
Abstract
Introduction:
Geriatric patients represent 14% of acetabular fractures and are the fastest growing subset of patients affected by this injury in the US. Treatment outcomes have been reported as inferior to those achieved in younger patients after high-energy (HE) acetabular trauma. This study aimed to compare detailed demographic characteristics and clinical outcomes in elderly patients (≥65 years of age) treated in a tertiary North American trauma center for acetabular fractures after both high- and low-energy mechanisms of injury.
Methods:
Patients (≥65 years of age) diagnosed with an acetabular fracture were identified over a 7-year period. Patient and injury characteristics were extracted from our institutional trauma database. Length of stay, intervention, operative details, disposition, complications, readmissions, and mortality were analyzed.
Results:
One hundred nine patients were identified for inclusion. Low-energy mechanisms (simple falls) were found in 64 (58.7%) and HE mechanisms in 45 (41.3%) patients. The HE cohort was younger (74.6 vs 80.7 years; P < .001), had a higher male predominance (76% vs 56%; P = .10), a lower Charlson comorbidity index (1.29 ± 1.49 vs 2.16 ± 1.76; P = .01), and a higher injury severity score (19.90 ± 15.33 vs 6.46 ± 3.57; P < .001). Fracture patterns, described according to the Letournel-Judet classification, were similar between the 2 groups. Thirty-day mortality was significantly higher in the HE group (26.7% vs 3.1%; P < .001); however, the 1-year mortality rates were not statistically different (31.1% vs 25.0%; P = .20).
Discussion:
Patients with acetabular fractures sustained due to HE accidents demonstrate significantly higher 30-day mortality rate than patients with low-energy fractures, but similar mortality 1 year after the injury, despite having a much lower mean age and fewer comorbidities.
Conclusion:
Medical efforts made during initial hospital admission may have the biggest impact on survivorship following acetabular fracture.
Introduction
While geriatric patients represent only 14% of acetabular fractures, it is the fastest growing subset of those affected by this injury in the United States. 1,2 Outcomes of treatment have been reported to be inferior to those achieved in younger patients after high-energy (HE) acetabular trauma. 3 These findings necessitate the need to learn about acetabular fractures among elderly patients to adequately meet their medical demands in the coming decades. 4 -8
Early research on geriatric acetabular trauma focused on descriptive epidemiological studies; however, publications that are more recent have concentrated on detailed, in-depth characterization of the injuries. 9 Even though geriatric acetabular fractures were initially assumed to be a product of low-energy (LE) mechanism of impact (by analogy to periarticular and spinal fractures related to senile osteopenia), it became obvious that HE accidents could also involve elderly patients due to increased life expectancy and prolonged physical activity. Several authors have referenced the paucity of information on HE skeletal trauma in the elderly. 8,10,11 Indeed, a recent review highlighted the lack of information on this increasingly important injury. 1,12
Indications for nonoperative versus operative treatment in geriatric patients are still poorly defined. Common consensus exists that fractures with posterior hip instability should be addressed surgically; however, more frequent patterns with anteromedial displacement may be amenable for nonoperative management. 9 Nevertheless, nonoperative treatment often leads to inadequate reduction, and operative outcomes, even when improved techniques are used, are still worse than those of younger patients. 3,9,13 -22
Therefore, the purpose of this study is to compare detailed demographic characteristics and clinical outcomes in elderly patients (≥65 years of age) treated in a tertiary North American trauma center for acetabular fractures after both HE and LE mechanisms of injury.
Methods
After institutional review board approval, all patients (≥65 years of age) who had been diagnosed with an acetabular fracture were identified from our institutional trauma database over a 7-year period. Periprosthetic acetabular fractures in patients with hip arthroplasties were excluded, as were pelvic ring injuries including pubic root fractures. Patient and injury characteristics were extracted from the database. These included age, sex, comorbidities, mechanism of injury, fracture classification, injury severity score (ISS), associated injuries, length of stay (LOS), intervention, type of fixation if applicable, ambulatory status, disposition, 1-year readmission rate, complications at 30 days and 6 months, and mortality at 6 months and 1 year. If the patient underwent operative treatment, time from injury to surgery, American Society of Anesthesiologists score, operative length, intraoperative blood loss, surgical approach, and type of fixation were all recorded. If the patient underwent nonoperative management, the reason for this decision was also extracted from the provider notes.
Patient comorbidities were classified according to the Charlson comorbidity index. 23 Preinjury habitation status was assigned as home or long-term care (LTC) facility. Mechanism of injury was classified as motor vehicle accident (MVA), low fall, high fall, assault, bicycle accident, pedestrian trauma, or crush injury. A low fall was defined to be any fall less than 6 ft, while a high fall was defined as any fall occurring from a height over 6 ft. If this was not distinguished from the provider notes, the injury was considered a low fall. Associated injuries were classified anatomically according to the methodology of the abbreviated injury scale. 24 The injury severity of each patient was calculated using the ISS. 25 Radiographs were evaluated to classify fracture type according to the Letournel-Judet classification. 26,27
The postintervention ambulatory status of the patient was classified as nonambulatory, ambulatory with assistance, or no assistance necessary. The postintervention disposition was classified as LTC, transitional care unit, home, or rehabilitation. Patient mortality information was identified through the medical chart review, a search of the obituary index, and/or search of the social security index. The patient was believed to be living if there was no indication of death by any of these sources.
After all patient data were entered into a centralized database (Microsoft Excel, Redmond, Washington), patients were stratified into either HE or LE trauma categories. Statistical analysis was performed to compare the HE and LE patient populations. The Fisher exact test was used for all binary comparisons and the Mann-Whitney U test was used for all ordinal or continuous variables. Significance was set at P < .05.
Results
Patient Characteristics
One hundred nine patients were identified and included in the study. Low-energy mechanisms (simple falls) accounted for the acetabular fractures in 64 (58.7%) patients and HE mechanisms (eg, motor vehicle crash, high falls, motorcycle) were responsible for the fractures in 45 (41.3%) patients (Table 1). The majority of the patients in the LE group sustained injuries from low falls, 63 (98.4%), whereas mechanisms of injury in the HE group were more diverse including 19 (42.2%) MVAs, 12 (26.7%) high falls, and 6 (13.3%) pedestrian versus car accidents. The 2 groups were distinctly different with respect to the baseline demographics. The HE cohort was younger (74.6 vs 80.7 years; P < .001), had a higher male predominance (76% vs 56%; P = .10), had a lower Charlson comorbidity index (1.29 ± 1.49 vs 2.16 ± 1.76; P = .01), more patients lived at home (86.4% vs 69.8%; P = .02), and fewer walked with an assistive devices (4.5% vs 31.3%; P < .001) upon presentation when compared with the LE cohort.
Patient Demographics.
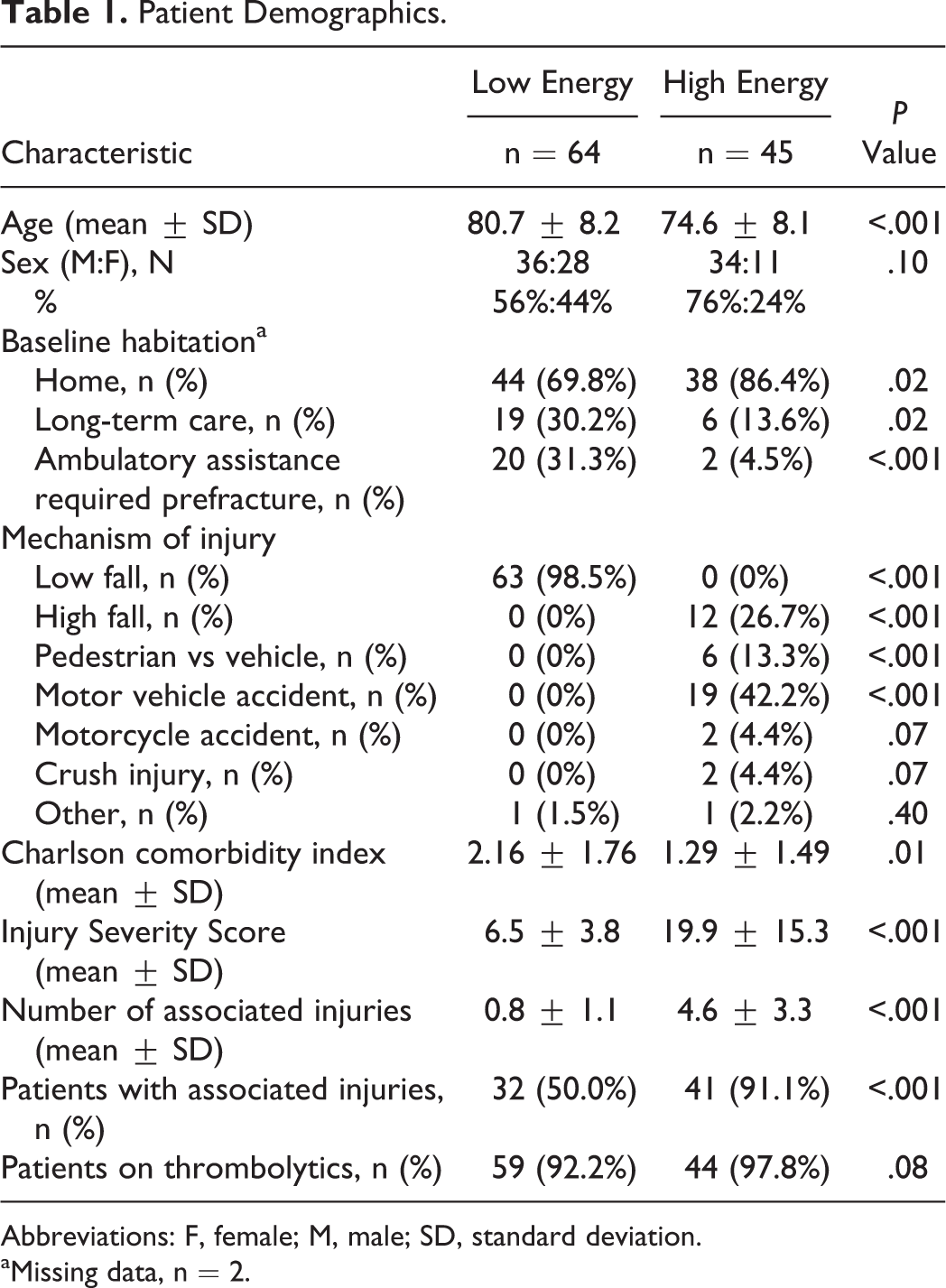
Abbreviations: F, female; M, male; SD, standard deviation.
aMissing data, n = 2.
Injury Characteristics and Radiographic Comparison
The majority of patients in the HE group presented with at least one associated injury (91.1% vs 50.0%) and a higher average number of associated injuries (4.6) compared with the LE group (0.8), P < .001. Injury severity scores were considerably higher, as well (19.9 ± 15.3 vs 6.5 ± 3.6; P < .001). In the HE group, abbreviated injury scores were highest for the pelvis followed by chest, head, abdomen, and extremities.
Interestingly, the fracture patterns, described according to the Letournel-Judet classification, 26,27 were similar between the 2 groups (Table 2), with the preponderance of patients sustaining acetabular fractures including the anterior column (26.6%). Approximately half of patients in each group had fractures crossing both anterior and posterior columns.
Fracture Classifications.

Abbreviations: ABC, Associated Both Column; ACPHT, anterior column/wall with Posterior Hemitransverse; AC,Anterior Column; AW, Anterior Wall; PW, Posterior Wall; PCPW, Posterior Column/Posterior Wall; PC, Posterior Column; Trans, transverse; TransPW, transverse posterior wall.
Management Comparison
A large number of patients in the entire cohort were treated nonoperatively (n = 66/109, 60.6%); however; in the HE group, a greater percentage of patients received an operative intervention (51.1% vs 31.3%; P = .02; Table 3). Treatment for the HE group consisted of open reduction and internal fixation (ORIF) in 18 (40.0%) patients, minimally invasive osteosynthesis (MIO) in 3 (6.7%) patients, combined ORIF with total hip arthroplasty (THA) in 2 (4.4%) patients, or nonoperative management in 22 (48.9%) patients, including those who died before treatment could be rendered (n = 12, 26.7%). For the HE patients treated nonoperatively, 10 (45.4%) of 22 patients were deemed to have a nondisplaced/stable fracture pattern and, therefore, treated with toe-touch weight bearing or weight bearing as tolerated. However, the remainder of the nonoperatively treated patients in this cohort (n = 12/22, 54.5%) were not taken to surgery because the surgeon did not feel that the patients could withstand the surgical insult related to preexisting medical comorbidities or due to the severity of their associated injuries.
Outcomes.
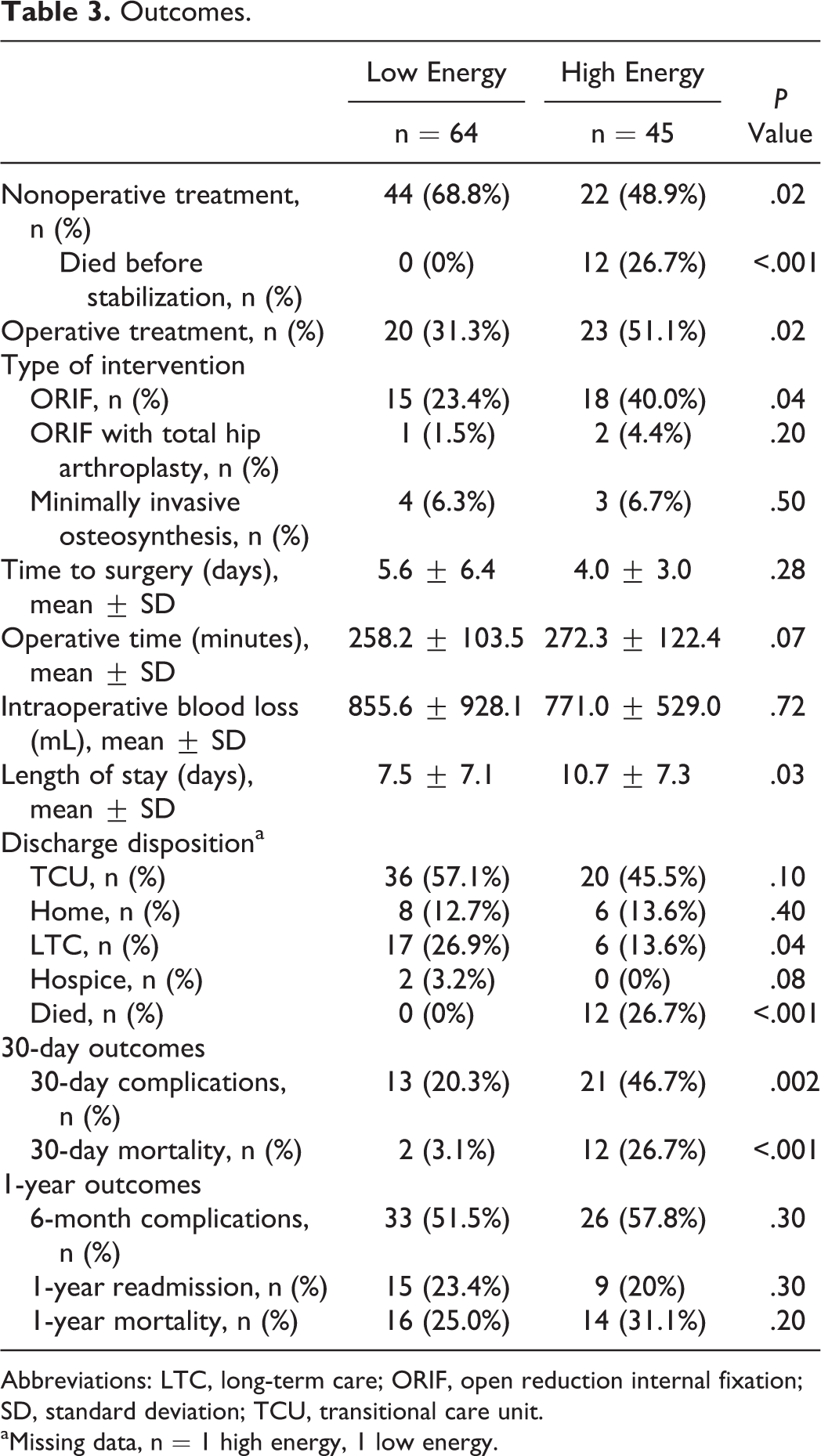
Abbreviations: LTC, long-term care; ORIF, open reduction internal fixation; SD, standard deviation; TCU, transitional care unit.
aMissing data, n = 1 high energy, 1 low energy.
For the LE group, the treatment consisted of ORIF in 15 (23.4%) patients, MIO in 4 (6.3%) patients, combined ORIF/THA in 1 (1.5%) patient, or nonoperative management in 44 (68.8%) patients. Patients treated nonoperatively because they were believed to be too fragile for surgery included 14 (31.8%) of the 44 in the LE cohort. Other reasons for nonoperative treatment included nondisplaced/stable fracture patterns in 22 (50%) patients and secondary congruence of the femoroacetabular articulation in 6 (13.6%) patients with associated both column fractures and they were allowed to bear weight as tolerated.
Very few patients (n = 5, 7.8%) required admission to the intensive care unit (ICU) in the LE cohort. The average total hospital LOS in the LE group was 7.5 days (standard deviation [SD]: 7.1). Conversely, 24 patients (53.3%) of the HE group were admitted to the ICU and the average total LOS extended to 10.7 days (SD: 7.3). This difference was significant (P = .03). Complications were significantly higher in the HE cohort within the first 30 days as well (46.7% vs 20.3%; P = .002).
Mortality
Thirty-day mortality (26.7% vs 3.1%; P < .001) was significantly higher in the HE group; however, the 1-year mortality rates (31.1% vs 25.0%; P = .20) were not found to be statistically different between the 2 groups. Of the 23 patients in the HE cohort who underwent operative management, the 1-year mortality rate was only 8.6% (n = 2 patients). In the LE cohort, patients who were not taken to surgery due to medical comorbidities or because they were not stable for surgery had an extremely high 1-year mortality rate. Forty-three percent (N = 6/14) of these patients died within 1 year.
Discussion
It is clear that HE geriatric acetabular fractures are a unique type of injury and pose a challenging conundrum in the field of orthopedic trauma. One potential source of improvement in the management of these injuries is a more specific and nuanced characterization of these fractures. Given that the literature indicates HE and LE geriatric acetabular fractures are distinct entities, medical and surgical management will be different in each case. Better characterization of the differences between HE and LE acetabular fractures in the elderly increases the chances of finding opportunities for improved management strategies and better outcomes. There is only one study to date that directly compared demographics and short-term clinical outcomes between geriatric patients with acetabular fractures after LE and HE mechanisms of trauma. 28 The authors demonstrated that patients with LE acetabular fractures were older, sicker, and thinner, were less likely to receive surgical treatment for their injuries, and had longer admission lengths than their counterparts with HE mechanisms. The authors confirmed dominance of anterior column involvement in geriatric patients regardless of the mechanism of injury. Even though general comparison of 2 groups was made, detailed characteristics of injury such as severity of the trauma, rehabilitation, ambulatory status, and long-term mortality were not provided. Applicability of the Korean patient population to the US population also remained unclear due to possible differences in levels of activity and expectations in cultural and socioeconomic environments. 29
This study compared demographics and clinical outcomes between elderly patients with acetabular fractures due to HE and LE mechanisms of injuries. It was found that 1-year mortality rates among those patients were similar; however, HE fractures were associated with significantly higher 30-day mortality rate. The significance of these findings is that the biggest impact on survivorship after geriatric acetabular injuries can be made in the acute posttraumatic period of care. The majority of previously published studies has focused on relationship between outcomes of geriatric acetabular fractures and treatment algorithms, but not by force of impact; therefore, direct comparison of patients 65 years and older with acetabular fractures distinguished from each other by energy of injury, was justifiable to access, and compares clinical outcomes.
This study is the first attempt to compare long-term outcomes of treatment of geriatric acetabular fractures in the US population. Results of our study confirmed that patients with HE fractures are younger, more active, and healthier, with male predominance than those with LE fractures. A different level of activity between groups also resulted in dissimilar mechanisms of injury with ground-level falls and high-speed MVAs dominating correspondingly among patients with LE and HE injury patterns, respectively. This study confirmed that more than 50% of elderly patients required nonoperative treatment regardless of mechanism of injury; however, this statement should be approached with caution because in many cases, the decision-making was affected by subjective assessment of general medical fitness of the patients by an attending surgeon. In as much as 26.7% (n = 12/45) of patients with HE fractures and 21.8% (n = 14/64) of patients with LE fractures, nonoperative treatment was chosen because the patient was felt to be too fragile to withstand stress of surgery. Although there were different surgeons assessing fitness for surgery or not, the results are from the same institution and trauma service (and surgeons) throughout this period.
Fracture patterns in geriatric patients were well described in previous studies. 1,2,5,30 This study confirmed that both HE and LE mechanisms also resulted in similar fracture pattern with involvement of the anterior column and a predominance of associated both column fracture patterns regardless of the mechanism of injury.
Mortality rates for the combined cohort of geriatric patients with acetabular fractures were reported to vary from as low as 16% to a soaring 79% 1 year after injury. 1,14 Even though some authors thought that higher mortality was associated with surgical treatment of the fractures, recent studies proved that mortality is mostly influenced by general medical condition of the patients including medical comorbidities and magnitude of sustained injuries. 14,17,20,21,31 Thirty-day mortality rate in this study was 9 times higher among patients with HE acetabular fractures (26.7% vs 3.1%, P < .001); however, 1-year mortality rates were not significantly different between groups (P = .20). These findings were opposite to the results, obtained among the Korean patients with LE and HE acetabular fractures by Kim et al, where in-hospital mortality rates were similar between groups. 23 Even though demographics and comorbidity parameters were comparable between studies, the HE cohort in this study was characterized by significantly higher ISSs and magnitude of associated injuries, which echoed on higher mortality rates among HE patients. Longer hospital stays and higher rates of admission to the ICU among patients with HE fractures serve as a reflection of higher morbidity, associated with HE acetabular fractures. One-year mortality rates similar for patients, affected by LE and HE fracture mechanisms, confirm results of other studies, where once the patient makes it out of the hospital, further mortality was mostly influenced by general medical status of the patient due to preinjury comorbidities and results of impact of the injury. 1,14,32 Given that the 30-day mortality rate was higher in the HE acetabular group, we want to make clear that this likely results from other factors besides the fracture itself, something implied by the 40% lower difference in associated injury rate and 13 point lower ISS score in the LE group.
Limitations of this study include retrospective design, relatively small cohort size, lack of patient-derived outcome measures included in the study, and allocation of all patients to a single major trauma US center, which can make extrapolation of the results difficult to smaller hospitals. Potential selection bias may also be introduced by the lack of formal treatment algorithms for geriatric acetabular fractures and subjective selection of a treatment approach by an attending orthopedic surgeon. In addition, we have not performed a detailed fracture analysis, beyond pattern. These fracture parameters would likely be useful assessment of variables affecting functional outcome, rather than 30-day or 1-year mortality measures. Further study into fracture characteristics and its impact on decision-making will make for a good future analytics.
Conclusion
In summary, geriatric patients with acetabular fractures, sustained due to HE accidents, demonstrate significantly higher 30-day mortality rate than patients with LE fractures, but similar mortality 1 year after the injury, despite having a much lower mean age (74.6 ± 8.1 vs 80.7 ± 8.2 years, P < .001) and health (Charlson comorbidity index 1.29 ± 1.49 vs 2.16 ± 1.76, P = .01). Based on the findings of this study, medical efforts made during initial hospital admission after the injury may have the biggest impact on survivorship following acetabular fracture injuries.
Footnotes
Acknowledgments
The authors would like to acknowledge David Wright, MD, and Matthew Molcjan, BS (in memoria), for their dedicated support of the project through various stages of study application, data collection, and summarization of the report. Without these individuals, this project would not have been completed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.