
Abstract
Introduction:
Despite the recommendation for postoperative orthopedic follow-up after a hip fracture in elderly patients, many patients do not return for these visits. In this study, we attempt to determine if early follow-up (<4 weeks post-discharge) changes orthopedic post-operative management.
Materials and. Methods:
1232 patients aged
Results:
417 patients (33.8%) patients did not return for any follow-up and 30 (2.4%) patients died <30 days from discharge. 370 (45.5%) patients had early orthopedic follow-up ≤28 days after discharge. 317 (38.9%) patients were seen ≥29 days after discharge (late follow-up). 127 (15.6%) patients returned for isolated non-orthopedic care. There were 23 (6.2%) readmissions in the early group, 17 (5.4%) in the late group, and 24 (18.9%) in the no follow-up group (p < 0.001). Patients discharged home were more likely to present for early follow-up compared to those with late and non-orthopedic follow-up (p = 0.002), however there was no difference in readmission rates between those discharged home vs. SNFs/SARs.
Discussion:
Patients who received isolated non-orthopedic follow-up within 4 weeks of surgery experienced more hospital readmissions than those with follow-up in that time period; however, these readmissions were primarily due to medical issues. There was no difference in orthopedic-related readmissions and changes in orthopedic management between groups. Patients discharged to SNFs/SARs did not present for early orthopedic as often as those discharged home.
Conclusion:
Early orthopedic follow up after hip fracture care does not change post-operative management in these patients and has implications for value-based care.
Level of Evidence:
Prognostic Level III.
Keywords
Introduction
Hip fractures are a known cause of morbidity, mortality, and cost in the geriatric population. The United States spends nearly $3 billion USD for hip fracture care, and this cost is expected to rise with an increase in the geriatric population. 1,2 As we encounter increasing frailty in patients, there is an associated rise in cost of care. 3,4 Furthermore, hip fracture patients are more likely to be discharged to a subacute rehabilitation center, especially when they are considered high risk or high frailty, which in turn further increases costs associated with their care. 5
Previous studies have demonstrated that routine radiographs following fracture surgery in the early post-operative period do not change management. 6 -9 Thus, the remaining potential purposes of early post-operative follow-up of these patients may be to evaluate incisions, remove sutures, and screen for and mitigate orthopedic complications.
Appropriate patient follow-up after surgery can often be challenging for certain patient populations, whether discharged home or to a post-acute care facility such as a subacute rehabilitation center (SAR) or skilled nursing facility (SNF). In the early post-operative period, transportation to clinic for routine follow-up may be more challenging in this patient population to include the need for medical transportation. For those at SAR or SNF, early follow-up requires inter-facility transportation that may even involve prolonged immobilization on a stretcher. The purpose of this study is to determine if the early (<4 week) post-operative care following discharge for hip fracture fixation or arthroplasty impacts readmission rates or changes orthopedic management.
Materials and Methods
Over a 4 year period, patients aged 55 years or older who were admitted with a femoral neck, intertrochanteric, or subtrochanteric hip fracture (AO/OTA fracture classification of 31A; 31B; and 32(A, B, C).1) were enrolled prospectively in a IRB-approved trauma registry and followed from hospitalization through one year. Demographics, patient comorbidities (measured by the Charlson Comorbidity Index), injury severity (measured by Glasgow Coma Scale and Abbreviated Injury Scale subscores including head, chest, and extremity/pelvis), and patient functional status (including use of assistive devices, ambulatory capacity, and independence in activities of daily living) were collected. Individual charts were reviewed and follow-up points were identified. Patients were grouped into either the early follow-up <28 days or in the late follow-up (>28 days) groups. Discharge destinations were recorded and 30-day readmission data was also obtained. All patients who were discharged, whether they went to a SAR or home, were given a “routine postoperative” appointment in their discharge paperwork for follow-up at 2-3 weeks. All complications were recorded. Statistical analyses including chi-square, independent-samples t-tests, and analysis of variance (ANOVA) were performed using IBM SPSS Statistics software, version 25.0 (Armonk, NY).
Results
1232 patients with either a femoral neck, intertrochanteric, or subtrochanteric hip fracture met inclusion criteria. Of these patients, 491(39.8%) had femoral neck fractures, 663 (53.9%) had intertrochanteric fractures and 78 (6.3%) had subtrochanteric fractures (Table 1).
Demographic Characteristics by Follow-up Group.

418 patients (33.9%) patients did not return for any follow-up and 30 (2.4%) patients died <30 days from discharge. 370 (45.5%) patients had early orthopedic follow-up ≤28 days after discharge. 317 (38.9%) patients were seen ≥29 days postoperatively (late follow-up). Of note, 127 (15.6%) patients returned for isolated non-orthopedic care to either a primary care or a medical specialty appointment (mean time to follow-up 50.0 ± 40.3 days).
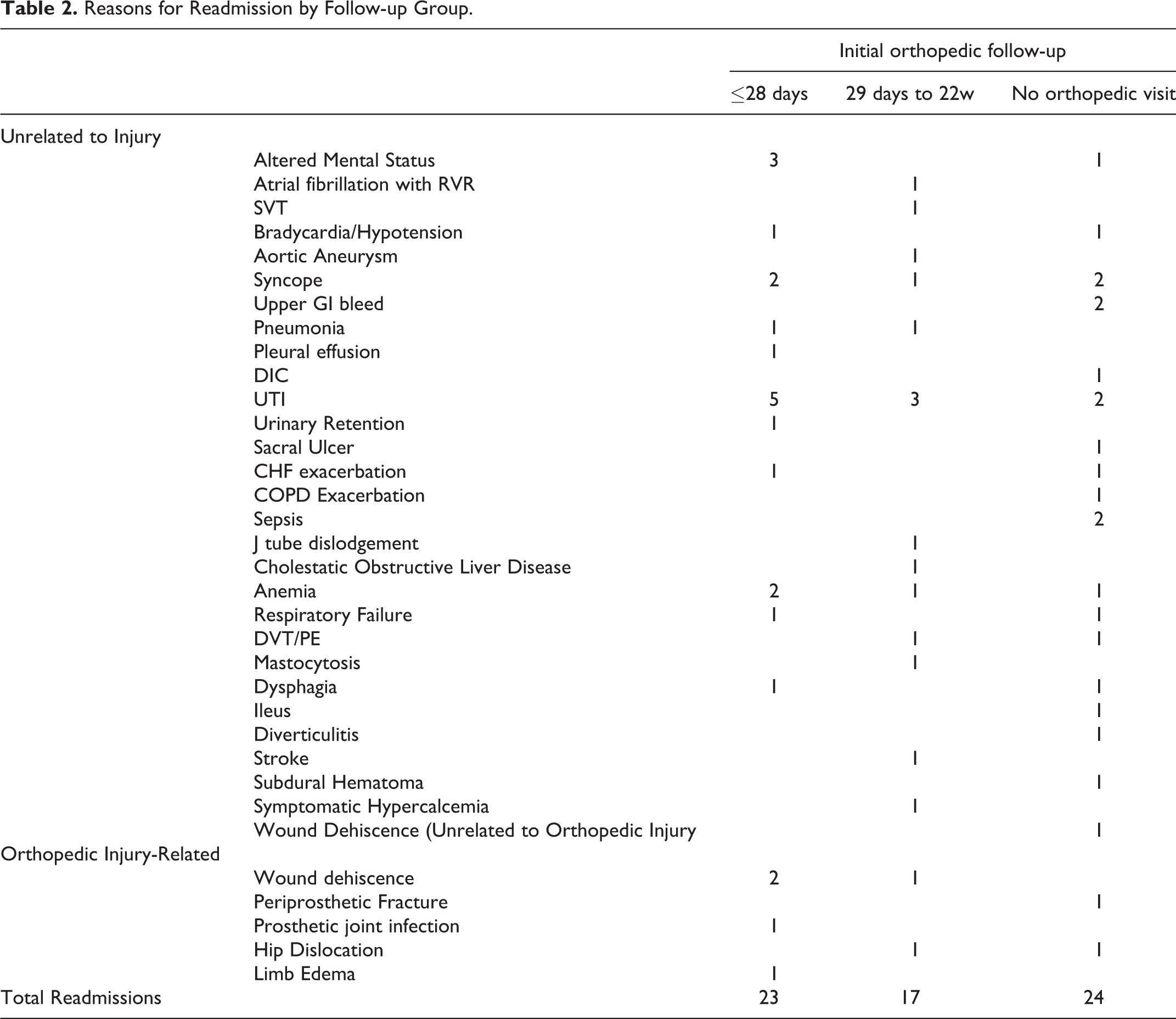
There were 23 (6.2%) readmissions in the early follow-up group, 17 (5.4%) in the late follow-up group, and 24 (18.9%) in the non-orthopedic follow-up group (p < 0.001). There were no differences in follow-up or readmissions when stratified by fracture classification. Of the 64 readmissions observed in this study, 8 (12.5%) were related to the patient’s orthopedic injury; the remainder were due to medical related issues (Table 2). Orthopaedic related complications were very low and did not seem to differ by group. Patients who were discharged home were more likely to present for early follow-up compared to those with late and no orthopedic follow-up (31.4% vs. 19.9% vs. 22.8%, respectively, p = 0.002), however there was no difference in readmission rates between those discharged home vs. SAR/SNF (7.7% vs 7.9%, p = 0.916).
Reasons for Readmission by Follow-up Group.
A binomial logistic regression to determine the effects of age, CCI, discharge location, and follow-up group on readmission was performed. The model was statistically significant (p < 0.001). The variables of CCI and follow-up group were associated; each increase in CCI increased likelihood of readmission by a factor of 1.3 (p = 0.001) and patients that received isolated non-orthopedic follow-up were 1.7 times more likely to be readmitted (p = 0.002).
Discussion
The study results demonstrate that hip fracture follow-up is highly variable, and our loss of follow-up (33.9%) is consistent with what is reported within the literature. 10,11 The medical aspect of hip fracture care was shown to have a higher impact on readmissions than orthopedic-related issues. Kuoriokosi and Soderlund demonstrated that routine follow-up after proximal femur fractures within the first 10 weeks postoperatively does not change management from an orthopedic standpoint. 11 The authors suggested that patients with postoperative issues (e.g. postoperative infection) would seek an appointment prior to their routine scheduled follow-up and this occurred in about 3% of their patients.
Similarly, Halonen et al. demonstrated that within their cohort of 200 intertrochanteric hip fractures, there was a 0.9% change in treatment at a planned outpatient visit due to orthopedic-related issues. Most infections, pressure sores, and mechanically-related complications were seen either in the ER or through unplanned outpatient visits. 12 Both authors proposed that routine follow-up after these injuries will unlikely change the course of postoperative care. The low overall complication rate noted in both series demonstrate that orthopedic-related complications are not encountered frequently. The readmission rate within this study is similar to what is seen not only in prior studies, but also relative to a general orthopedic trauma population. 13 Furthermore, the study highlighted that the majority of readmissions in an orthopedic trauma population were either related to medical reasons or non-complications (e.g. planned re-admission, new injuries, transfers).
Our study demonstrates that patients who are discharged home are more likely to have attended their scheduled follow-up appointment. Patients who are typically discharged to a SNF typically incur higher costs and complications. 4,14 While this study did not demonstrate any difference in readmission rates between patient who were discharged home and patients who were discharged to SAR or SNF, it did highlight the challenges associated with follow-up for patients receiving post-acute care. Our experience with follow-up from a SAR or SNF is that it requires planning and coordination for the patient to be able to leave the care center and report to the office.
Transportation to the office is typically done through an ambulette and other non-emergency EMS transportation. These transportation modalities incur significant costs that are dependent not only on the geographic location, but also on the distance traveled and time spent during travel. 15 The baseline rate for an ambulette service for transport from a SAR is about $150-200 USD; however, this number is subject to the acuity of care, number of passengers, as well as distance traveled. This was cost value is provided to us from a rehab center associated with our level 1 trauma center and can vary per geographical region. If the upper end of this value is used, in our cohort of 124 SNF patients with early follow up, transportation itself comprises $24,800 USD. Furthermore, many of these patients are transported immobilized on a stretcher for the duration of preparation to travel, travel, clinic wait, clinic visit, return travel, and return to SAR/SNF.
Given the low number of orthopedic-related complications in these patients, routine follow-up for hip fracture patients, most notably to those discharged to SAR/SNFs, may incur extraneous increased costs. However, it is noted that in our study that patient readmission rates are most likely impacted by medical complications postoperatively and should thus have close follow medical follow-up either in a post-acute care setting or as an outpatient. These medical complications are often independent of the surgical procedure can potentially inflate readmission rates. 13 In lieu of in-person orthopedic early post-operative follow-up, telemedicine visits may be a viable alternative to maintain active orthopedic oversight of patient care without adding cost to the overall episode of care.
Our study does have limitations. The hospitals in our center are tertiary urban hospitals so these results may not be representative of other institutions through the country. There is an inherent bias in patients who are able to maintain follow up; they are either at a rehab facility that is run well enough to allow for this or are discharged home and have involved family and support to maintain follow up. Furthermore, our study is retrospective in nature and data is limited to what is available through chart review.
Conclusion
Patients with isolated non-orthopedic follow-up experienced more readmissions than those with follow-up. Despite this, there was no difference in orthopedic-related readmissions and changes in orthopedic management between groups as medical complications drive readmissions in both cohorts. Patients discharged to SAR/SNF, while less likely to have orthopedic follow-up, and place increased cost on the episode of care primarily through transportation costs. While orthopedic management is likely unchanged in this cohort of patients, follow up should consist of either phone calls or telemedicine visits at the minimum from an orthopedic perspective. Medical follow-up and management either in a SAR/SNF or with a patient’s primary care may be necessary to minimize postoperative readmissions for geriatric hip fractures to decrease readmission rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Konda reports the following conflict of interest: Stryker Orthopedics consultant. Dr. Egol reports the following conflict of interest: Exactech, Inc consultant. All authors declare that they have no conflicts of interest related to the contents of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Authorship has been granted only to those individuals who have contributed substantially to the research or manuscript. No sources of funding have been granted for this study.