
Abstract
Background:
Acute lymphoblastic leukemia (ALL) is reported to be the most common malignancy in children, but is less common in adults. Though vertebral compression fractures have been reported as initial signs of ALL in children, to the best of our knowledge, there have not been any previous reports of vertebral compression fractures as an initial manifestation of ALL in elderly people.
Case Presentation:
Here we reported a 65-year-old man who was admitted with a 1-month history of progressive chest and back pain and worsening pain after heavy lifting. Considering the histories of osteoporosis, minor trauma and normal peripheral blood counts, it was firstly misdiagnosed as spinal osteoporotic compression fractures which were caused by low-energy injuries. The patient was definitely diagnosed as ALL after bone marrow biopsy.
Conclusion:
ALL must be considered in the differential diagnosis with acute vertebral compression fracture. Considering that bony lesions may precede clinical findings, knowledge of radiographic and orthopedic appearances of leukemia are important in order to initiate earlier treatment to avoid the progressive damage and improve their survival rates. we recommend bone marrow biopsy in vertebroplasty to avoid misdiagnosis.
Keywords
Introduction
As a malignant hematologic disease, acute lymphoblastic leukemia (ALL) is reported to be the most common malignancy in children, but is less common in adults. 1 Previous study showed the age-adjusted incidence rate was 1.6 per 100,000 individuals per year, with a median age of 14 years and almost 60% of the patients were diagnosed before 20 years of age. 2 Clinical presentation of adults with ALL usually involves symptoms of lymphadenectasis, infections, anemia, pallor, bleeding, and bone pain. 3
Though vertebral compression fractures have been reported as initial signs of ALL in children 4 -6 and middle-aged, 7 -9 to the best of our knowledge, there have not been any previous reports of vertebral compression fractures as an initial manifestation of ALL in elderly people. Here, we reported on a case of elderly man in whom back pain associated with vertebral compression and collapse were presenting features of ALL. The patient has provided written informed consent for the publication of this case report.
Case Presentation
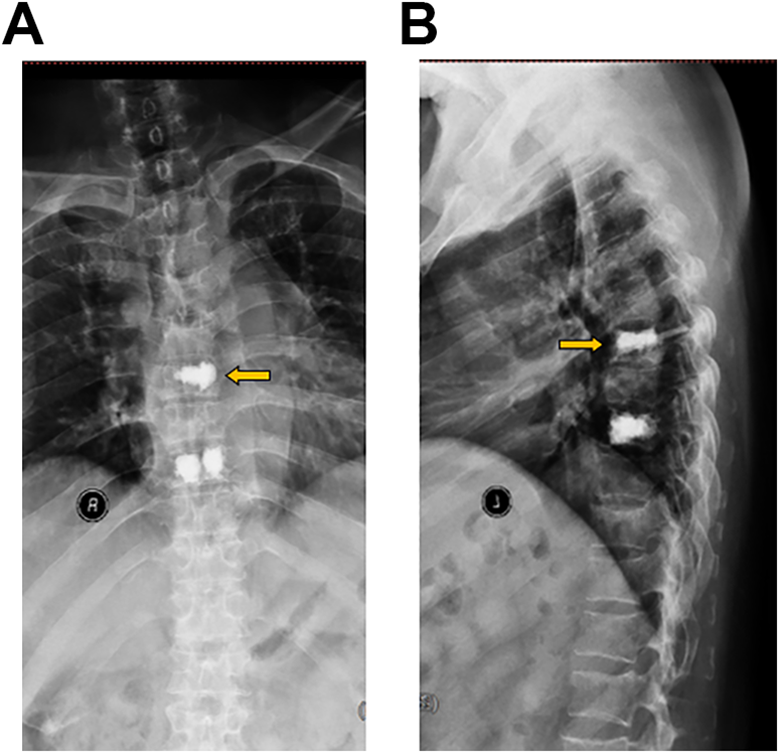
A 65-year-old man was admitted with a 1-month history of progressive chest and back pain and worsening pain after heavy lifting. The pain had no obvious cause. It became painful when standing or walking, and relieved after bed rest. At that time, the thoracolumbar spine X-rays showed obvious spinal degenerative changes which was not match his age. Combined with the clinical symptoms of chest and back pain, the bone density examination was performed to diagnosis furtherly. Bone density examination showed osteoporosis. Then the anti-osteoporosis treatment was given. 3 days later, the patient felt that the symptoms of chest and back pain were significantly aggravated after lifting a heavy object, and the pain was not obviously relieved after resting. So he sought medical attention again. Physical examination revealed widespread pressure and percussion pain in chest and back. X-ray of the thoracic spine showed mild vertebral compression of T5 and T6 (Figure 1A). Further magnetic resonance imaging (MRI) showed a high probability of compression fractures of vertebrae from T5 to T8, T10 and T12 (Figure 1B). Inpatient diagnosis: 1. Multiple spinal compression fractures (T5-T8, T10, and T12); 2. Severe osteoporosis; 3. Hypertension (5-years prior history of hypertension). No abnormalities were found in routine blood examination, liver and kidney function tests after hospitalization. In order to further clarify the responsible segment, bone scans were given to show that increased radioactive uptake in multiple vertebrae of the thoracolumbar spine, especially for T4, T6, T8, T10, T11 and T12 (Figure 1C). Compared with other vertebrae, there was higher accumulation of radioactivity in T6 and T8. At the same time, careful physical examination showed that pressing pain and percussion pain were the most obvious accordingly. Then the T6 and T8 vertebrae were analyzed as fresh fracture and symptom responsibility segment to perform vertebroplasty under local anesthesia and sedation (Figure 2A and B). Intraoperative pathology specimens were sent. And the results demonstrated: the peripheral myeloproliferative hyperplasia was extremely active; adipocytes disappeared; rare erythroid cells and megakaryocytes, myeloblasts and promyelocytes mainly in the proliferative cells, scattered immature eosinophils in the foci. Myeloid sarcoma was considered. The further result of bone marrow biopsy was showed in Figure 3A. Bone marrow hyperplasia was extremely active; 77.5% of the cells were archaeocytes; guanulocytosis was suppressed; 13% of the cells were erythroid cells; 2.5% of the cells were lymphocytes; 299 megakaryocytes were visible in the whole film. Immunophenotype by flow cytometry with CD45 gating: CD45 weakly positive cells accounted for 69.2% of all karyocytes; abnormal cellular antigen expression was dominated by lymphoid differentiation antigen; cCD79 88.9%, CD19 95.9%, CD10 85.6%, CD33 79.5%, CD15 22.3%, CD34 96.8%, HLA-DR 96%, TdT 75.8%. The result of immunohistochemistry (Figure 3B) was negative. Final diagnosis was given as 1) B-ALL with myelocytic antigens; 2) B-ALL with multiple bone metastasis. Finally, the patient was transferred to the hematology department for standardized chemotherapy treatment. After regular chemotherapy, the patient’s symptoms improved significantly. The patient unfortunately passed away in March 2019 from heart failure and lung infection due to atrial fibrillation.

X-ray (A) of the patient’s thoracic spine with obvious degeneration, sagittal MRI (B) showing multi-segment vertebral compression, bone scan (C) showing multi-segment vertebral nucleus concentrations. *All arrow markings in the figures were T-6 vertebrae.
Vertebroplasty of T6 and T8 vertebrae.

Biopsy pathology of vertebroplasty (A), biopsy pathology of bone marrow aspirations (B).
Discussion
ALL is a hematologic neoplasm characterized by the clonal proliferation of lymphoid progenitor cells both in the bone marrow and in extramedullary sites. 10 Symptoms of ALL are generally non-specific and various and include prolonged fever, swollen lymph nodes, petechiae, and dyspnea due to mediastinum enlargement. Diagnosis of ALL was based principally on morphological identification of leukemic bone marrow blasts >25%. 11 Compared with other types of leukemia, ALL is prone to extramedullary infiltration, but generalized osteopenia and vertebral complications are less common. 12 Although ALL accounts for about 15-25% of adult acute leukemias, 13 it is uncommon among older patients (age > = 60 years). 14 According to previous clinical reports, some ALL patients had vertebral fractures, 4,15,16 and most were children or adolescents. Some vertebral fractures also were reported in middle-aged, including a 56-year-old man form China, 7 a man in his thirties form Japan, 8 and 38-year-old man from America. 9 However, to the best of our knowledge, vertebral compression fractures presented as the only symptoms prior to the diagnosis of ALL has not been previously reported in an elderly ALL patient. We reported vertebral compression fractures-as the first manifestations in a 65-year-old ALL patient. Considering the histories of osteoporosis, minor trauma and normal peripheral blood counts, it would be misdiagnosed as spinal osteoporotic compression fractures which were caused by low-energy injuries. Osteoporotic vertebral compression fractures involve thoracolumbar, commonly between T8 and L4. Patients usually have a history of low-energy injury, and it is rare that fractures involve multiple (>3) vertebrae. However, fractures from ALL can involve multiple vertebrae. In normal hematopoiesis, there is a balance between hematopoietic stem cells (HSCs) and components of the hematopoietic microenvironment including osteoblastic cells, osteoclasts, mesenchymal cells, and vascular structures. In leukemia, invasion of leukemia cells would result in osteopenia mediated by an expansion of osteoclasts causing increased bone reabsorption and a concomitant reduction of osteoblastic activity. 17
Vertebral fractures are unusual presentations for elderly leukemia that can cause significant chest and back pain without other systemic symptoms. Normally, the presence of anemia, low or high white cell counts with lymphocytosis, and thrombocytopenia can be a clear signal of bone marrow involvement and the diagnosis would be easy. However, the absence of classic features with unusual features as initial manifestations could lead to delay in diagnosis. This can be considered a diagnostic difficulty when both clinical presentations and abnormal radiographic findings are not traditional characteristics of leukemia patients. Considering that other solid tumors may have pathological compression fractures due to spinal metastases as their primary symptoms and some hematological tumors such as myeloma can also cause spinal damage as initial presentation, bone marrow biopsy in vertebroplasty is recommended. 18
Conclusion
ALL must be considered in the differential diagnosis with acute vertebral compression fracture. Considering that bony lesions may precede clinical findings, knowledge of radiographic and orthopedic appearances of leukemia are important to initiate earlier treatment to avoid the progressive damage and improve their survival rates.
Footnotes
Authors’ Note
The study was approved by the institutional ethics committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by general program of National Natural Science Foundation of China (NSFC) (No. 31671304).