
Abstract
Introduction
Due to the aging population the incidence of Low Energy Fractures (LEF) increases. LEF have high mortality and morbidity rates and often cause elderly to lose independence. Patient-reported outcomes, such as Quality of Life (QoL) and patient satisfaction (PS) are needed to evaluate treatment, estimate cost-benefit analyses, and to improve clinical decision-making and patient-centered care.
Objective
The primary goal was to evaluate QoL and PS in patients with LEF, and to compare QoL scores to the community dwelling population. Second, we observed the amount and type of physiotherapy (PT) sessions the patients conducted.
Methods
A single-center cohort study was conducted in Switzerland. Patients between 50 and 85 years, who were treated in the hospital for LEF, were followed 1 year after initial fracture. Data on QoL were obtained through the Euroqol-5-Dimension questionnaire-3-Level (EQ-5D-3L) and the EQ VAS (visual analog scale). PS was measured by a VAS on satisfaction with treatment outcome. Data on PT sessions, mobility and use of analgesics were collected by telephone interviews and written surveys. Results were compared between the different fracture locations and subgroup analyses were performed for age categories.
Results
411 patients were included for analysis. The median scores of the EQ-5D-3L index—VAS and PS were 0.90 (0.75–1.0), 90 (71.3–95) and 100 (90–100). Significant differences in all scores were found between fracture location (P < .05), with hip fracture patients and patients with a malleolar fracture scoring lowest in all measures. QoL index in hip fracture patients was 0.76 (0.70–1.00), QoL VAS 80 (70–90), and PS 95 (80–100). Median amount of PT sessions in all patients was 18 (9–27) and a significant difference was found between fracture locations. Patients with a fracture of the humerus received the highest amount of PT sessions 27 (18–36), hip fracture patients had a median of 18 (9–27) sessions.
Conclusion
At follow-up, QoL throughout all patients with a LEF was comparable to a normal population. Remarkably, though hip fracture patients seem to suffer from a clinically relevant loss of QoL, they received fewer PT sessions and performed fewer long-lasting home training than patients with a humerus fracture. Intensive, progressive rehabilitation with a high frequency of supervised training is recommended after hip fracture. The low frequency of PT sessions found in this study is unsatisfying. In hip fracture patients and in patients with a malleolar fracture, especially when aged over 75 years, more efforts are required to improve rehabilitation and subsequently QoL.
Introduction
Low Energy Fractures (LEF), defined as fractures resulting from standing height or less, are a common health problem and due to the aging population the incidence of LEF continues to increase.1-3 Community-dwelling elderly over the age of 75 have an estimated 32% chance of experiencing a LEF within a one year period. This risk continues to increase with age. 4 Mortality rates, morbidity rates, and costs are high and complete recovery is seldom.5,6 LEF patients often lose their independence and become permanently institutionalized. 7 Recent literature stresses the importance of patient-reported outcome measures (PROMs) such as Quality of Life (QoL), and patient satisfaction (PS). 8 PROMs are essential for evaluating treatment, analyzing cost-effectiveness and improving clinical decision-making and patient-centered care. In previous literature, it has been reported that QoL is negatively affected by a LEF. 5 However, there is a lack of studies comparing QoL and other PROMs (i.e., PS) between different fracture locations.
The primary aim of this study was evaluating QoL and PS in LEF patients in Switzerland and comparing QoL and QoL domains between different fracture locations. Also, comparisons were made to community-dwelling elderly in comparable age groups. Second, we aimed to evaluate the amount of physiotherapy (PT) sessions conducted for rehabilitation.
Materials and Methods
This study is written conforming to the STROBE statement. 9
Study Design
An observational cohort study was conducted in one Level-I Swiss trauma center. Approval was obtained from the ethics committee of the Canton Lucerne (approval number 616). Enrollments were carried out after receiving informed consents. This study is part of a larger research project on LEF in trauma patients. 10 The first study of this project focused on improving osteoporosis screening and treatment, the second study on Fear of Falling, the occurrence and prevention of subsequent falls and fractures. Inclusion criteria, baseline data, and flowchart were similar in all studies. 11
Study Patients
Eligibility criteria.

Data Collection
Data were collected during a follow-up period of one year. Baseline data were assessed retrospectively through the electronical medical record at time of injury. Baseline data included: Age, gender, American Society of Anesthesiologists score (ASA), body mass index (BMI), and fracture location according to the Arbeitsgemeinschaft für Osteosynthesefragen classification.13-15 Follow-up data were collected in two ways. First, a written questionnaire was sent to the patients’ home address. Second, patients were interviewed by telephone. Primary outcome was: EuroQol-5 Dimension 3-Level (EQ-5D-3L) index score and the EQ-VAS (visual analog scale), a validated, generic PROM. 16 Secondary outcomes included: PS, which was assessed by asking: “On a scale from 0–100, in general, how satisfied you are with the result of the treatment.”17-19 QoL outcomes were compared to the EQ-5D-3L normative data sets. Data on anxiety/depression, mobility, and usual activities were extracted from the EQ-5D-3L and individually analyzed. Amount and type of PT sessions were recorded by patients. To improve data quality, four independent study nurses were trained to conduct standardized and structured telephone interviews.
Statistical Analyses
Data was analyzed using SPSS Statistics version 25 (IBM Corporation Armonk, NY). Results were evaluated using total numbers (N) and percentages for categorical variables and median values (M) with inter-quartile ranges for numeric values (i.e., age). The Shapiro–Wilks test was used to test for normality. We compared between fracture groups using the Chi-square test and Mann–Whitney U test for two groups and the Kruskal–Wallis and independent sample t test for >2 groups. A post hoc analysis was performed with the Bonferroni method and the 95% confidence interval (CI) for the median difference (Mdn diff) was calculated using Hodges–Lehman. Mean and standard deviations were reported to compare our findings to previous literature. Subgroup analyses were performed for age categories: a) 65–74 years, b) patients aged ≥75 years, and c) 50–64 years. Missing values were assessed through available case analyses and excluded from analyses.
Results
Figure 1 shows the flowchart of patient inclusion. Out of 2,230 fracture patients, invitations were sent to 823 potentially eligible patients. 411 patients returned the written questionnaires. 390 patients were reached for a telephone interview. Patient flowchart.
Patient Characteristics
Baseline characteristics.
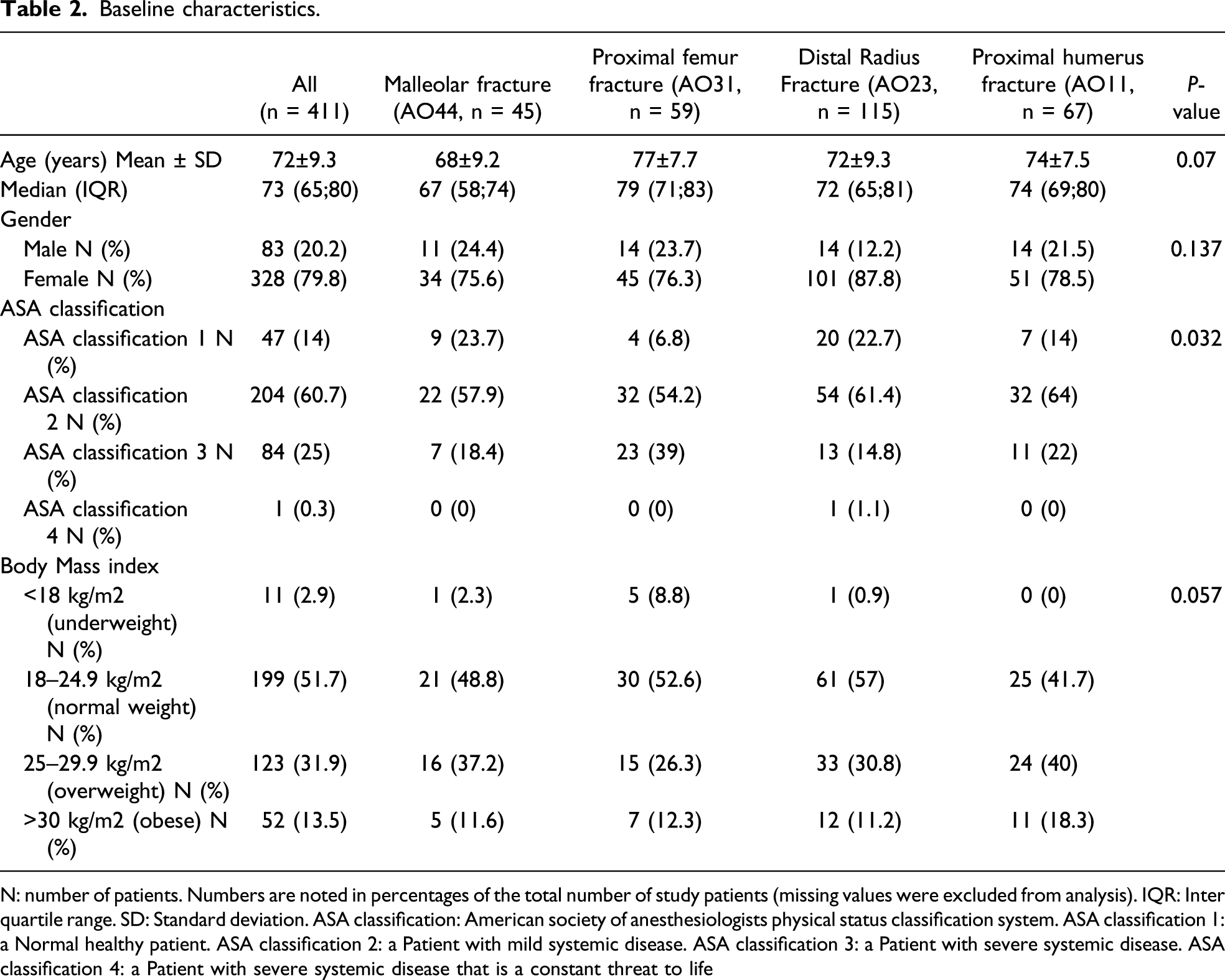
N: number of patients. Numbers are noted in percentages of the total number of study patients (missing values were excluded from analysis). IQR: Inter quartile range. SD: Standard deviation. ASA classification: American society of anesthesiologists physical status classification system. ASA classification 1: a Normal healthy patient. ASA classification 2: a Patient with mild systemic disease. ASA classification 3: a Patient with severe systemic disease. ASA classification 4: a Patient with severe systemic disease that is a constant threat to life
No significant differences between study participants and non-participants were found in age (P = .496), gender (P = .0668), and BMI (P = .885). Median age of non-study participants was 72 (64–81).
Primary Outcomes
Postoperative outcomes.

Note: N: number of patients. Numbers are noted in percentages of the total number of analyzed study patients per fracture location. IQR: Inter quartile range. EuroQol-5 dimension 3-Level.VAS: Visual analog scale. Missing values were excluded from analysis.
Subgroup Analysis of Primary Outcomes According to Age Categories
Patients aged 65–74: Median EQ-5D-3L index score was 1.0 (0.85; 1.0) and EQ-VAS was 90 (80; 95). PS was 100 (90; 100). There were no differences in EQ-5D-3L index, VAS, and PS between fracture locations. Significant differences between fracture locations were found in amount of PT sessions (P < .001). A difference was found in the number of patients performing home exercises one year after their fracture (P = .018). Supplementary Tables 3 and 5A show more detailed information. Patients aged 75years or older: There was a significant difference in EQ-5D-3L index scores between fracture locations (Mdn diff: 0.08; 95% CI 0.00–.016; P = .045) with hip fractures and ankle fractures scoring lowest: 0.75 (0.70; 1.00) for hip fractures and 0.75 (0.74; 1.00) for ankle fractures. Between fracture locations, no differences were found in EQ-VAS scores and PS. PT sessions did differ significantly (P =.02). A significant difference was found in the number of patients who performed home exercises after one year (P < .001). Details are shown in Supplementary Tables 4 and 5B. Patients aged 50–64years of age: There was a significant difference in QoL VAS score (P = .023), strength training (P = .032), and balance training (P < .001) between fracture groups. Malleolar and hip fracture patients received more strength training and balance training, distal radius fracture patients reported highest VAS scores. See Supplementary Table 5 for more information.
Secondary Outcomes
Regarding individual aspects of the EQ-5D-3L, we found differences between fracture locations in mobility (P < .001), self-care (P = .039), and usual activities (P = .016). Patients with an upper extremity fracture experienced fewer problems with anxiety/depression (P = .045) and reported to have less problems with mobility (P < .001). Hip fracture patients had the most problems with postoperative mobility and patients with a fracture of the wrist the least (44.1% of hip fracture patients vs 13.4% of wrist fracture patients, P < .001). 40.6% of all patients reported use of analgesics due to pain. 56% of hip fracture patients reported moderate to severe levels of pain and moderate or severe problems with the other QoL domains. Loss of QoL domains increased with age. Median amount of PT sessions was 18 (9; 27), a significant difference was found between fracture groups (P < .001). Differences between fracture groups were found in the amount of patients who performed strength training for the lower extremities, balance training, and in the proportion of patients who performed home exercises 1 year after trauma. For more details see Table 3 and supplement.
Discussion
This study compared QoL, PS, and PT outcomes between fracture locations of LEF patients after one-year follow-up. Significant differences in QoL and PT were observed between fracture locations. Hip fracture patients reported lowest QoL scores, and patients with a humerus fracture received most PT sessions. Hip fracture patients, despite scoring the lowest in QoL and PS, received considerably fewer PT sessions. Subgroup analysis of patients ≥75 years also revealed a significant difference in QoL index between fracture locations, both hip and ankle fracture patients had clinically relevant lower QoL index scores compared to the other fracture locations. No significant difference in QoL between fracture locations was found in patients aged 65–74 years old. Elderly hip and ankle fracture patients, especially over the age of 75, seem to be at greater risk of loss of QoL compared to patients with wrist or humerus fractures. When comparing our data to the data of equivalent age categories of the community-dwelling population, QoL scores in our patients were comparable, or even somewhat higher.
When comparing QoL scores, it should be noted that QoL depends on multiple factors such as social, economical, cultural, environmental factors, and others. In this study, we intended to compare similar patient groups; however, being aware that abovementioned factors will contribute to any differences found.8,20
Previous literature shows a negative correlation between LEF and QoL. A comparable, multicenter study that was conducted in 11 countries (excluding Switzerland) reported EQ-5D-3L scores after a one-year follow-up. Similar to this study, they found lower QoL scores in hip fracture patients (0.64 index and 67 VAS) compared to wrist fracture patients (0.87 index and 80 VAS). 21 Despite the lower mean age in their study population (73 ± 10 years in hip fractures, 65 ± 9 years in distal radius fractures), EQ-5D-3L index and—VAS scores in this study were higher in hip fracture patients (0.77 index and 77 VAS) and in wrist fracture patients (0.89 index and 86 VAS). Intercultural differences in health status, perception of health, and QoL and patient expectations may have contributed to the variation in findings. Whether different treatment modalities or rehabilitation procedures have contributed to QoL differences would need to be further explored.
We used two manners to put QoL outcomes into perspective:
First, EQ-5D-3 L provides normative data through population value sets for 24 countries, which show EQ-5D-3L values in the general population for different age groups. 20 To compare results, we performed subgroups analyses within the same age categories. Since no value sets were calculated for the Swiss population, we compared our data to German, Dutch, and French data set because we consider these populations most comparable. Mean QoL index score for Germans aged 65–74 years old is 0.84, Dutch 0.86 and French 0.80 vs 0.90 in our study. Mean population index scores in people aged ≥75 years were: 0.77 in Germany, France 0.76, and the Netherlands 0.80 vs 0.81 in our study.
Second, for QoL scores, a “Minimal Clinically Important Difference” (MCID), defined as “the smallest amount of benefit that the patient can recognize and value,” is often used to interpret differences. 22 An index value of 0.074 is considered a MCID for EQ-5D-3L. 23
With abovementioned noted, QoL in our study was comparable and even somewhat higher to that of the general (German, Dutch, and French) population. This may be caused by international differences in socio-economics, culture, and environment. However, it would be interesting to further research reasons for these higher QoL scores. Regarding hip fracture patients, our results suggest that they have a clinically relevant lower QoL compared to the whole study population (M 0.76 vs 0.9). This is consistent with other research.21,24,25
In patients aged 65–74 years, no difference was found in QoL index between fracture groups. Patients in this age category seemed to better sustain and reach an acceptable level of QoL. Still, there is a clinically relevant difference in the QoL index in ankle and hip fracture patients (M for both: 0.9) compared to the whole subgroup (M: 1.0).
The fragility and extra need for attention in the oldest age group (≥75 years) should be acknowledged in the treatment and aftercare of ankle and hip fracture patients.
Regarding EQ-VAS scores, our results were higher compared to population scores (“65–74”: Our study: 85, German: 69, French: 68, and Dutch: 78) and (“≥75”: Our study: 77.5, German: 61, French: 62, and Dutch: 73). A possible explanation is that the index provides concrete questions, whereas the EQ-VAS score is more open to variation. Other contributing factors (e.g., socio-economic factors) seem to be accounted for in the EQ-VAS. In this study, a significant difference in EQ-VAS scores between fracture locations was found when analyzing the whole study population.
Our PS scores seemed high compared to previous literature.16,26 However, earlier studies showed differences in study setting and population. PS is known to be a difficult concept which has not yet been clearly defined. 27 We defined it as satisfaction with treatment outcome only. Other studies on PS showed positive effects of managing patient expectations, and this may be applied in the treatment of LEF.25,28 In addition, several studies show added value of a psychological intervention in the aftercare of a hip fracture to improve PS and QoL.24,29 The implementation of a study nurse, who visited patients with information on bone health and osteoporosis may have attributed to our high PS scores.
Remarkably, hip fracture patients only received 18 PT sessions, while they were the oldest and scored lowest on all QoL domains. To improve functional and QoL outcomes, intensive, progressive, and prolonged (home) rehabilitation is recommended after hip fracture as well as a fall prevention program.30,31 According to the literature, it can be assumed that 48–80 supervised training sessions are needed in hip fracture patients to effectively improve activity of daily life–related outcomes and QoL. Our results exhibit a discrepancy in evidence-based recommendations and its lack of implementation into clinical practice.31,32 In accordance with previous research, our study shows that hip fracture patients received the most balance, gait, and strength training of the lower limb.32,33 Strength training of the lower extremities was performed in 84.2% and balance training in 73.2% of the patients. This shows that recommended, important determinants of effective hip fracture rehabilitation are implemented in most cases. Nevertheless, strength and balance training are feasible for almost all hip fracture patients.31-33 Increasing the proportion of patients undertaking strength and balance training should be further focused on. Despite the recommendation of prolonged training after hip fracture (a year or even more), one year after fracture, home exercises were more prevalent in patients with a humerus fracture than in hip fracture patients. 30
Multidisciplinary care pathways like the one in this study have become increasingly popular over the past years and are effective in bettering (objective) outcomes.34,35 Whilst such care pathways for hip fractures are well defined, it has been stated that fractures around the ankle are as devastating but largely overlooked, even though they are the third most common fracture location and with studies indicating a rising incidence and severity as well as worsening of functional outcome with age.36-39 This study also found low QoL outcomes in ankle fracture patients and therefore, we encourage future studies to establish evidence-based treatment recommendations.
This study has limitations. First, a possible selection bias because it contained patients who were living independently at home, which may have caused the study cohort to be a relatively healthy and young representation of the population. This could have attributed to higher QoL outcomes as compared to outcomes of other studies and needs to be considered in the comparison and interpretation of the results. Second, an observer bias may have occurred. We tried to minimize this by using validated instruments. Oral instructions and training on conducting interviews were provided to ascertain that outcomes were as uniform as possible. PS was deliberately measured without validated instruments. Since most studies on PS also use numeric rating scales, we considered it the most practical measurement to compare results. Third, we did not have normative QoL data for the Swiss population so our observations may be partly attributed to the differences between countries. In addition, we subcategorized our data according to age. However, this caused the subgroups to have relatively small sample sizes which lower the generalizability of the outcomes. Fourth, the response rate of this study was 50%, which we consider acceptable since previous studies show similar response rates.40,41 Finally, no baseline QoL scores were reported; wherefore, it became impossible to study possible changes in QoL over the follow-up period.
Conclusion
One-year after LEF, patients’ QoL in this study was considered comparable to the normal population. However, in hip fracture patients QoL-index was markedly lower compared to the whole study group, and these patients reported lowest PS scores. Compared to humerus or wrist fracture patients, hip and ankle fracture patients, especially those aged over 75 years, seem to have a higher risk of loss of QoL.
The fragility and extra need for attention in hip fracture patients and in ankle fracture patients ≥75 years should be acknowledged in their treatment and aftercare. To avoid detrimental loss of QoL, frequent physiotherapy sessions should belong to the comprehensive management of these vulnerable patients. We therefore recommend incorporating an intensive progressive rehabilitation program, including strength and balance training, in the aftercare of hip fractures. Furthermore, hip fracture patients should be encouraged to perform tailored home exercises on a daily or weekly basis for a long period (1 year) or even continually. Regarding the comprehensive management of elderly ankle fracture patients, future studies are needed to establish evidence-based recommendations for the best treatment modalities.
Based on our findings, we believe that population-based research on Swiss normative data for the EuroQol-5D-3 L would be highly valuable.
Supplemental Material
sj-pdf-1-gos-10.1177_21514593211046407 – Supplemental Material for The Quality of Life, Patient Satisfaction and Rehabilitation in Patients With a Low Energy Fracture—Part III of an Observational Study
Supplemental Material, sj-pdf-1-gos-10.1177_21514593211046407 for The Quality of Life, Patient Satisfaction and Rehabilitation in Patients With a Low Energy Fracture—Part III of an Observational Study by Puck C. R. van der Vet, Jip Q. Kusen, Manuela Rohner-Spengler, Bjoern-Christian Link, Egbert-Jan M. M. Verleisdonk, Matthias Knobe, Christoph Henzen, Lukas Schmid, Reto Babst and Frank J. P. Beeres in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Author contributions
Conceptualization: RB, CH, FB, MR-S, LS, MK, E-JV, B-CL, Pv, JKData curation: Pv, MR-S, JKFormal analysis: Pv, MR-S, FBInvestigation: Pv, MR-S, JKMethodology: Pv, JKProject administration: MR-S, FBResources: FB, MR-SSupervision: FB, MR-S, B-CL, MK, RB, CH, LS, E-JVValidation: Pv, MR-S, FBVisualization: Pv, MR-SWriting—Original draft: Pv, JK, MR-S, FBWriting—Review and editing: Pv, M. R-S, FB, E-JV, B-CL, MK, RB, CH, LS
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The Regional Ethics Committee of the Canton of Lucerne approved this study. All participants gave written informed consent before data collection began.
Informed consent
Informed consent was obtained from all patients for being included in the study.
Human rights statements
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and its later amendments.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.