (P = .041) compared to minimal risk patients. Delay to surgery (26.4% overall) was significantly associated with STTGMA stratification (P = .015). Low-risk patients had 2.14× higher odds (P = .009), moderate-risk patients had 2.70× higher odds (P = .001), and high-risk patients had 2.18× higher odds of delay to surgery (P = .009) compared to minimal risk patients. High-risk patients experienced higher 30-day mortality compared to minimal (P < .001), low (P = .046), and moderate-risk patients (P = .046).
Discussion:
Patients in higher STTGMA quartiles encountered longer time to surgery, greater operative delays, and higher 30-day mortality.
Conclusion:
Score for Trauma Triage in the Geriatric and Middle-Aged can quickly identify hip fracture patients at risk for a delay to surgery and may allow treatment teams to optimize surgical timing by proactively targeting these patients.
Level of Evidence:
Prognostic Level III.
Keywords
Introduction
The United States Census Bureau estimates that the geriatric population, aged 65 and over, will almost double from 43.1 million in 2012 to 83.7 million by 2050. 1 Given the incidence of hip fracture rises substantially with age, the developing older adult population translates to a projection that the worldwide number of hip fractures will grow to 6.3 million yearly by 2050. 2,3 Especially in geriatric patients, these injuries are associated with significant risk of morbidity, mortality, loss of independence, and financial burden. 4 -6 Specifically, the relative risk of mortality for hip fracture patients aged 65 and older increases by 4% per year. 7
The standard of care for the vast majority of hip fracture patients is operative fixation. 8 Delays in time to surgery for elderly hip fracture patients are thought to play a primary role in heightening the risk of morbidity and mortality in these vulnerable patients. However, findings are mixed regarding the effects of a delay to surgery and the time point at which patients’ risk of complications, inpatient, 30-day, 90-day, and 1-year mortality begins to increase. 9 -16 Recent studies suggest that each day beyond same-day surgery increases a patient’s overall complication rate. Once surgery is delayed by 2 or more calendar days, mortality rate begins to increase. 10 Therefore, it is crucial to identify patients whose demographics, injuries, and comorbidities may contribute to a delay in time to surgery so that these patients can be placed on an expedited pathway for medical optimization.
The Score for Trauma Triage in the Geriatric and Middle-Aged (STTGMA) is a validated and reliable inpatient mortality risk-stratification algorithm designed to efficiently triage geriatric and middle-aged patients presenting to the emergency department (ED) with trauma-related injuries. 17,18 In addition to predicting inpatient mortality, the STTGMA tool has demonstrated an ability to predict length of stay, inpatient complications, need for intensive or step down unit care, readmission within 30 days, associated cost of care, discharge location, and long-term functional outcomes for geriatric and middle-aged patients with orthopedic trauma injuries. 19 -25 The primary aim of this study was 2-fold (1) to examine the STTGMA tool’s capacity to assess time to surgery for minimal, low-, moderate-, and high-risk hip fracture patients as well as (2) to determine whether the STTGMA tool can be used to identify hip fracture patients at high risk of experiencing a delay to surgery following inpatient admission and assign them to an expedited pathway for medical optimization.
Materials and Methods
Patient Selection
Between October 2014 and September 2017, all patients aged 55 and older who presented to our academic institution (2 level 1 trauma centers, 1 orthopedic specialty hospital, and 1 university based tertiary care referral center) after sustaining a hip fracture that required inpatient admission and subsequent operative fixation were enrolled in a prospective institutional review board–approved database. Hip fracture was defined as fracture involving the femoral neck, trochanteric region, or subtrochanteric region of the femur. Patients who expired prior to operative fixation were excluded from this study.
Independent Variables
Upon initial ED evaluation at our academic institution, all patients aged 55 and older with fracture injuries secondary to nonpenetrating trauma are assigned a STTGMA score following an orthopedic consultation. The STTGMA score algorithm takes into account the following variables: patient age, Charlson Comorbidity Index (CCI), Glasgow Coma Scale (GCS) on initial evaluation, mechanism of injury, as well as Abbreviated Injury Severity Subscores for the Head & Neck (AIS-HN), Chest (AIS-Chest), and Extremities & Pelvis (AIS-EP). Mechanisms of injury are categorized as low and high energy. Low-energy mechanisms of injury include all falls from standing height or ≤2 stairs. High-energy mechanisms of injury include all falls >2 stairs, motor vehicle accidents, motorcycle accidents, or pedestrians struck by vehicles.
Score for Trauma Triage in the Geriatric and Middle-Aged scores are calculated on a scale of 0% to 100%, with higher scores denoting greater risk of inpatient mortality during the index hospitalization. 18 Orthopedic surgical residents are educated on how to properly compute STTGMA scores using an online education module and publicly available internet-based STTGMA calculator (https://sttgma.wordpress.com/about/). The primary independent variable in this study was STTGMA trauma triage risk score. Based on calculated STTGMA scores, patients were stratified into quartiles to create minimal, low-, moderate-, and high-risk trauma triage groups ranging from <0.87%, 0.87% to 1.39%, 1.39% to 2.15%, and >2.15%, respectively.
In addition to STTGMA variables, the following patient information was collected and analyzed: sex, race, insurance status, anticoagulant use, and type of hip fracture. The procedural variable type of surgery, year of hospital admission, and day of hospital admission (weekday vs weekend) were also documented and evaluated.
Dependent Variables
Patients were followed throughout hospitalization, and the primary dependent variable was time to surgery measured in hours. A delay to surgery was defined as operative fixation occurring later than 48 hours from time of admission. A secondary dependent variable was mortality within 30 days.
Statistical Analysis
After stratifying patients into trauma triage risk groups, 1-way analysis of variance, χ2, and Fisher exact tests were used, as appropriate, to identify baseline differences between risk cohorts. Time to surgery data were found to be non-normal with a right-skewed distribution (Figure 1). Therefore, median time to surgery was calculated overall and for each independent variable: trauma triage risk group, sex, race, insurance status, anticoagulant use, type of hip fracture, type of surgery, year of hospital admission, and day of hospital admission (weekday vs weekend). Bivariate analyses between time to surgery and each independent variable utilized Mann-Whitney U and Kruskal-Wallis tests, as appropriate, for nonparametric analysis. A Dunn test with Bonferroni corrections implemented for multiple comparisons was used to identify post hoc differences between trauma triage groups and time to surgery. Delay to surgery was analyzed as a binary variable, and bivariate analyses utilized χ2 tests to identify factors impacting delay to surgery.

Boxplot of time to surgery with respect to trauma triage risk group. Multiple post hoc comparisons with Bonferroni corrections demonstrated that time to surgery for patients in the moderate-risk and high-risk groups was significantly higher than for patients in the minimal risk group. Circle symbols (ˆ) indicate outliers in the data. *P < .05, **P < .01.
Negative binomial regression was subsequently performed in a multivariable approach to control for confounding factors and determine the adjusted association between trauma triage groups and time to surgery. Negative binomial models are used to assess skewed outcome variables and have been effectively implemented in prior studies analyzing length of stay following orthopedic surgery. 26,27 In addition, according to Carter and Potts, the negative binomial regression modeling technique can be used for predicting other outcome variables, besides length of stay, when the distribution of data is skewed. 28 Meanwhile, multivariable logistic regression was used to control for confounding variables and investigate the adjusted effect of trauma triage groups on delay to surgery. All multivariable analyses utilized forward variable selection with threshold for entry set at P < .1 for baseline characteristics associated with time to surgery and delay to surgery. A comparison of 30-day mortality rates across all trauma triage risk groups was performed using a Fisher exact test with subsequent pairwise comparisons carried out using χ2 and Fisher exact tests, as appropriate. Statistical analyses were performed using IBM SPSS Statistics version 25 (IBM Corporation) and RStudio version 1.2.5019 (RStudio Incorporated) with a significance level set a priori at P < .05.
Results
Descriptive Statistics
In total, 611 patients underwent hip fracture surgery and met inclusion criteria (152 or 153 per STTGMA risk quartile). Mean age of the entire sample was 81.1 ± 10.5 years with 598 (97.9%) patient injuries occurring secondary to low-energy mechanisms and 13 (2.1%) patient injuries occurring secondary to high-energy mechanisms. Most patients had CCI scores <2 (65.3%), GCS evaluations of 15 (94.3%), and AIS classifications of 0 for AIS-HN (96.9%) and AIS-Chest (98.0%). An AIS classification of 3 (98.2%) was most common for AIS-EP. Incorporating these characteristics, the mean STTGMA score was 1.8 ± 1.4%. Baseline STTGMA variables stratified by risk group are presented in Table 1.
STTGMA Variables Stratified by Trauma Triage Risk Group.
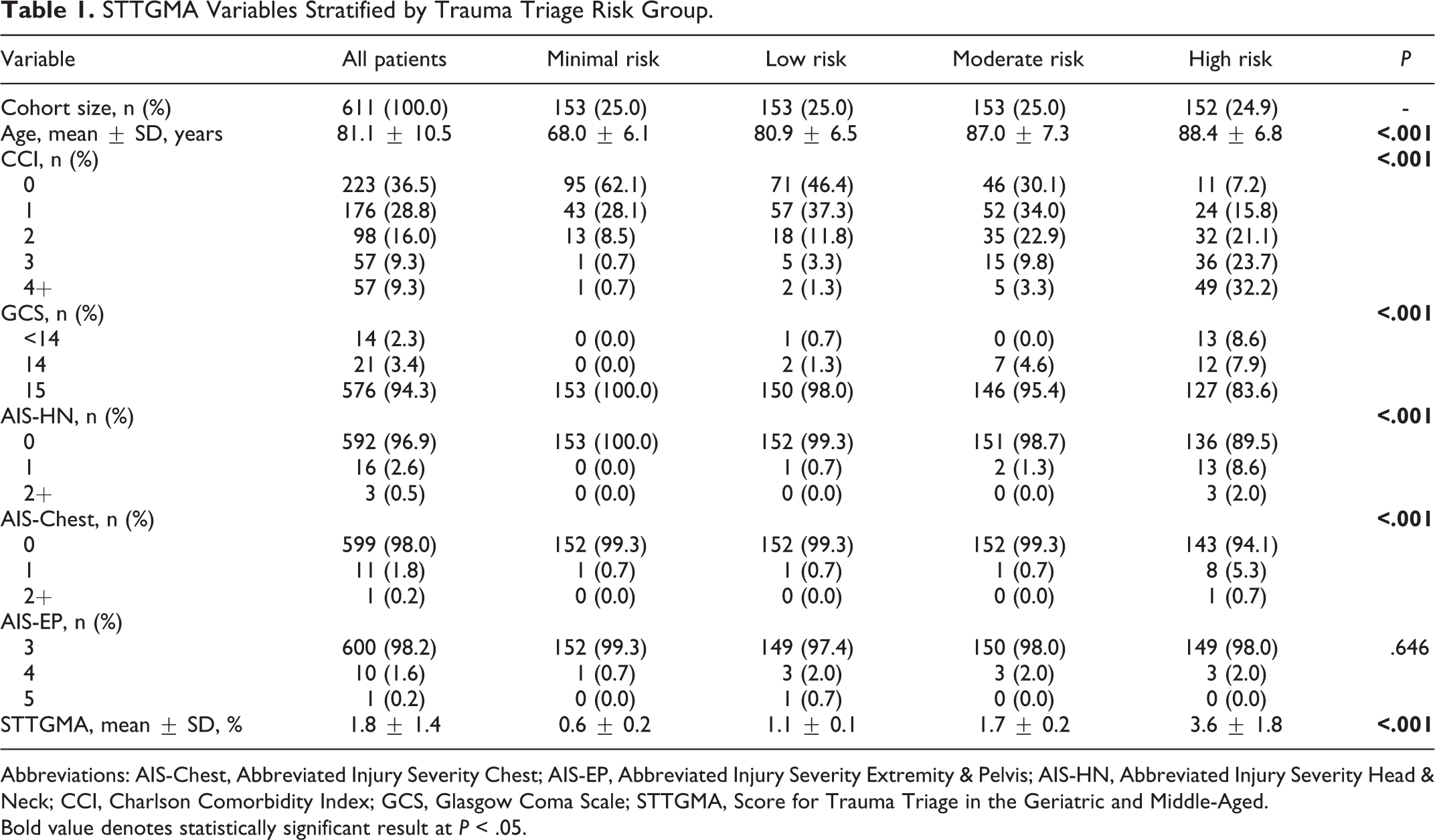
Abbreviations: AIS-Chest, Abbreviated Injury Severity Chest; AIS-EP, Abbreviated Injury Severity Extremity & Pelvis; AIS-HN, Abbreviated Injury Severity Head & Neck; CCI, Charlson Comorbidity Index; GCS, Glasgow Coma Scale; STTGMA, Score for Trauma Triage in the Geriatric and Middle-Aged.
Bold value denotes statistically significant result at P < .05.
Furthermore, the majority of patients in this study were female (70.9%) and of Caucasian descent (69.9%). Most patients possessed Medicare insurance (61.5%) and were not on anticoagulant medication prior to hospitalization (63.3%). Intertrochanteric fractures (51.2%) and femoral neck fractures (42.1%) accounted for the highest percentage of patient cases with only a small fraction of patients sustaining subtrochanteric fractures (6.7%). Open reduction and internal fixation was the most frequently used operative repair technique (64.3%), and most patients presented to our academic institution on a weekday (67.8%). Non-STTGMA patient variables stratified by risk group are displayed in Table 2.
Other Patient Characteristics Stratified by Trauma Triage Risk Group.

Abbreviation: ORIF, open reduction and internal fixation.
Bold value denotes statistically significant result at P < .05.
Time to Surgery
Median time to surgery for all patients was 31.9 hours (interquartile range [IQR]: 21.9-48.7 hours). An unadjusted bivariate comparison demonstrated significant differences in time to surgery when stratified by trauma triage risk group (P = .002) with minimal risk patients experiencing the shortest median time to surgery (26.3 hours, IQR: 18.3-41.0 hours) and high-risk patients experiencing the longest median time to surgery (35.2 hours, IQR: 24.0-48.6 hours). Post hoc comparisons between trauma triage risk groups demonstrated that time to surgery for patients in the moderate-risk and high-risk groups was significantly longer than for patients in the minimal risk group (P = .013 and P = .002, respectively; Figure 1). Further unadjusted bivariate comparisons identified sex (P = .012), anticoagulant use (P = .001), and type of surgery (P = .011) as other variables that were significantly associated with time to surgery. All other baseline patient characteristics were nonsignificant influencers of time to surgery (all P > .05). Unadjusted bivariate analyses between baseline patient characteristics and time to surgery are shown in Table 3.
Bivariate Analysis Between Baseline Patient Characteristics and Time to Surgery.

Abbreviation: ORIF, open reduction and internal fixation.
a Variable selected for negative binomial regression analysis based on statistical significance.
Bold value denotes statistically significant result at P < .05.
In negative binomial regression, patients in the moderate risk group had 33% longer time to surgery (incidence rate ratio [IRR]: 1.33, 95% CI: 1.05-1.69, P = .019) and patients in the high-risk group had 28% longer time to surgery (IRR: 1.28, CI: 1.01-1.63, P = .041) compared to patients in the minimal risk group. There were no other significant predictive factors in negative binomial regression (all P > .05; Table 4).
Negative Binomial Regression Analysis for Time to Surgery.
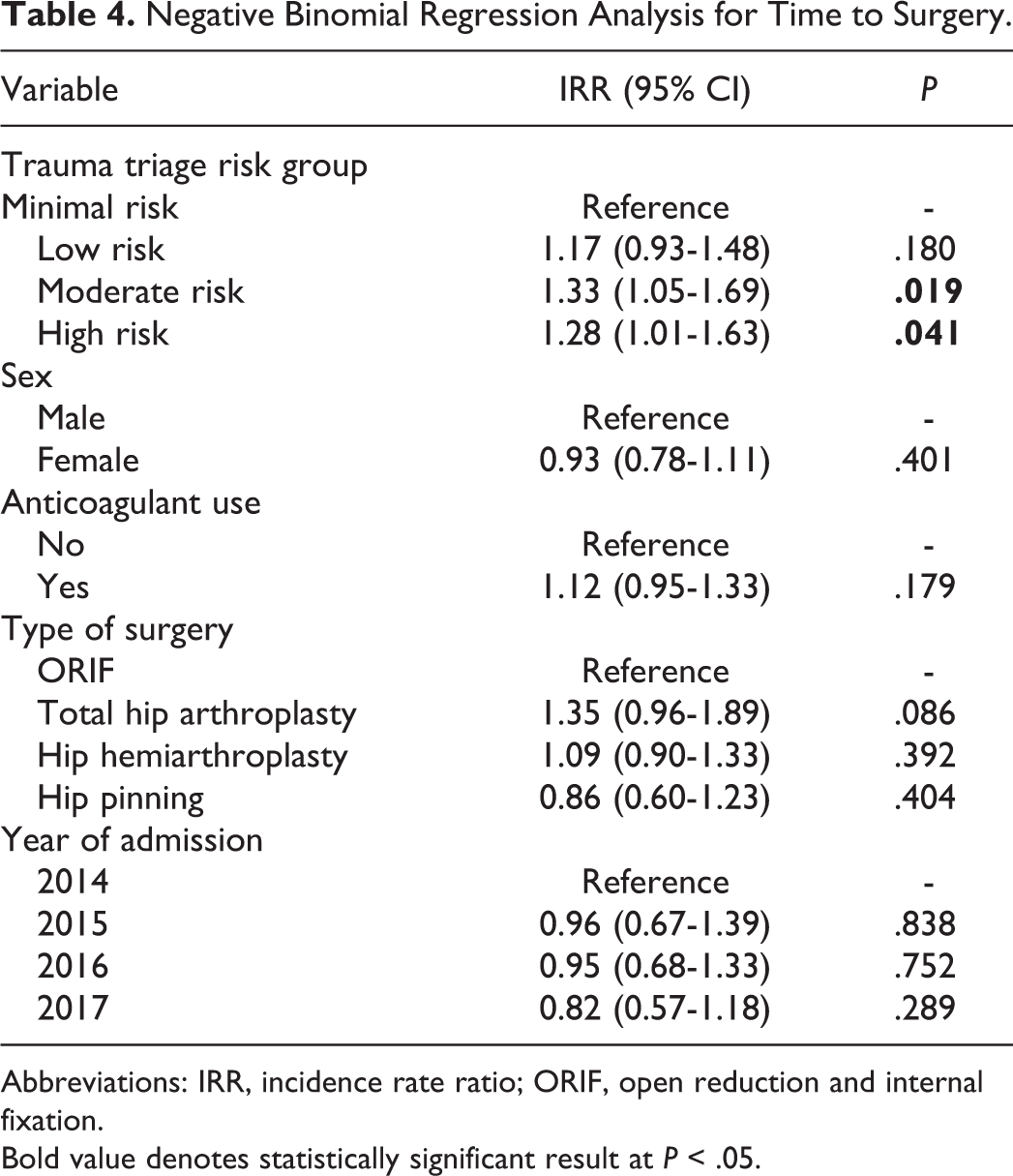
Abbreviations: IRR, incidence rate ratio; ORIF, open reduction and internal fixation.
Bold value denotes statistically significant result at P < .05.
Delay to Surgery
Overall delay to surgery rate was 26.4%. An unadjusted bivariate comparison demonstrated that trauma triage risk profiling was significantly associated with delay to surgery (P = .015) with 17.0% of minimal risk patients experiencing a delay to surgery and over 27% of low-, moderate-, and high-risk patients experiencing a delay to surgery. Sex (P = .041) and type of surgery (P = .011) were also associated with delay to surgery, but the distribution of delay to surgery was similar for all other patient characteristics (all P > .05; Table 5).
Bivariate Analysis Between Baseline Patient Characteristics and Delay to Surgery.

Abbreviations: ORIF, open reduction and internal fixation.
a Variable selected for multivariable logistic regression analysis based on statistical significance.
Bold value denotes statistically significant result at P < .05.
Multivariable logistic regression demonstrated that low-risk patients had 2.14× higher odds (odds ratio [OR]: 2.14, CI: 1.21-3.80, P = .009), moderate-risk patients had 2.70× higher odds (OR: 2.70, CI: 1.52-4.80, P = .001), and high-risk patients had 2.18× higher odds of delay to surgery (OR: 2.18, CI: 1.21-3.92, P = .009) compared to minimal risk patients. Total hip arthroplasty was also a significant predictor of delay to surgery (OR: 2.70, CI: 1.32-5.51, P = .007) compared to open reduction and internal fixation with sliding hip screws or cephalomedullary nails for operative management of hip fracture patients (Table 6).
Multivariable Logistic Regression Analysis for Delay to Surgery.
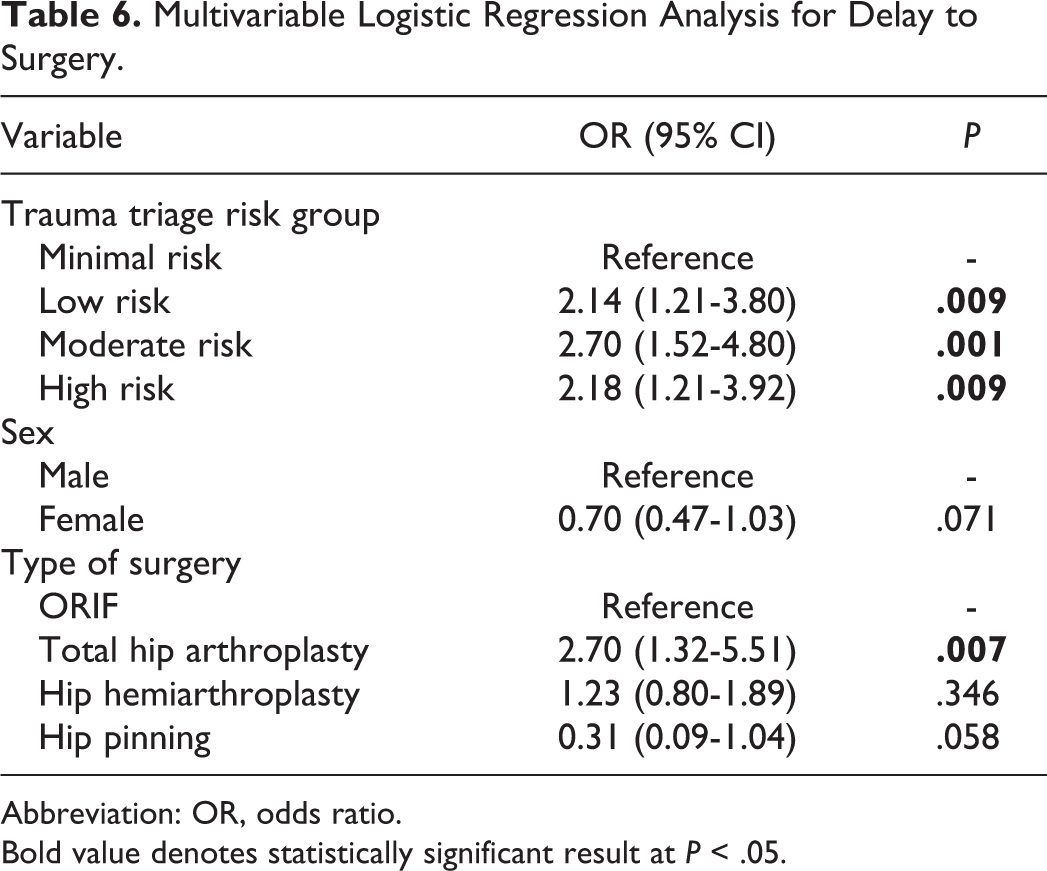
Abbreviation: OR, odds ratio.
Bold value denotes statistically significant result at P < .05.
Thirty-Day Mortality
Overall mortality within 30 days was 2.6%. The 30-day mortality rate for each trauma triage quartile was 0.0% for minimal, 2.0% for low, 2.0% for moderate, and 6.6% for high-risk patients. There was a significant association between mortality within 30 days and trauma triage risk profiling (P = .003). Further pairwise comparisons demonstrated that high-risk patients experienced significantly higher mortality within 30 days compared to minimal (P < .001), low (P = .046), and moderate-risk patients (P = .046; Figure 2).
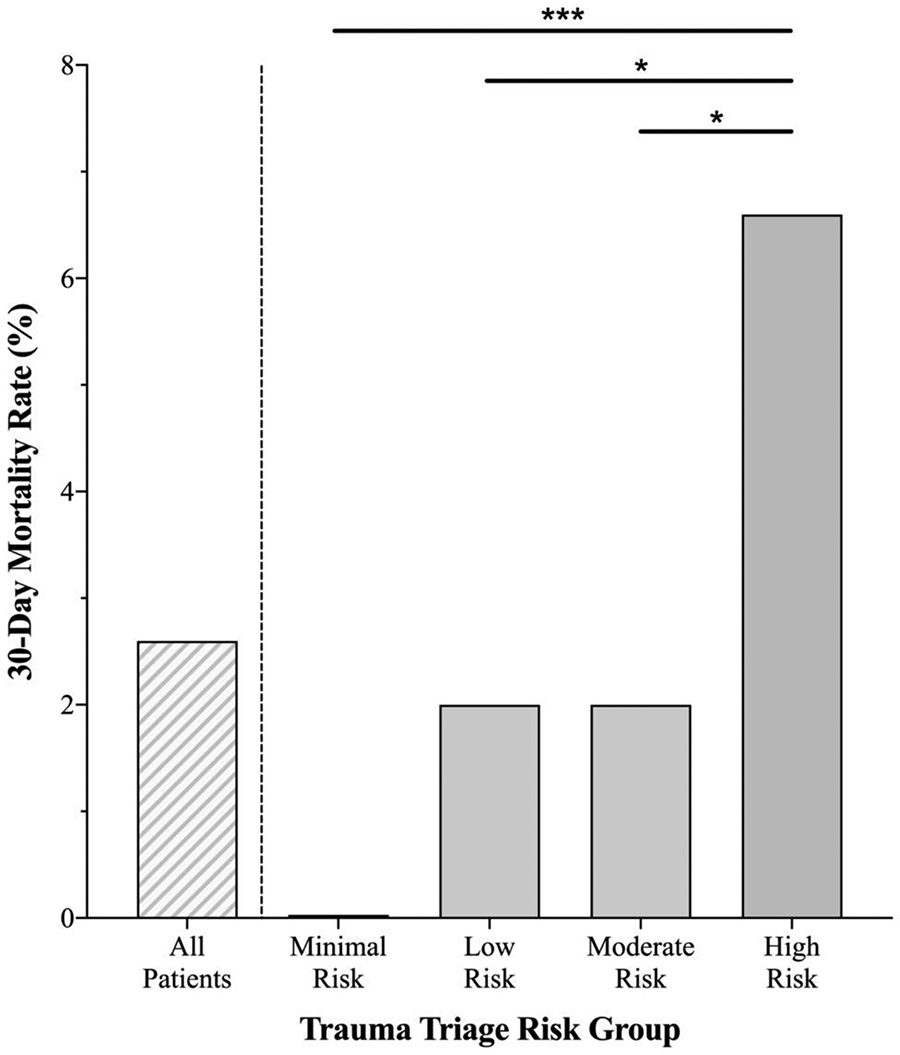
Thirty-day morality stratified by trauma triage risk group. Multiple pairwise comparisons demonstrated significant differences between risk groups. *P < .05, ***P < .001.
Discussion
This study highlights that risk profiling geriatric and middle-aged hip fracture patients in the ED setting using the STTGMA tool is a quick and effective method to assess expected time to surgery and predict which patients may experience over a 48-hour delay to surgery following inpatient admission. Notably, the STTGMA tool showed that moderate-risk and high-risk patients experienced 33% and 28% longer times to surgery than minimal risk patients, respectfully. In addition, the adjusted odds of delay to surgery were 2.14× higher for low-risk patients and were even higher for moderate-risk and high-risk patients (2.70× and 2.18×, respectively) when compared with minimal risk patients. Additionally, the STTGMA tool demonstrated a robust ability to predict 30-day mortality following hip fracture with 6.6% of high-risk patients expiring within 30 days compared to 0.0% of patients in the minimal risk group.
A prior nationwide study using the National Inpatient Sample evaluated the morbidity and mortality associated with delays in time to surgery for hip fracture patients and defined a “delay” as operative fixation performed 2 or more days following admission for a hip fracture. 10 The study found no significant difference in inpatient mortality between patients who underwent same-day surgery versus next-day surgery. However, the odds of inpatient mortality were significantly increased in patients who had surgery >2 days after admission, underscoring our study’s definition of a delay to surgery being >48 hours from admission.
Given the established definition of delay to surgery for hip fracture patients, the collective results from our study demonstrate that STTGMA is a clinically meaningful tool. We report the statistically significant trend that time to surgery increases based on higher STTGMA risk quartiles (Table 4, Figure 1). Moreover, these increases in time to surgery based on STTGMA risk quartiles are relevant beyond simply being statistically significant because they resulted in higher proportions of patients experiencing a clinically defined delay to surgery >48 hours (Table 6). Together, these complimentary findings create a framework in which STTGMA predicts pertinent increases in time to surgery. This information may be useful for early identification of hip fracture patients who are at risk for a significant delay in time to surgery so that treating physicians can more proficiently utilize resources and streamline care.
It has been repeatedly reported that early surgical intervention for hip fracture patients leads to decreased inpatient, 30-day, and 1-year mortality. 16,29,30 However, an ongoing area of research involves different strategies to circumvent hip fracture morbidity by identifying the individuals at greatest risk of poor outcomes following delay to surgery. For instance, along with fracture-related blood loss, frail patients may present with malnutrition and hypotension exacerbated by diuretics and other antihypertensive medications. Therefore, active avoidance of postoperative hypotension may reduce risk of cardiac-related complications and delirium. 31 Early recovery of mobilization, including a shorter time between operation and first mobilization, has also been associated with lower in-hospital mortality and complications following hip fracture surgery. 32 In accordance with this notion, our trauma center emphasizes early mobility and rehabilitation for orthopedic trauma patients, especially following hip fracture repair. Aligning with another study that advocates for avoidance of “as needed” (PRN) consults in favor of consistently scheduled consults, our trauma center has implemented a palliative care program aimed toward all higher risk orthopedic patients. 33 As part of this program, it is our standard of care for any patient with a STTGMA score ≥1.0% to automatically receive a palliative care consult to establish goals of care. This consult is obtained within the first 72 hours of admission, either pre- or postoperatively and is designed to guide both inpatient and postdischarge care by optimizing interventions based on patient/family wishes. Future studies will be necessary to determine the impact that this established program has on improving patient outcomes for the hip fracture population.
Collectively, there is limited up-to-date research attempting to triage patients into risk groups based on anticipated delay to surgery, which presents the novel opportunity for the STTGMA tool to be utilized upon admission to identify high-risk hip fracture patients. Interestingly, after performing negative binomial and multivariable analyses in our study, many previously identified risk factors for increased time to surgery or delay to surgery in hip fracture patients were found to be nonsignificant (sex, race, insurance, anticoagulant use, type of hip fracture, and day of admission). For instance, men have previously been found to have increased time to surgery compared to women following hip fracture, possibly secondary to men requiring higher degrees of medical stabilization before surgery. 34 Additionally, another study found that race and insurance-based disparities exist in delivery of care for hip fracture patients with delay to surgery risk increasing for black and Asian patients compared to white patients as well as Medicaid patients compared to Medicare patients. 35 Furthermore, there is concern regarding increased risk of surgical bleeding due to anticoagualant therapy at time of admission, and other investigators found anticoagulant therapy to be a risk factor for increased delay to surgery following hip fracture. 36,37 In addition, another group found that patients who sustained intertrochanteric or subtrochanteric fractures were at lower risk of missing the United Kingdom’s National Institute for Health and Care Excellence time-to-hip-fracture-surgery benchmark compared to patients who sustained femoral neck fractures. 38 Other investigators have also found that weekend admissions tend to have longer time to surgery, secondary to fewer resources being available on weekends than on weekdays. 34,36 Conversely, our current study did find that patients treated surgically with total hip arthroplasty did experience higher odds of experiencing a delay to surgery relative to patients treated with open reduction and internal fixation with sliding hip screw devices or cephalomedullary nails. This finding aligns with a previous study regarding time to surgery for hip fracture patients and may be due to the limited availability of an on-call surgeon experienced in total hip arthroplasty or arthroplasty implants not being readily available for use. 39
One possibility for why our study failed to find an association between most previously studied risk factors and time to surgery or delay to surgery following hip fracture may be that our patient sample was derived from a single academic institution rather than from a large-scale national database. Given that statistical power is positively correlated with sample size, large database studies allow for greater sample size selection and therefore higher statistical power. 40 Higher statistical power translates to a lower probability of making a type II error (false negative), allowing large database studies to uncover significant predictive factors that may go undetected in a single institutional study. However, large database studies often require a subset of patients to be omitted from analysis due to missing data, which can result in selection bias and limit the extent to which findings may be relevant in clinical practice.
Additionally, there may be significant confounding from a variety of other patient and hospital variables that were not collected as a part of this study. For instance, there is diurnal variation in rates of hip fracture presentation and the timing of presentation has been shown to have a marked effect on surgical delays. 41 We also did not report preinjury ambulatory status or metrics of frailty in this study. However, a previous study by Konda et al demonstrated no further improvement in the predictive ability of the STTGMA tool following the addition of these factors into the model: preinjury ambulatory status, serum albumin level (surrogate for long-term nutritional status), use of a gait assistive device, and preinjury anticoagulation status. 18
Given that STTGMA accounts for nonmodifiable factors (eg, age, CCI, injury severity), the current study does not heavily focus on resource availability factors that can be modified, aside from type of surgery. However, it does demonstrates a novel method of identifying high-risk patients who can be quickly targeted to reduce time to surgical readiness, which may facilitate improved outcomes by decreasing time to surgery and the proportion of high-risk patients experiencing a delay to surgery following hip fracture. Notably, while there was an apparent dose–response in time to surgery and 30-day mortality across STTGMA risk quartiles, the elevated risk of delay to surgery plateaued for the highest STTGMA quartile. This finding may demonstrate that providers internally recognize extremely high-risk patients which heightens their awareness to preferentially optimize these patients for surgery, thereby attenuating operative delays. This proposal is consistent with the reduced variance in time to surgery for the upper quartile of high-risk patients compared to the upper quartile of moderate-risk patients (Figure 1).
Although the STTGMA tool was originally designed for all trauma patients, it has been extensively utilized to study perioperative outcomes in the hip fracture population, reinforcing its reliability and potential for improving patient workflow and hospital quality measures pertaining to hip fracture outcomes. 20,23 Previously, the STTGMA score has been used in the early identification of high-risk geriatric and middle-aged trauma patients for resource-sparing interventions, including palliative care consultation referral. This identification model demonstrated that using STTGMA to identify high-risk palliative care patients could produce over US$1 million in net hospital savings per year. 17 Therefore, given its high cost-saving potential, the STTGMA tool may be used to flag hip fracture patients who are at high risk of a delay to surgery, which would likely improve patient outcomes as well as provide a cost-saving intervention for hospitals everywhere.
Conclusion
The STTGMA tool allows for rapid assessment of geriatric and middle-aged hip fracture patients and has a demonstrated ability to predict expected time to surgery and operative delays. Using this tool may allow treatment teams to proactively triage “at risk” patients which would likely improve patient outcomes and hospital quality measures.
Footnotes
Authors’ Note
This research was presented as a podium presentation at the International Geriatric Fracture Society Annual Meeting, Denver, Colorado, September 2019 and as a poster presentation at the Annual Meeting of the Orthopaedic Trauma Association, Denver, Colorado, September 2019. This study was approved by the NYU School of Medicine Institutional Review Board and the Jamaica Hospital Medical Center Institutional Review Board. Investigation performed at NYU Langone Medical Center, New York, NY; Jamaica Hospital Medical Center, Queens, NY; NYU Langone Hospital—Brooklyn, Brooklyn, NY.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.R.K. is a paid consultant and receives research support from Stryker. T.L. is a paid consultant for Acumed and receives IP royalties from Arthrex. K.A.E. is a committee member of the Orthopaedic Trauma Association, a paid consultant for Exactech, a paid speaker for Smith & Nephew, and receives research support or publishing royalties from Acumed, Synthes, SLACK Incorporated, and Lippincott Williams & Wilkins.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.