
Abstract
Objectives
To assess outcomes following early weight bearing after distal femur fracture fixation with locked lateral plating.
Design
Retrospective cohort study
Setting
Two Level 1 Academic Trauma Centers.
Patients/Participants
Patients 18 years and older with distal femur fractures treated with locked lateral plating
Intervention
Early full weight bearing (defined as less than 30 days from date of surgery) versus restricted post-operative weight bearing
Main Outcome Measurements
Composite complication comprising malunion, nonunion, surgical site infection, re-admission, or death
Results
270 distal femur fractures were reviewed, with 165 meeting inclusion criteria. 21 patients had been allowed early full weight bearing. Fractures were divided into two groups based on when full weight bearing was allowed post-operatively. The two groups had similar fractures as determined by the distribution of AO distal femur fracture and Su periprosthetic femur fracture classifications. The early weight bearing group was significantly older and more comorbid. Despite being older, more comorbid, and allowed early full weight bearing on their fracture fixation construct, there was no difference in the rate of composite complications between groups.
Conclusion
Our data contributes to the small, but growing body of literature that has found no increased rate of fracture related complications in surgically treated distal femur fractures allowed early post-operative weight bearing.
Level of Evidence
Therapeutic Level III Study.
Introduction
Distal femur fractures are a relatively uncommon injury, making up < 1% of all adult fractures and approximately 3% of all femur fractures. 1 Most of these fractures occur in elderly women from low energy mechanisms, such as a simple standing level fall. 2 Because of the age and baseline frailty of the affected patient population, distal femur fractures are associated with a considerable degree of both morbidity and mortality. 3 Although hip fractures have received more attention for their associated mortality, studies have demonstrated that geriatric distal femur fractures carry a similar mortality to geriatric hip fractures. 4 As with hip fractures, delay of surgical fixation of distal femur fractures is associated with worse outcomes. 4 While much of the post-operative morbidity and mortality following distal femur fractures is attributable to pre-injury frailty, it is thought that post-operative immobility and diminished ambulatory capacity contribute to complications and subsequent rapid decline in health.4-7
Despite the similarity to hip fractures with regard to healthcare burden, financial impact, and morbidity/mortality, there has been little in the way of such optimization of care for distal femur fractures.2,4,8
In particular, post-operative weight bearing restrictions after distal femur fractures are an area for potential improvement. Acknowledging the importance of post-operative mobilization after hip fractures, significant research has been dedicated to developing treatments that allowed for immediate post-operative weight bearing in these patients.9,10 Unfortunately, no equivalent emphasis for distal femur fractures has been developed, and subsequently, the majority of patients are confined to weight bearing restrictions for a considerable period post-operatively.2,11
Contributing to a post-operative treatment bias towards restricted weight bearing is the history of troublesome surgical outcomes following distal femur fracture fixation. Prior to the 1970s, the majority of all distal femur fractures were treated with non-operative management.11-13 Slowly, over the course of several decades, the care of distal femur fractures has trended toward surgical management following the modernization of surgical technique, implants, and increasingly common reports of good outcomes following surgical fixation.3,5,14-16 Even with the trend towards fixation, weight bearing restrictions continue to be the norm2,13,17-19 despite reports of good outcomes permitting post-operative weight bearing.2,16,19 Therefore, despite having been exposed to the risk of surgery, these patients continue to be at risk for immobility related post-operative complications. In order to move towards a more geriatric sensitive post-operative rehabilitation protocol that allows for early full weight bearing, we set forth to assess post-operative outcomes in a review of patients permitted to early post-operative weight bearing.
Materials and Methods
This study was designed as a retrospective cohort study. After institutional review board approval was obtained, the Research Patient Data Registry (RPDR), a registry of patients treated at two large academic, level 1 trauma centers, was queried for appropriate patients. Using the RPDR, consecutive patients 18 years of age and older who had undergone surgical treatment of a distal femur fracture between 2015 and 2018 were identified. Patients were excluded if fracture fixation was accomplished with a construct other than lateral plating. There was no stipulation regarding the use of free screws outside of the plate construct. Further, though there was no distinct stipulation regarding the brand of the plating construct utilized and this study was not designed to analyze specific plating constructs. However, because of contractual obligations of the involved hospitals, the overwhelming majority of trauma implants utilized are from DePuy Synthes (West Chester, Pennsylvania). Additionally, patients were excluded if complication free follow-up was less than 180 days. Patient information, treatment data, and injury characteristics were abstracted from the electronic medical record for both the surgical admission as well as through the follow-up period. Patient data included age at time of injury and medical comorbidities, recorded as Charlson Comorbidity index (CCI). Treatment data included estimated surgical blood loss and post-operative weight bearing protocol both at time of surgical fixation and at each subsequent follow-up visit. Injury characteristics included mechanism of injury, status of fracture including periprosthetic or native femur fracture, AO/OTA fracture classification, Su periprosthetic femur fracture classification, and classification as either open or closed fracture. Patients were then sorted into two groups based on their post-operative surgeon-dictated weight bearing protocol. Patients who were allowed weight bearing as tolerated within 30 days of fracture fixation were placed into the Early weight bearing (Early WB) group. When patients’ weight bearing was restricted for greater than 30 days, they were considered part of the Standard weight bearing (Std WB) group.
Outcomes of interest were malunion, nonunion, surgical site infection, readmission within 90 days from discharge, additional fracture related surgery, and mortality within 1 year from surgery.
All statistical analyses were performed using either Microsoft Excel or STATA. Univariate statistics were calculated in the usual fashion. Categorical bivariate statistics were analyzed using chi-square tests. Continuous variables were assessed for normality using Kolmogrov–Smirnov testing. Bivariate testing for continuous variables was accomplished with either Student’s t-test, Kruskal–Wallis, or Mann–Whitney testing, where appropriate. Because the post-operative complications were disparate, a composite outcome variable was generated. Fracture related complication was defined as any of malunion, nonunion, or infection. Composite complication was defined as any of the individual outcomes of interest: malunion, nonunion, surgical site infection, additional fracture related surgery, re-admission within 90 days, and death within 365 days. Multivariable logistic regression was utilized to assess the contributing factors for these composite variables. Variables were included in the multivariable analysis if the P-value from bivariate testing was P < .10.
Results
In total, 270 distal femur fractures were reviewed. One-hundred and five fractures were excluded for not meeting appropriate criteria. Twenty-two of these were excluded because fracture fixation was accomplished with a construct other than locked lateral plating. Eighty three fractures were excluded because follow-up was less than 180 days and was free from complication. After exclusion of ineligible patients, the final analysis population consisted of 165 fractures (in 160 patients). Within the 165 analyzed fractures, there was 1 instance of free screws used outside of a plate construct and no instances of multiple plate construct. Twenty-one patients were allowed full weight bearing within 30 days of injury and therefore assigned to the Early WB group. The remaining 144 patients were labeled as the Standard WB group for analysis.
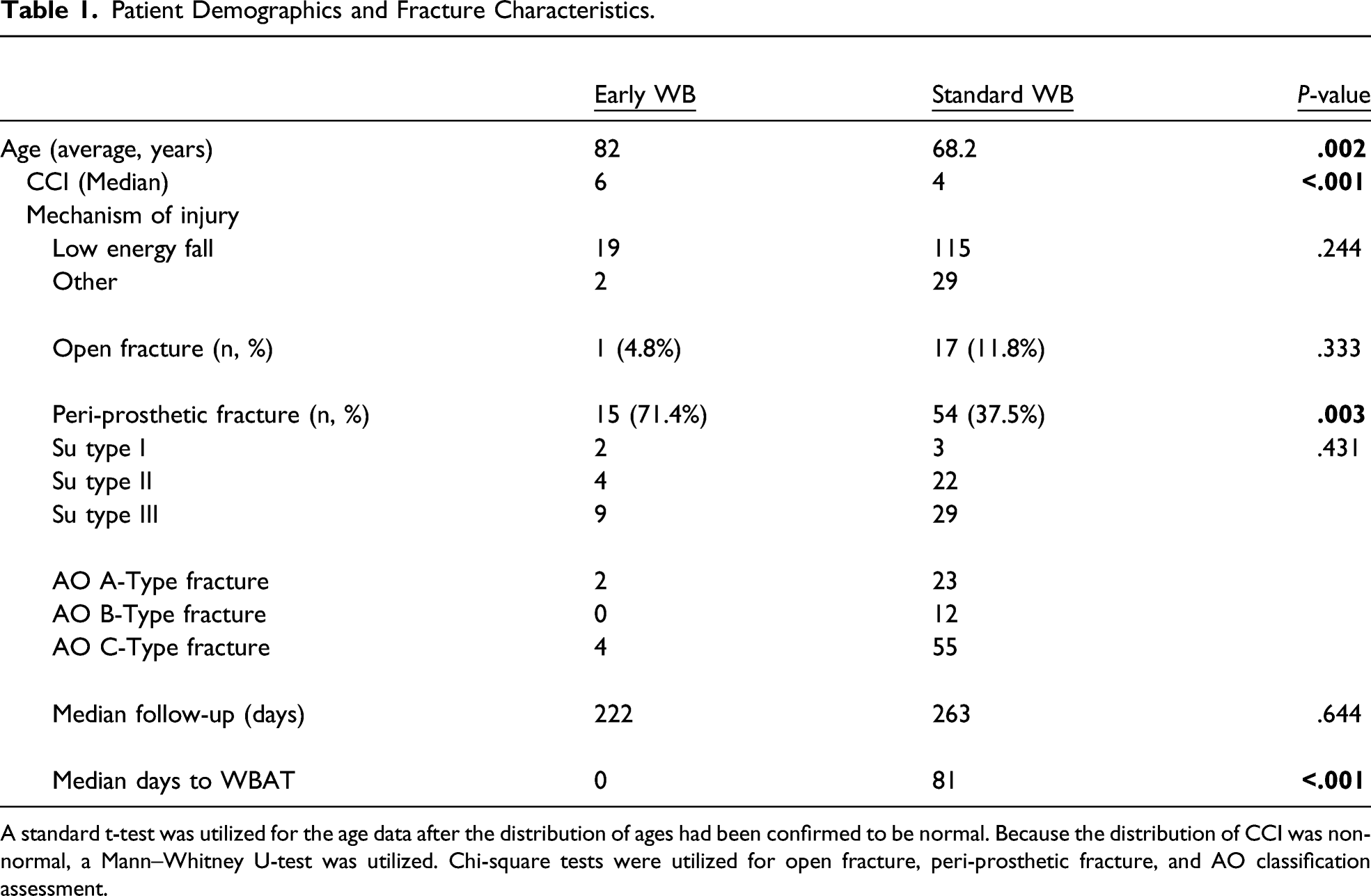
On average, the Early WB group was older and more comorbid as measured by CCI. The average patient in the Early WB group was 82 years of age at time of injury, compared to 68.2 years in the Standard WB group (P = .002). The median CCI in the Early WB group was 6, compared to 4 in the Standard WB group (P < .001). In both the Early and Std WB groups, the majority of fractures were from simple falls, 90.5% and 79.9%, respectively. The proportions of fractures resulting from simple falls was the same between the two groups (P = .244). There was no difference in the prevalence of open fracture with 1 (4.8%) in the Early WB group and 17 (11.8%) in the Standard WB group (P = .333). The Early WB group patients were statistically significantly more likely to have had a peri-prosthetic fracture (P = .003). The Early WB group had 15 (71.4%) peri-prosthetic fractures, whereas the Standard WB group had 54 (37.5%) peri-prosthetic fractures. In the Early WB group, there were 2 Su Type I, 4 Type II, and 9 Type III fractures. An example of a comminuted Su Type III fracture permitted for immediate weight bearing can be found in Figure 1. In the Standard WB group, there were three Su Type I, 22 Type II, and 29 Type III. While there was a difference in the proportion of periprosthetic fractures between the standard and early WB groups, there was no statistical difference between the distribution of Su periprosthetic fracture types between the two groups (P = .431). In the Early WB group, there were two A-type fractures, zero B-type fractures, and two C-type fractures. In the Standard WB group, there were 23 A, 12 B, and 55 C-type fractures. Median follow-up in the Early and Standard WB groups was 222 and 263 days, respectively. This difference did not meet statistical significance (P = .644). The median time to weight bearing as tolerated in the Early WB group was 0 days, or post-op day 0. In the Standard WB group, the median time to surgeon permitted weight bearing as tolerated was 81 days (P < .001). A summary of demographic and treatment related information can be found summarized in Table 1. Representative radiographs of a comminuted Su Type III femur fracture allowed early WB after fixation. Figure 1A and 1B represent pre-op and 2 week post-op clinic visit radiographs. Patient Demographics and Fracture Characteristics. A standard t-test was utilized for the age data after the distribution of ages had been confirmed to be normal. Because the distribution of CCI was non-normal, a Mann–Whitney U-test was utilized. Chi-square tests were utilized for open fracture, peri-prosthetic fracture, and AO classification assessment.
In the Early WB group, there was 1 malunion (4.8%), 1 nonunion (4.8%), 1 infection (4.8%), and 6 readmissions (28.6%). In the Standard WB group, there was 3 malunions (2.1%), 17 nonunions (11.8%), 10 infections (6.9%), and 29 readmissions (20.1%). There were no differences in the rates of malunion, nonunion, infection, or readmission between groups (P > .05 for all). Further, there was no difference between groups in the rate of collective fracture related complications, defined as malunion, nonunion, or post-operative infection (P = .62). The Early WB group had 1 (4.8%) re-operation, compared to 40 (27.8%) in the Standard WB group; this difference was statistically significant (P = .023). Significantly more patients in the Early WB group died within the follow-up time period (P = .005). There were 6 deaths (28.6%) in the Early WB group, compared to 13 deaths (8.3%) in the Standard WB group.
Overview of Post-Operative Complications. Please Note That All Complications Were Listed Within, and Therefore, one Patient may be Reflected Multiple Times if They Encountered Multiple Complications.

Because of the high proportion of periprosthetic fractures in the Early WB group and the possibility that weight bearing status may have influenced complication rates differently in periprosthetic fractures, a post-hoc subgroup analysis of complications limited to periprosthetic fractures was conducted. With regard to fracture related complications, 13.3% of periprosthetic fractures allowed early weight bearing experienced complications, compared to 22.2% in periprosthetic fractures with restricted post-op weight bearing. This difference was not significantly different (P = .449). Analysis of any complication revealed a 53.3% complication rate in periprosthetic fractures allowed early weight bearing. Similarly, patients with periprosthetic fractures that had restricted weight bearing experienced a composite complication 50% of the time. This again was not statistically significantly different (P = .819). Multivariable logistic regression model included age, periprosthetic fracture, CCI, and Early v. Standard weight bearing post-operative protocol. In the multivariable model, only age (P = .002) and CCI (P = .006) were significantly associated with the likelihood of experiencing a complication. Importantly, surgeon permitted early weight bearing and periprosthetic fractures were not associated with complications.
Discussion
Distal femur fractures are complicated injuries associated with multiple complications for which there is no optimized standard of care.1,2 Further complicating these injuries is the frail, multiply comorbid, elderly patient population who tend to sustain distal femur fractures.2-4 Subsequently, these patients are at significant risk of experiencing post-operative morbidity and mortality, with series reporting mortality rates up to 35% at 1 year post-injury.2-4 With regard to post-operative mortality, previous authors have commented on the similarity between geriatric hip fractures and geriatric distal femur fractures.4,20 Given the high incidence of hip fractures, multiple best practice initiatives have been undertaken to optimize the care of geriatric hip fractures with 1 notable point being the necessity of post-operative mobility.10,21 Siu et al demonstrated that improved mobility after hip fracture was associated with reduced mortality at 6-months post-injury. 22
One factor altering the ability to mobilize frail geriatric fracture patients post-operatively is surgeon-dictated weight bearing status. It is our experience that in this frail patient population, mobilization while maintaining a reduced weight bearing status in the operative leg is often so difficult that it significantly diminishes mobility at all. Often, physical therapists and nursing staff, unable to mobilize a patient with weight bearing restriction and fearful for injuring the operative leg will therefore defer mobilization attempts altogether, instead opting for in bed or in chair mobility. This supposition has been supported by previous authors. 23
After dedicated study, hip fracture care has evolved to allow full weight bearing without compromising care.9,24,25 Unfortunately, there is no consensus on the post-operative rehabilitation after distal femur fracture fixation and often surgeons recommend restricted weight bearing.2,11 There are, however, multiple small studies of distal femur fracture fixation reporting good outcomes with surgeon-dictated full weight bearing post-operatively. In 2016, Smith et al reported on 52 peri-prosthetic distal femur fractures allowed full weight bearing with a fracture union rate of 93% at 20 weeks. 19 Similarly, Poole et al in their 2017 review of 127 distal femur fractures treated with locked femoral plating, reported no increase in failure of fixation in the 84% of patients allowed unrestricted weight bearing post-operatively 17 ; however, this study provided no direct comparison between treatment groups. Smith et al, in their 2015 review of 105 elderly distal femur fracture patients, reported no increase in complication rate in the 15 patients allowed full weight bearing post-operatively. 2 Consigliere et al, recommended allowance of early post-operative weight bearing after distal femur fracture fixation after finding no increased rate of complications in their review of 51 patients. 26 Our study adds to and expands upon this growing body of literature assessing early, immediate weight bearing after distal femur fracture fixation in particular by providing dedicated analysis of patient comorbidities.
It is important to note that the two groups analyzed in our study had important similarities and differences. Both groups most commonly suffered their fracture from a simple fall. There was no difference in the distribution of fracture classification between groups. However, the Early WB group was significantly older and had significantly higher Charlson Comorbidity Index scores indicating a higher burden of comorbid conditions. Despite the increased age, comorbidities, and early weight bearing on fracture fixation construct in the Early WB group, the rate of complications were similar between both groups. Taken together, the more fragile patients in the Early WB group were seemingly at increased risk for complications, yet there was no appreciable difference in actual complications observed compared to the Std WB group. The Early WB did have significantly more mortalities within 1 year of injury, which we interpret as a function of their advanced age and higher Charlson Comorbidity Index scores rather than a function of allowing these patients to fully bear weight.
Our study is not without flaws. It was a small retrospective study, analyzing surgeon recommended weight bearing status without the ability to account for indication for post-operative protocol. This, however, is consistent with prior published literature on weight bearing after distal femur fracture fixation. It is possible that institutional concerns regarding the deleterious effects of restricted weight bearing in severely frail, elderly patients biased decision-making and therefore, we suspect that full weight bearing was intentionally recommended for the most vulnerable patients. This is supported by the fact that the Early WB group was both more elderly and had higher comorbidity scores. These differences in patient characteristics would bias the data towards more complications in the Early WB group; however, there were similar rates of complications in both groups.
An additional consideration is the possibility that restricted weight bearing was recommended for cases in which there was hesitation or doubt about the quality of fracture fixation. If this were the case, then the more tenuous fixation constructs would be found in the Std WB group and would potentially bias toward more complications in the Std WB group. We are unable to definitively make comment on this possibility, but in our estimation, it is unlikely that the fracture fixation was systematically worse in the Std WB group given the fact that there was no difference between groups with respect to fracture morphology and the patients were younger and less comorbid on average.
Further, this analysis centered on surgeon recommended weight bearing, but did not directly assess whether patients walked with full weight bearing on their fracture fixation construct. Previous literature has demonstrated that many geriatric patients are poor at maintaining weight bearing restrictions and therefore it is possible that the distinction between our two groups is blurred. 27 However, this analytical style falls in line with the prior studies assessing the weight bearing after distal femur fracture. Future studies analyzing the effect of weight bearing on locked lateral plating for distal femur fracture would benefit from direct assessment of weight bearing.
In conclusion, our data contributes to the growing body of small retrospective studies that has found no increased rate of complications in surgically treated distal femur fractures allowed early post-operative weight bearing. Our data is novel in its direct assessment of patient comorbidities, fracture morphology, and mechanism of injury and therefore expands the literature in its ability to provide a multi-faceted assessment of factors contributing to post-operative complications. With knowledge that these elderly, frail, comorbid patients are at high risk of post-operative morbidity and mortality and appreciating the importance of post-operative mobilization in the elderly, we believe that there is a role for consideration of early weight bearing in the correct patient population. This stance is supported by our study and the previous small, cohort studies, but the literature remains without high quality, prospective trial evaluating post-operative weight bearing in elderly patients with distal femur fractures. These findings highlight a need for and can function as a seed for future study of post-operative rehabilitation of distal femur fractures.
Footnotes
Author Note
This investigation was performed at the Massachusetts General Hospital and Brigham and Women’s Hospital
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.