
Abstract
Background: There is limited information in the literature on the outcomes and complications in elderly patients who sustain high-energy hip fractures. As the population ages, the incidence of high-energy geriatric hip fractures is expected to increase. The purpose of this study was to analyze the outcomes and complications in patients aged 65 years or older, who sustained a high-energy proximal femur fracture. Methods: Retrospective review of a prospective trauma database from January 2000 to April 2011 at a single US academic level-1 trauma center. Inclusion criteria consisted of all patients of age 65 years or older, who sustained a proximal femur fracture related to a high-energy trauma mechanism. Details concerning injury, acute treatment, and clinical course and outcome were obtained from medical records and radiographs. Results: We identified 509 proximal femur fractures in patients older than 65 years of age, of which 32 (6.3%) were related to a high-energy trauma mechanism. The mean age in the study group was 72.2 years (range 65-87), with a mean injury severity score of 20 points (range 9-57). Three patients died before discharge (9.4%), and 22 of 32 patients sustained at least one complication (68.8%). Blunt chest trauma represented the most frequently associated injury, and the main root cause of pulmonary complications. The patients' age and comorbidities did not significantly correlate with the rate of complications and the 1-year mortality. Conclusions: High-energy proximal femur fractures in elderly patients are not very common and are associated with a low in-hospital mortality rate of less than 10%, despite high rate of complications of nearly 70%. This selective cohort of patients requires a particular attention to respiratory management due to the high incidence of associated chest trauma.
Introduction
There is a paucity of peer-reviewed publications in the literature addressing proximal femur fractures in elderly patients resulting from high-energy trauma mechanisms.1–3 Impressively, recent epidemiological studies have revealed that more than one third of all trauma patients are aged 65 years or older, with 10% older than 80 years. 4 In addition, the number of hip fractures in the United States continues to increase drastically, with approximately 300 000 fractures occurring each year.5–9 The mortality of isolated proximal femur fractures in elderly patients is very high,6,10,11 and the case fatality in multiply-injured elderly patients has been shown to be about twice as high as in younger patients.12,13
Due to the constantly increasing age of our population, it is important for all health care providers, particularly for orthopedic trauma surgeons, to be aware of the complex clinical aspects related to the care of the highly vulnerable cohort of elderly patients with high-energy hip fractures. The purpose of the present study was to investigate the complications and outcomes in patients aged 65 years or older who sustained a proximal femur fracture as a result of a high-energy trauma mechanism.
Methods
After institutional review board approval, we performed a retrospective review of a prospective database at a single US academic level-1 trauma center from January 1, 2000 to April 30, 2011. Inclusion criteria consisted of all patients aged 65 years or older with a high-energy mechanism of injury resulting in a closed or open fracture to the femoral head, neck, trochanteric, and subtrochanteric zone (AO/OTA type 31-A/B/C and 32-X.1). “High-energy” trauma was defined as any of the following mechanisms: (1) motor vehicle or motorcycle accidents; (2) bicycle accidents; (3) skiing accidents (whereby patients sustained “true” high-energy injuries including a skier who hit a gate at high speed and fell on his head, and a second skier who was found unconscious after hitting a tree at high speed); (4) pedestrians being hit by any of the above; (5) crushing injuries; and (6) falls from a height of ≥10 feet. Exclusion criteria consisted of patients younger than 65 years of age, low-energy trauma mechanisms (eg, fall from standing or walking, falls from a height <10 ft), traumatic hip dislocations in the absence of a fracture, periprosthetic femur fractures, and pathologic fractures related to an underlying metastatic disease.
The following demographic data and outcome parameters were extracted from the database: patient age, gender, mechanism of injury, injury severity score (ISS), date of injury, date of surgery, AO/OTA fracture classification, 14 operative procedure, type of implant used, associated injuries, hospital length of stay (LOS), intensive care unit (ICU) LOS, ventilator-dependent days, comorbidities, complications, and in-hospital mortality.
Statistical analysis was performed using GraphPad Prism version 3.03 (GraphPad software, Inc, La Jolla, California). Descriptive statistics were used to characterize demographic data and outcome parameters in the study cohort. Mann-Whitney U test, Kruskal-Wallis test, Dunn multiple comparison test, and linear regression analysis were applied as appropriate. A P < .05 was considered statistically significant.
Results
During the study period, 509 patients were identified with an age 65 years or older and a proximal femur fracture. Of these, 32 patients (27 males and 5 females) had sustained a high-energy trauma mechanism, based on the definition outlined in the Methods section (6.3%). The mean age of the study population was 72.2 years (range 65-87). The mean ISS was 20 points (range 9-57). The patients' demographic data are shown in Table 1. The algorithm for patient selection, the AO/OTA fracture classification, and the selected treatment modality are shown in Figure 1. The most common mechanisms of injury were motor vehicle accidents (n = 12), pedestrian hits (n = 9), and bicycle accidents (n = 4). Operative fracture fixation was performed in 27 of 32 patients, while 3 fractures were treated nonoperatively, and 2 patients died before surgery. The overall injury severity, based on ISS scoring, did not differ significantly between the different mechanisms of injury (P = .3922). Associated injuries consisted of blunt chest trauma (n = 13), pelvic fractures or acetabular fractures (n = 12), spine fractures (n = 9), associated lower extremity factures (n = 7), and traumatic brain injuries (n = 7).
Patient Demographics and Injury Characteristics in Elderly 32 Patients With High-Energy Proximal Femur Fractures


Abbreviations: ISS, injury severity score; Fx, fracture(s); MVA, motor vehicle accident.

Flowchart depicting patient selection criteria, AO/OTA fracture classification, and injury-specific treatment modality in 32 elderly patients with high-energy proximal femur fractures.
The mean length of hospital stay was 18.1 days (range 3-85). Three patients died before discharge (in-hospital mortality: 9.4%). Of these, 2 patients died from respiratory failure related to severe chest trauma and 1 patient died from multiorgan failure (MOF). Pulmonary complications occurred in 10 of 13 patients who suffered a blunt chest trauma (77%). Overall, 22 patients sustained at least one complication (68.8%). The specific complications are listed in Table 2.
Complications and Unplanned Surgical Revisions in Elderly 32 Patients With High-Energy Proximal Femur Fractures

Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism.
There was no significant correlation between age and hospital LOS (P = .349) or ICU LOS (P = .354), ventilator-dependent days (P = .889), ISS (P = .95), number of complications (P = .147), or number of comorbidities (P = .355; Figure 2). Age was not significantly different between survivors and nonsurvivors (P = .075) or between patients who could be discharged home versus those who were transferred to a nursing facility (P = .26). As shown in Figure 3, the number of comorbidities did not correlate with the number of complications (P = .629), hospital LOS (P = .123), ICU LOS (P = .949), or ventilator-dependent days (P = .634). The ISS was significantly higher in those patients who required intensive care treatment (P = .022), but there was no correlation with ICU LOS (P = .204) or ventilator-dependent days (P = .742). Figure 4 illustrates an exemplary case (patient #13).
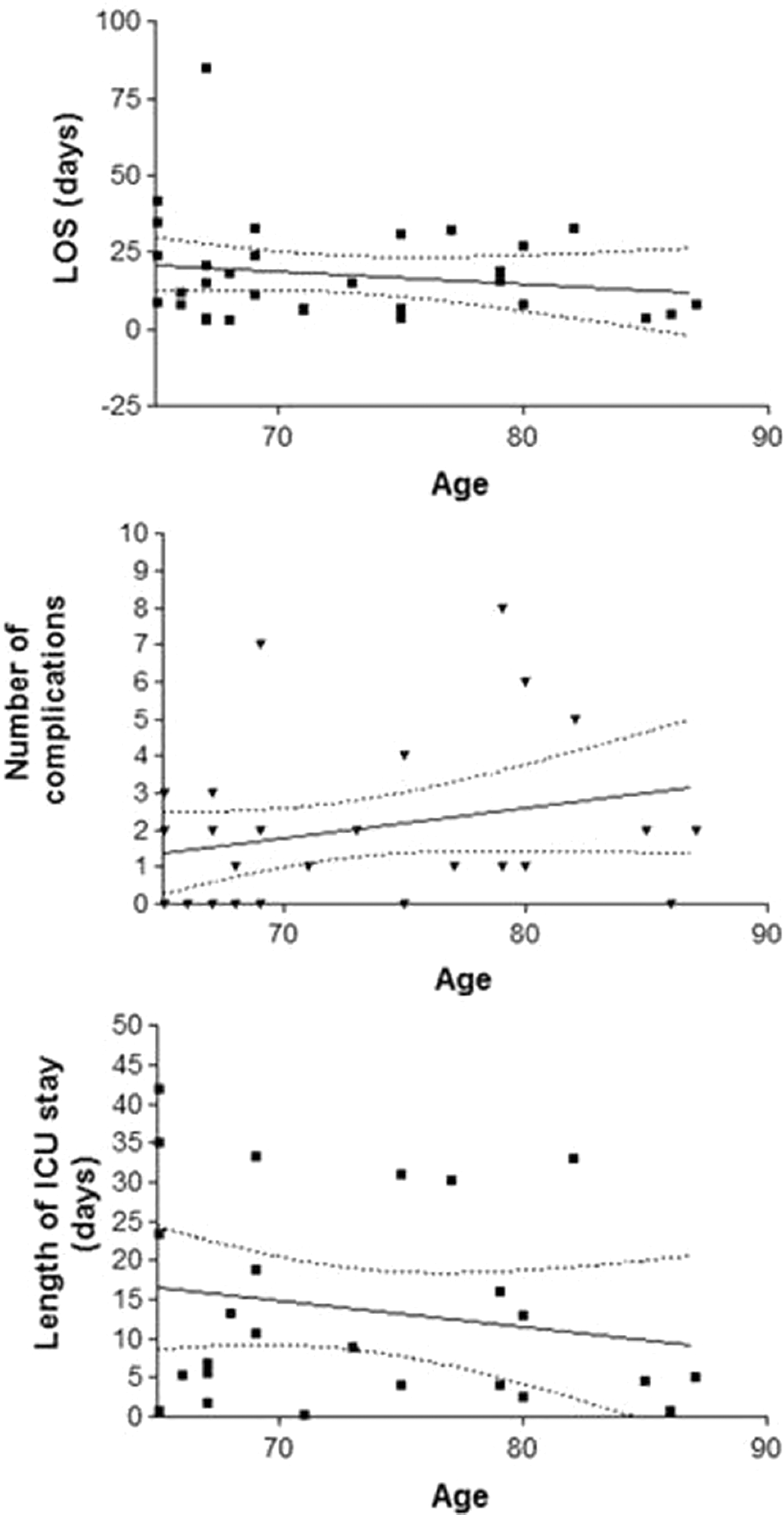
Scatter plots of linear regression analysis for age versus length of hospital stay (LOS), number of complications, and length of intensive care unit (ICU) stay in 32 elderly patients with high-energy proximal femur fractures. See text for detailed explanations.

Scatter plots of linear regression analysis for comorbidities versus length of hospital stay (LOS), number of complications, and length of intensive care unit (ICU) stay in 32 elderly patients with high-energy proximal femur fractures. See text for detailed explanations.

Case example of the long-term outcome of a 67-year-old patient (#13) who sustainedmultiple injuries after amotorcycle accident. The patient was initially managed by a “damage control” procedure with spanning external fixation of an ipsilateral right femoral neck fracture and acetabular fracture related to a central hip dislocation (A, B) and ipsilateral femur shaft fracture (C). The patient also sustained a contralateral bicondylar tibial plateau fracture (not shown). After resuscitation, the orthopedic injuriesweremanaged by a staged conversion to internal fixation during the physiological “time-window of opportunity” between days 5 and 10 after trauma (D-G). The patient recovered well from his critical injuries and was discharged within 2 weeks after trauma. After 2 years, the patient developed right hip pain related to avascular necrosis of the femoral head and underwent a hardware removal and total hip arthroplasty (H, I). He is currently ambulating without restrictions and has an excellent quality of life.
Discussion
Hip fractures represent a major cause of morbidity and mortality in elderly patients.4,11 In the present study, we found that high-energy proximal femur fractures are rare injuries, which account for only 6.3% of all hip fractures in geriatric patients. Interestingly, patients' age and the number of preexisting medical conditions did not influence the hospital or ICU LOS and did not correlate with the number of complications. These findings are in agreement with a recent study on severely injured geriatric patients, which lacked to find a correlation between patients'comorbidities with the in-hospital mortality rate. 15 In contrast, previous studies have revealed a correlation between the presence of medical comorbidities, delay to surgery, and adverse outcome in low-energy geriatric hip fractures.10,16,17
Chest trauma represents one of the major “lethal injuries” in severely injured patients, 18 particularly in the elder population. Accordingly, we found that 13 of 32 patients with high-energy hip fracture patients had an associated blunt chest trauma, with an associated pulmonary complication rate of 77%. After exclusion of head injuries, elderly trauma patients with chest injuries have been shown to have a high mortality of up to 30%. 19 Early in-hospital mortality rates for elderly patients with low-energy hip fractures have been shown to range between 3% and 13%.6,10,11,20 In contrast, the fatality of multiply-injured geriatric patients is significantly increased and is reported to range between 38% and 53%,12,13 and even higher in the presence of early coagulopathy. 21 The early mortality of high-energy proximal femur fractures in the present study (9.4%) appears lower than the numbers published in the peer-reviewed literature, which may relate to an aggressive, proactive management strategy of this highly vulnerable patient population, particularly, as it relates to the early recognition and management of postinjury coagulopathy at our institution.22,23
High-energy trauma to the hip and multiple injuries leads to a graded immune response including an early hyper-inflammatory (systemic inflammatory response syndrome) and a delayed immunosuppressive (compensatory anti-inflammatory response) episode with altered plasma and tissue levels of cytokines and interleukins.24–27 This deranged host immunity may lead to systemic inflammatory complications, coagulopathy, MOF, and subsequent death.21,22,28,29 Recently, elevated plasma levels of proinflammatory and anti-inflammatory cytokines (tumor necrosis factor α, interleukin [IL]-6, and IL-10) have been shown to be independent predictors of mortality and complications in geriatric patients with hip fractures. 30
Two recent retrospective studies have shown that vital signs of geriatric trauma patients on presentation are not as predictive for outcome as in the younger patient population.19,31 In these previous studies, elder patients were less likely to show alarming vital signs related to tachycardia and hypovolemia, thus creating a higher risk of being “undertriaged” on presentation in the emergency department.19,31 Impressively, the in-hospital mortality rate for “undertriaged” patients was 6% in young trauma patients compared with 21% in the elderly population. 31 To overcome this alarming issue, standardized protocols for the early evaluation of patients with acute trauma will have to be adjusted for risk stratification by age groups.22,32 In a recent study, van Zeeland and colleagues evaluated a new “POSSUM” score (“Physiologic and operative severity score for the enumeration of mortality and morbidity”) that was shown to be sensitive and predictive of outcome in 272 consecutive patients with hip fractures. 32
In the present study, patient age and the presence of medical comorbidities did not appear to correlate with the acute in-hospital mortality. Beyond a doubt, the main limitations of this study are represented by the retrospective nature of the study design and the small patient cohort included, which may not be representative for a larger prospective study population. In addition, this study was not designed to determine long-term clinical outcomes, quality of life, and mortality beyond the acute hospital care phase. Future studies will have to be designed as large-scale multicenter collaborative efforts to determine long-term outcomes in this rare albeit highly vulnerable population of elderly patients with high-energy hip fractures.
Conclusion
High-energy proximal femur fractures in elderly patients are rare injuries resulting mainly from motor vehicle accidents, pedestrian hits, or bicycle accidents. Associated injuries to the chest are very common and represent the root cause of the high incidence of pulmonary complications. While the acute in-hospital mortality appears to be low (<10%), these patients are susceptible to a high complication rate of around 70%. The concept of early fracture fixation in conjunction with timely recognition and proactive management of associated conditions, such as postinjury coagulopathy and chest trauma, may be of “key” importance for reducing the early mortality in this highly vulnerable patient cohort.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
The author(s) received no financial support for the research, authorship, and/or publication of this article.