
Abstract
Introduction
This study compared the clinical and radiologic outcomes of screw-tip augmented locking plate osteosynthesis (STA) vs primary reverse total shoulder arthroplasty (RSA) in elderly patients with displaced proximal humeral fractures.
Methods
60 patients (age >65 years) with a displaced proximal humeral fracture underwent open reduction and internal fixation with locking plate and fluoroscopy controlled screw-tip augmentation. Sixty matched individuals (age, gender, fracture pattern, and mean follow-up) treated by RSA for fractures were identified from the institutional database and outcomes as well as occurring complications and need for revision surgery were compared.
Results
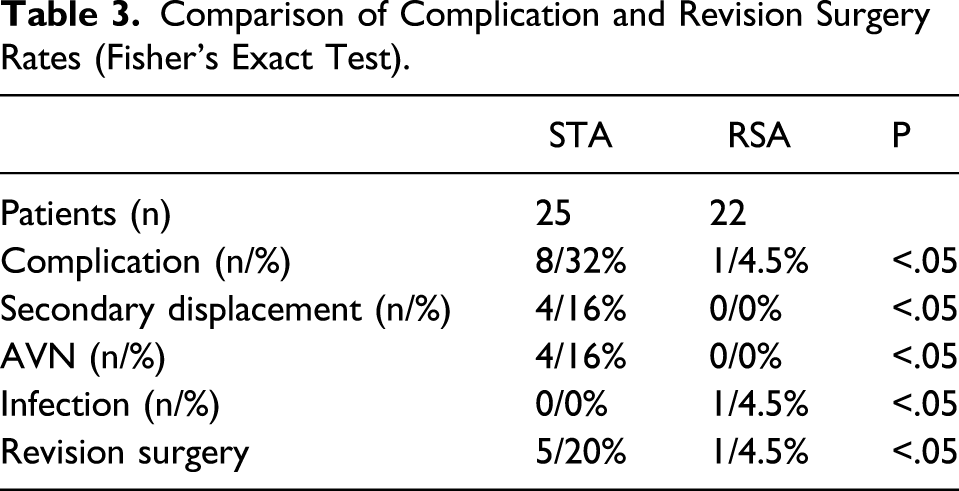
At 39 months’ follow-up, 25 patients in the STA group (mean age 74.5 ± 12 years, 76.7% woman) showed a mean Constant Score (CS) of 68 ± 18.8 points. Mean %CS compared to the contralateral side was 81.6 ± 19.8%. Of 60 matched individuals in the RSA group, 22 patients (mean age 78.9 ± 8.2 years, 76.7% woman) showed a mean CS of 60.6 ± 21.2 points (P = .33), and the mean %CS compared to the contralateral side was 81.6 (74.7 ± 18.6)% (P = .14). The overall complication rate in STA group was 32% (secondary varus or valgus displacement >10°, n = 4, avascular necrosis, n = 4). In RSA group, the overall complication rate was 4.5% (P = <.05). We observed one early onset infection. Revision surgery with removal of the prosthesis and PMMA spacer implantation for two-stage revision was necessary. The follow-up rate was 41.7 vs 36.7%.
Conclusions
Screw-tip augmented locked plating and reverse total shoulder arthroplasty result in comparable satisfying functional outcome 3 years following a displaced proximal humeral fracture in elderly patients. However, we noted a higher complication and revision rate in the STA group. In contrast, primary reversed shoulder arthroplasty resulted in a lower rate of complications and revisions, which may be beneficial in elderly patients.
Keywords
Introduction
Due to demographic change, the incidence of proximal humeral fractures (PHFs) is expected to rise in the future while accounting for five percent of adult fractures today.1-3 Non-operative management of undisplaced and stable fractures proved good clinical results. 4 In contrast, displaced and complex fractures indicate for operative treatment. Locking plates have been established as the working horse for open reduction and internal fixation in order to restore shoulder function. 5 However, due to reduced bone quality in elderly patients, complications (ie, secondary displacement and screw cutout) are observed frequently.6-9 In a publication by Jost et al., 10 63% of patients with complications after ORIF had a malunion, 13% had a nonunion, 12% had a primary screw cutout, and 5% had an infection. Therefore, some authors recommend primary fracture arthroplasty for the treatment of displaced proximal humeral fractures. 3 Improved implant design and advancement of surgical technique with introduction of eccentric glenospheres and lateralization reduced the number of secondary humeral notching after reverse total shoulder arthroplasty and raised the survivorship of the arthroplasty to 90% at 10 years.11,12 In elderly patients, reverse total shoulder arthroplasty (RSA) has therefore replaced hemiarthroplasty regarding quantity of carried out procedures.13,14
In osteoporotic bone, open reduction and internal fixation is associated with an immense complication rate (secondary dislocation, screw cutout, and avascular necrosis). One technical approach to address this problem is synthetic augmentation of osteosynthesis by use of bone cement (PMMA = polymethylmethacrylate) or calcium phosphate to increase fixation strength. By using cannulated screws, cement augmentation thereby expands the interface between bone and screw tip, potentially supporting fixation strength. While there are several biomechanical studies, showing an increase of fixation strength, data on functional outcomes and complications following screw-tip augmentation of locked plating in displaced proximal humerus fractures are still rare.8,15-20 From our view, there are mainly three options in elderly patients with reduced bone quality: closed reduction and humeral nailing, open reduction and internal fixation using cement augmented screws in locked plating, or reverse total shoulder arthroplasty.
The aim of the study was therefore to evaluate outcomes and complications following screw-tip augmented locking plate osteosynthesis (group STA) of displaced proximal humeral fractures and compare the results to patients treated by reverse total shoulder arthroplasty (group RSA). It was hypothesized, that complications would occur less frequent in the group of reverse total shoulder arthroplasty compared to screw-tip augmented locking plate osteosynthesis and the functional outcome would be comparable.
Material and Methods
Study Cohort and Data Collection
Sixty patients with displaced (>1 cm, 45° angulation) PHFs were prospectively enrolled into this study between April 2014 and October 2016. Inclusion criteria of this review board-approved study were patients older than 65 years and a minimum follow-up of 2 years. In all cases, fracture pattern was classified by x-ray (true anteroposterior and outlet view radiographs) as well as CT scans. Fractures were classified according to Neer and Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) classifications.21-23 Exclusion criteria were isolated fractures of the greater or lesser tuberosity, open fractures, pathologic fractures resulting from metastatic or primary neoplasia, preoperative non- or malunion of a former fracture, revision surgeries, primary infections, and preoperatively diagnosed neurological deficiency (lesions of the axillary or radial nerve, distinct dementia, condition after apoplectic insults, and consecutive hemiparesis concerning the corresponding extremity).
To each of the 60 patients treated by STA locked plating, a matched individual patient was identified from our institutional database that had been treated for a displaced PHF by RSA between 2006 and 2016. Matching was related to age, gender, and fracture pattern. Follow-up and rehabilitation protocol did not differ from the original study group. Thus, the group of 60 patients treated by STA locked plating was compared to a group of 60 patients treated by RSA.
Surgical Procedure
Timing of surgery was within 8 days of the traumatic incident as first-line therapy by open reduction and internal fixation (ORIF) by one of two experienced trauma surgeons. Under general anesthesia, in combination with an interscalene block for perioperative pain management, every patient received prophylactic intravenous antibiotics (1.5 g cefuroxime or 3 g Unacid® = 1 g sulbactam/2 g ampicillin, or 600 mg clindamycin® for patients with known penicillin allergy) as a single-shot at beginning of the surgery in beach chair position. Via a standardized deltopectoral approach, open reduction and internal fixation removed humeral offset and restored the head-shaft angle as well as the position of the greater and lesser tuberosity. In all cases, a proximal humeral interlocking plate system (PHILOS®, DePuy Synthes GmbH, Zuchwil, Switzerland) was used. The rotator cuff was evaluated for tears and when necessary tuberosity sutures (FiberWire No. 5®; Arthrex Inc., Naples, FL, USA) were used. Following accurate fracture reduction, 6 locking screws were carefully driven until approximately 5 mm from the subchondral layer under fluoroscopic evaluation to assure correct screw length and not to penetrate the articular surface of the humeral head. Screws were repositioned to obtain the intended distance and location of the screw tip relative to the subchondral bone layer when necessary. Three bicortical screws were inserted to fix the plate against the humeral shaft.
Screw-Tip Augmentation
As described previously, screw-tip augmentation was indicated on preoperative and intraoperative signs of poor bone quality (T-score < −2.5 in performed dual-energy x-ray absorptiometry, FRAX score, or deltoid tuberosity index <1.4).18,24,25
After careful evaluation of the intended screw position, 3–4 screws were changed to cannulated screws with identical screws’ length. In all cases, the screws of the top row (line A) were changed to cannulated screws; additionally, either both screws of the third row (line C) or the center screw (#7, line D) was exchanged (see Figure 1). Before beginning with screw-tip augmentation, screw lengths were controlled under image intensifier control in full range of glenohumeral motion. To avoid potential leakage into the fracture or joint, .5–1 ml radiographic contrast agent was applied. After securing not to penetrate the fracture or joint under image intensifier, the contrast agent was injected. If the contrast agent could not be injected, the screw cannulation was cleared by probing a 1.6 mm k-wire via the cannulated screw. Saline solution was injected to wash out the agent from the humeral head if the contrast agent led to inappropriate visualization. If contrast agent leaked into the joint or fracture, alternative screws were chosen and replaced by cannulated screws. If less than four screws could be augmented, it was secured that at least six screws secured the humeral head. When evaluation proved absence of leakage, augmentation was then performed using polymethylmethacrylate (PMMA, Trauma Cem V+®, DePuy Synthes GmbH, Zuchwil, Switzerland or Calcium phosphate cement, Quickset™, Arthrex Inc., Naples, FL, USA) through the cannulated screws under image intensifier. A setting time of 15 min was respected. During this time, any movement of the fractured arm of the patient was avoided. Any spilled cement was removed from the screw heads, plate, and soft tissue. After setting of the cement, a final evaluation of screw-tip augmentation was performed under image intensifier in full range of glenohumeral motion. Illustration of lines in PHILOS plate.
Rehabilitation Protocol
The standardized post-surgical protocol allowed passive- and active-assisted rehabilitation exercises on day one after surgery under supervision of the surgeon. All patients received a shoulder sling in the operating room. For the first 6 weeks, abduction and elevation up to 60° without forced external rotation were allowed. The day after surgery x-ray radiographs in true anteroposterior and outlet view were obtained for securing right implant position without loss of fixation before taking active exercises with full range of motion and increasing force.
Follow-Up and Outcome Measures
Patients were followed up in consistency with the Declaration of Helsinki after giving their informed consent. Every patient was both examined by the surgeon and interviewed according to a standardized protocol at every follow-up examination. In the STA group, 14 patients died within the follow-up period, 3 patients sustained apoplectic insult or dementia, and 18 patients were not able to be contacted or examined due to an unknown address or being in a nursing home. Mean follow-up was 40.4 ± 8.6 months (39.5; 28–64 months). Follow-up rate was 41.7% (25 patients).
In the RSA group, 17 patients died within the follow-up period, 2 patients sustained apoplectic insult or dementia, and 17 patients were not able to be contacted or examined due to an unknown address or being in a nursing home. Mean follow-up period was 41 ± 12.2 months (39; 27–68 months) after surgery and follow-up rate was 36.7% (22 patients).
The standardized physical examination included assessment of the Constant Score (CS),26,27 by measurement of strength with a digital spring balance (Burg Wächter 76 000 Tara PS®) in highest possible abduction position and range of motion (=ROM), as well as the %CS as CS in relation to the uninjured contralateral shoulder. Medical records comprised demographic data and x-rays and were prospectively collected in our digital database. The standardized longitudinally follow-up included clinical and radiographic examinations of the affected shoulder 6 weeks, 3, 6, and 12 months after surgery and at 3-year follow-up. We defined 24 months as minimum follow-up for this study.
Radiographic Evaluation
True anteroposterior and outlet view radiographs were assessed in all patients on day one after surgery and at every follow-up. According to Schnetzke et al., quality of reduction was evaluated.9,28 Radiographs were furthermore evaluated for radiographic signs of secondary displacement, loss of fixation, screw cutout, avascular necrosis (AVN) of the humeral head, nonunion, malunion, or failure of the implant (loosening and breakage) as well as notching of the arthroplasty. AVN was evaluated according to Hattrup and Cofield. 29 We defined secondary dislocation as an alteration of the humeral head-shaft angle of more than 10°. 30
Statistical Evaluation and Matched Pair Analysis
Continuous variables (demographic data and functional outcome) were described by means and standard deviation and were compared using the Mann–Whitney Test. Categorical variables (radiographic findings, complications, and revisions) were analyzed using Fisher’s exact test. The level of significance for all testing was set at P <.05. Statistical analysis was performed using SPSS (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, version 24.0. Armonk, NY: IBM Corp.).
Results
Patients Demographics and Fracture Pattern in the Two Study Groups (STA and RSA).

The mean Constant Score (CS) of 25 patients (mean age: 74.5 ± 12 years, 76.7% women) treated by STA locking plate osteosynthesis 40.4 ± 8.6 months after surgery was 68 ± 18.8 for a displaced PHF. The mean %CS compared to the uninjured side was 81.6 ± 19.8. Complications were observed in 8 cases (32%) with n=4 cases of secondary displacement >10° and n=4 cases of AVN. The overall revision rate was 20% (n = 5 patients) with revision osteosynthesis in two cases and screw removal in two cases as well as one case of conversion to RSA.
In the group of matched pair (age, gender, fracture pattern, and follow-up period) individuals treated by RSA, the mean CS was 60.6 ± 21.2 (P=.33). The %CS compared to the uninjured contralateral shoulder was 74.7 ± 18.6. The overall complication rate of matched pair individuals was 4.5%. In one case, an infection was observed and the patient underwent two-stage revision arthroplasty with temporary spacer implantation. We did not see any case with implant failure or notching.
Comparison of the Clinical Results of the Two Study Groups (Mann–Whitney U Test).

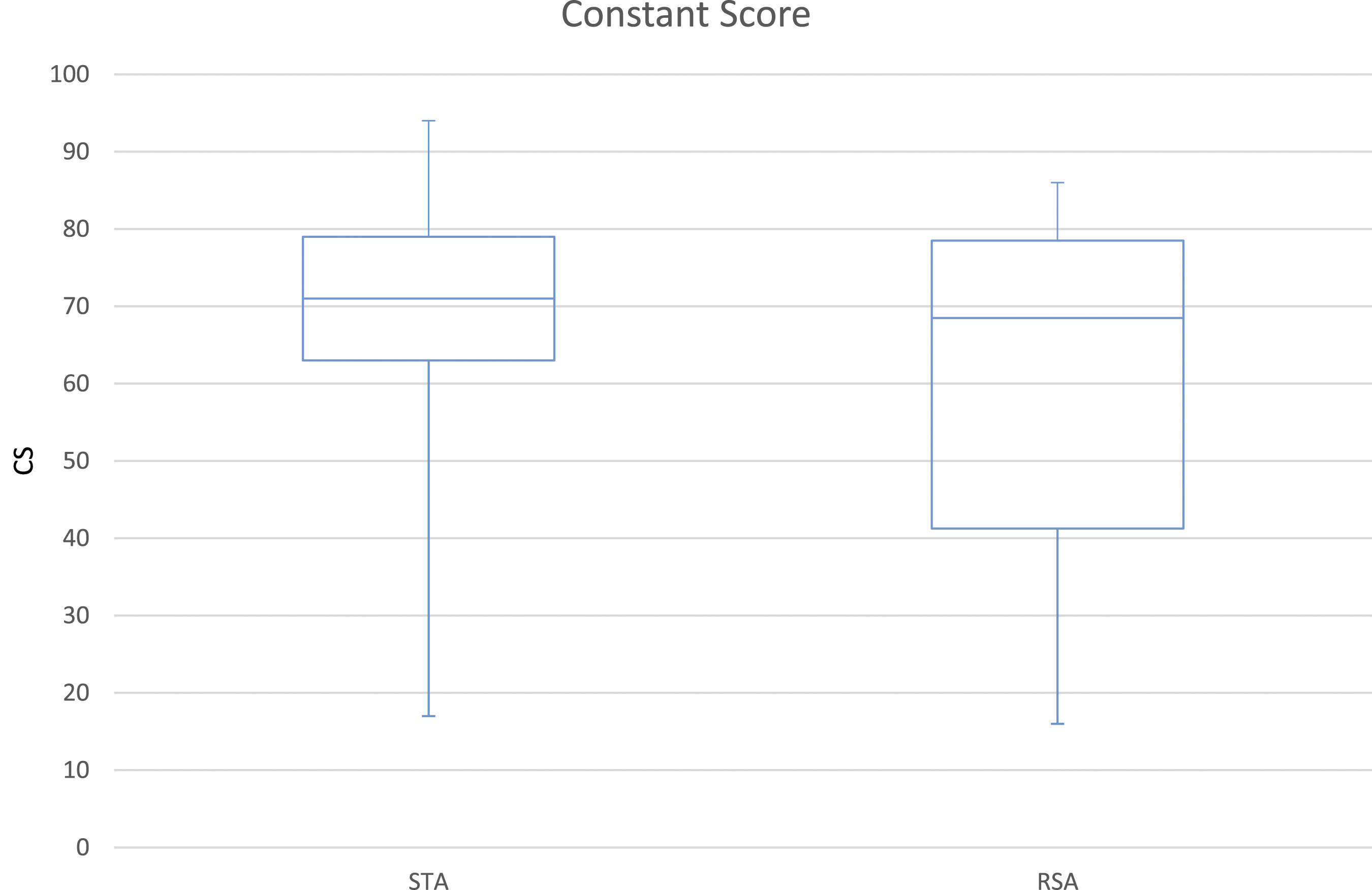
Clinical outcome box plot CS (P>.05).

Clinical outcome box plot %CS (P>.05).
Comparison of Complication and Revision Surgery Rates (Fisher’s Exact Test).
Discussion
While the evidence in literature on augmented locked plating for proximal humeral fractures is increasing, we suggest that this is the first report describing the outcomes and complications following STA locking plate osteosynthesis in displaced PHF in comparison to RSA in a matched pair analysis in a midterm follow-up of approximately three years after trauma.
One main result of this study is that screw-tip augmentation results in satisfying functional outcomes in a selective cohort of predominantly elderly and female patients.
In this study, the mean age of patients was 75 years and 76.7% of the patients were female. This study cohort thus well represents one typical patient with a displaced proximal humeral fracture that is treated by open reduction and internal fixation. While several studies have shown good results for open reduction and locked plating in younger patients, Owsley et al. showed that in patients over the age of 60, 57% of cases show radiographic signs of a complication, such as secondary displacement, screw cutout, and AVN. 31
Synthetic augmentation of osteosynthesis by use of bone cement (PMMA = polymethylmethacrylate or calcium phosphate cement) was introduced, potentially reducing the risk of secondary displacement and screw cutout. It is performed for various indications of fracture treatment, and outcomes are reported promising for the treatment of spine fractures and fractures of the proximal femur.32,33 At the proximal humerus, fracture treatment by PMMA augmented locking plates was proclaimed in order to increase the fixation strength of osteosynthesis. Several biomechanical studies reported less movement at the interface between bone and implant in PMMA augmented locking plate osteosynthesis.15-17,34,35 Schliemann et al. reported in a biomechanical study that the addition of bone cement to augment anteriorly directed head screws reduces motion at the bone-implant interface, thus potentially reducing the risk of secondary displacement. However, until now, there are no data on the clinical outcome and complications of PMMA augmented locking plate osteosynthesis in comparison to reverse total shoulder arthroplasty.
The rate of secondary displacement and AVN was comparable (32%) to studies published before. 10 However, in comparison to other studies, the fracture pattern was different. In the present study, 30% of fractures were two-part surgical neck type fractures and 43.3% were three-part fractures. In turn, four-part and head-split type fractures were represented less frequently, compared to other studies.
In 16% of cases, we observed AVN around PMMA augmented screw tips. Usually being induced by fracture-related compromised blood supply, in our study, AVN may be related to the temperature and pressure reaction associated to PMMA and calcium phosphate cement augmentation. While in vitro studies suggest no harming effects, in vivo studies of the proximal humerus are not present.36,37 However, the results are comparable to the results of other study collectives investigating on AVN following proximal humeral fractures.38,39 We have seen AVN in cases where the cement was filled into the subchondral layer. We therefore suggest that screws’ lengths should be chosen at least 1 cm from the apex (much shorter then without STA, normally 2 mm). In accordance to the surgical technique, we believe that care must be taken not to exceed 1 mL of PMMA around each screw tip and that the cement should be injected with the correct viscosity as we reported before.
The other main result is that RSA leads to comparable functional outcome with lower complication rates and rates of revision surgery needed. RSA for displaced PHFs may be advantageous for elderly patients to stay independent in their daily activities and reduce revision rate in complex fracture pattern.
The results of this study have to be seen in the light of its limitations. Although this is a prospective cohort study of 60 consecutive cases, the treating surgeon individually took the decision for STA or RSA.
Fracture patterns were distributed differently in STA and RSA groups. While lesser complex fracture patterns were represented more frequently in the STA group, the RSA group comprised more complex multifragmentary fractures as well as head-split fractures.
Therefore, this study may not conclude on differences and similarities in both groups for all fracture patterns. Due to risks of cement leakage and an otherwise complicated outcome due to severe AVN, screw-tip augmented locked plating may not be a good indication in elderly patients with four-part or head-split type fractures. However, screw-tip augmentation may result in satisfying functional outcomes in mainly two-part and three-part fractures of the proximal humerus in an orthogeriatric cohort of patients but lower complication rates and comparable outcome for RSA.
Another limitation is the follow-up period of 3 years which may be too short to judge on the long-term outcome and complications, specifically on the presence of AVN or loosening of the prosthesis. While this is the first study upon the subject, further studies with randomized inclusion and decision of treatment as well as longer follow-up periods are necessary.
Conclusion
Screw-tip augmented locked plating and reverse total shoulder arthroplasty result in comparable satisfying functional outcome 3 years following a displaced proximal humeral fracture in orthogeriatric patients. However, we noted a higher complication and revision rate in the STA group. In contrast, primary reversed shoulder arthroplasty resulted in a lower rate of complications and revisions, which may be beneficial in elderly patients.
Footnotes
Author Contributions
Siebenbuerger G and Ockert B contributed to this manuscript: study design, data collection, data analysis, and writing of the manuscript.Fleischhacker E and Helfen T contributed to this manuscript: data collection, literature research, and data interpretation.Stumpf U and Böcker W contributed to this manuscript: study protocol, data analysis, and critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Certificate of the ethical review board/IRB, Ethical Committee Approval: Ethikkommission bei der LMU München, Pettenkoferstr. 81, D-80336 München, Germany, study number: 156-12.