
Abstract
Keywords
Introduction
Osteoporosis is a systemic bone disease associated with increasing age, commonly seen in postmenopausal women and older men, 1 characterized by a reduction in bone mineral content and mechanical strength of the skeleton, and it is the primary cause of fragility fractures in older adults. 2 As the population ages, osteoporotic vertebral compression fracture (OVCF), as the most common complication of osteoporosis, has become a significant cause of low back pain and prolonged bed rest in the elderly. This significantly impacts the quality of life for patients and is becoming a growing public health concern globally.3,4
Currently, percutaneous kyphoplasty (PKP) is the most prevalent minimally invasive technique utilized in managing OVCF. This procedure offers patients substantial alleviation from low back pain and enhanced spinal functionality, permitting them to get out of bed sooner postoperatively and thereby decreasing the occurrence of complications such as decubitus ulcers and pneumonia.5,6 However, there are still patients who experience some debilitating clinical effects after PKP, including residual back pain and recurrent fractures. Previous research has reported that the proportion of residual back pain after PKP ranges between 5% and 20%.7–10 A mate analysis by Dai et al 11 included 1225 patients and found that the chance of re-fracture after PKP was 13.4%. There are also conflicting opinions and no clear consensus on the reasons for the negative outcomes after the PKP.
Sarcopenia, a syndrome of age-related loss of muscle mass, strength, and/or somatic function that occurs primarily in the elderly, has garnered increasing interest from researchers. Some researchers have established the diagnosis of sarcopenia by measuring the third lumbar (L3) skeletal muscle index (SMI) and have investigated the association of sarcopenia with residual pain and recurrent fractures after OVCF.12,13 However, few studies have explored the relationship between prognosis after PKP and sarcopenia in patients with OVCF. We hypothesized that the clinical prognosis of patients with OVCF may be affected by sarcopenia. Thus, the objective of this study was to compare the long-term clinical results of OVCF patients with and without sarcopenia after PKP.
Methods
Patients
This study was authorised by the Institutional Review Board of our hospital, and all patients involved in the research provided informed consent before participating. Patients who suffered from painful osteoporotic vertebral compression fracture (OVCF) and underwent percutaneous kyphoplasty (PKP) between September 2021 and August 2022 were retrospectively reviewed.
Inclusion criteria were as follows: (1) age over 60 years; (2) initial OVCF diagnosis; (3) single-segment fracture from T5 to L4; (4) PKP treatment due to ineffective conservative treatment. The exclusion criteria were as follows: (1) severe neurological symptoms produced by the fracture’s encroachment/compression of the spinal canal; (2) pathological fractures (including tumors and infections); (3) degenerative spinal changes causing low back pain; (4) histories of previous spinal surgery; (5) incomplete patient imaging data.
Surgical Methods
The PKP procedures were performed under local or intravenous anesthesia. The patients were placed in a prone position with the abdomen vacated, and a C-arm X-ray was used to locate the fractured vertebral body. With the assistance of the C-arm guidance, bone puncture trocars were bilaterally introduced through the lateral edge of the pedicles at the level of the fracture. They were then progressively advanced through the pedicles into the vertebral body. After establishing a working channel, careful injection of high-viscosity cement was performed under C-arm fluoroscopy until the cement reached the posterior wall of the vertebral body, where the possibility of leakage was high. After the cement hardened, the working channel was gradually removed. Throughout the procedure, the C-arm fluoroscopy was used for assistance. Following the surgery, the patients were observed for 10-15 minutes. After the operation, all patients were instructed to rest in bed and encouraged to get out of bed with a brace on the first day of PKP.
Evaluation Index
All patients underwent preoperative MRI of the fractured segment, as well as frontal and lateral X-rays. Additionally, bone mineral density (BMD) and appendicular skeletal muscle index (ASMI) were assessed using dual-energy X-ray absorptiometry (DXA). Clinical follow-up period after PKP lasted more than 1 year. At 1, 6, and 12 months postoperatively, patients received regular follow-ups on an outpatient basis or at any instance of recurrent back discomfort. X-rays of the surgical area were reviewed at subsequent follow-up appointments. An MRI was conducted if there was residual back pain or suspicion of a new vertebral fracture.
The clinical and radiological data were documented and evaluated for comparison. Demographic data of the patients included age, sex, body mass index (BMI), bone mineral density (BMD), appendicular skeletal muscle index (ASMI), fracture type (acute fractures or subacute fractures), fractured segment, surgical approach (unilateral or bilateral), bone cement volume, and bone cement distribution (satisfactory or unsatisfactory). Clinical data encompassed the time of initial postoperative ambulation and the total duration of hospital stays. Visual Analog Scale (VAS) scores for back pain and Oswestry Disability Index (ODI) were collected preoperatively, postoperative first day, 1 month, 6 months, and 12 months. Modified MacNab criteria were collected at 12 months. Surgery-related complications, refractures, and residual back pain (VAS score >4) were recorded during follow-up. Radiologic data included changes in regional kyphosis (RK) and vertebral height loss of the fractured vertebrae during preoperative and postoperative follow-up.
Index Definition
The T-score represented BMD. Regarding fracture type, acute fractures were defined as new fractures within 2 weeks, while subacute fractures were defined as fractures occurring within 2 weeks to 2 months. Satisfactory bone cement distribution was defined as bone cement contacting both the superior and inferior endplates, whereas unsatisfactory bone cement distribution was defined as bone cement missing at least 1 endplate.
14
RK refers to the angle created by the tangent line connecting the upper endplate of the upper vertebral body of the damaged vertebra and the lower endplate of the lower vertebral body (Figures 1 and 2). Vertebral height loss rate was defined as the percentage of anterior vertebral body height relative to the average anterior vertebral body height of the upper and lower adjacent levels. An 84-year-old female patient with OVCF and comorbid sarcopenia was treated with PKP. (A) Preoperative sagittal MRI T2 image showed a compression fracture of T12. (B) RK was defined as the angle formed by the tangent line between the upper endplate line a of the superior vertebral body and the lower endplate line b of the inferior vertebral body, and the vertebral height loss rate was defined as (Ha + Hc)/Hb*2*100%. The preoperative RK was 33.6°, and the vertebral height loss rate was 35.1%. (C) Postoperative RK was 27.9°, and the vertebral height loss rate was 62.0%. (D) The 12-month follow-up RK was 29.6°, and the vertebral height loss rate was 54.1%. A 76-year-old male patient with OVCF without sarcopenia underwent PKP. (A) Preoperative sagittal MRI T2 image showed a compression fracture of T8. (B) Postoperative RK was 5.4°, and the vertebral height loss rate was 67.6%. (C) Postoperative RK was 4.8°, and the vertebral height loss rate was84.8%. (D) The 12-month follow-up RK was 5.2°, and the vertebral height loss rate was 82.3%.

DXA separates soft tissue into lean and adipose tissue, which in turn gives the appendicular skeletal muscle index (ASMI), which is limb muscle mass divided by the square of height (Figure 3). Sarcopenia was diagnosed based on the ASMI criteria of <7.0 kg/㎡ for males and 5.4 kg/㎡ for females, according to the definition of sarcopenia recommended by the European Working Group on Sarcopenia in Older People2 (EWGSOP2).
15
Based on the diagnostic criteria, patients were classified into the sarcopenia group and the non-sarcopenia group. A report of whole-body dual-energy X-ray absorptiometry in a 70-year-old patient with sarcopenia. The final ASMI was calculated to be 4.6 kg/㎡.
Statistical Analyses
Quantitative data were expressed as mean ± standard deviation, and all statistical data were analyzed by Statistical Package for the Social Sciences (SPSS) 27.0 software (SPSS, Inc, Chicago, IL, USA).t test was used for measurement data, and intergroup comparison and counting data used chi-square test or Fisher exact probability method. P < .05 was considered to be statistically significant.
Results
General Characteristics of the Patients
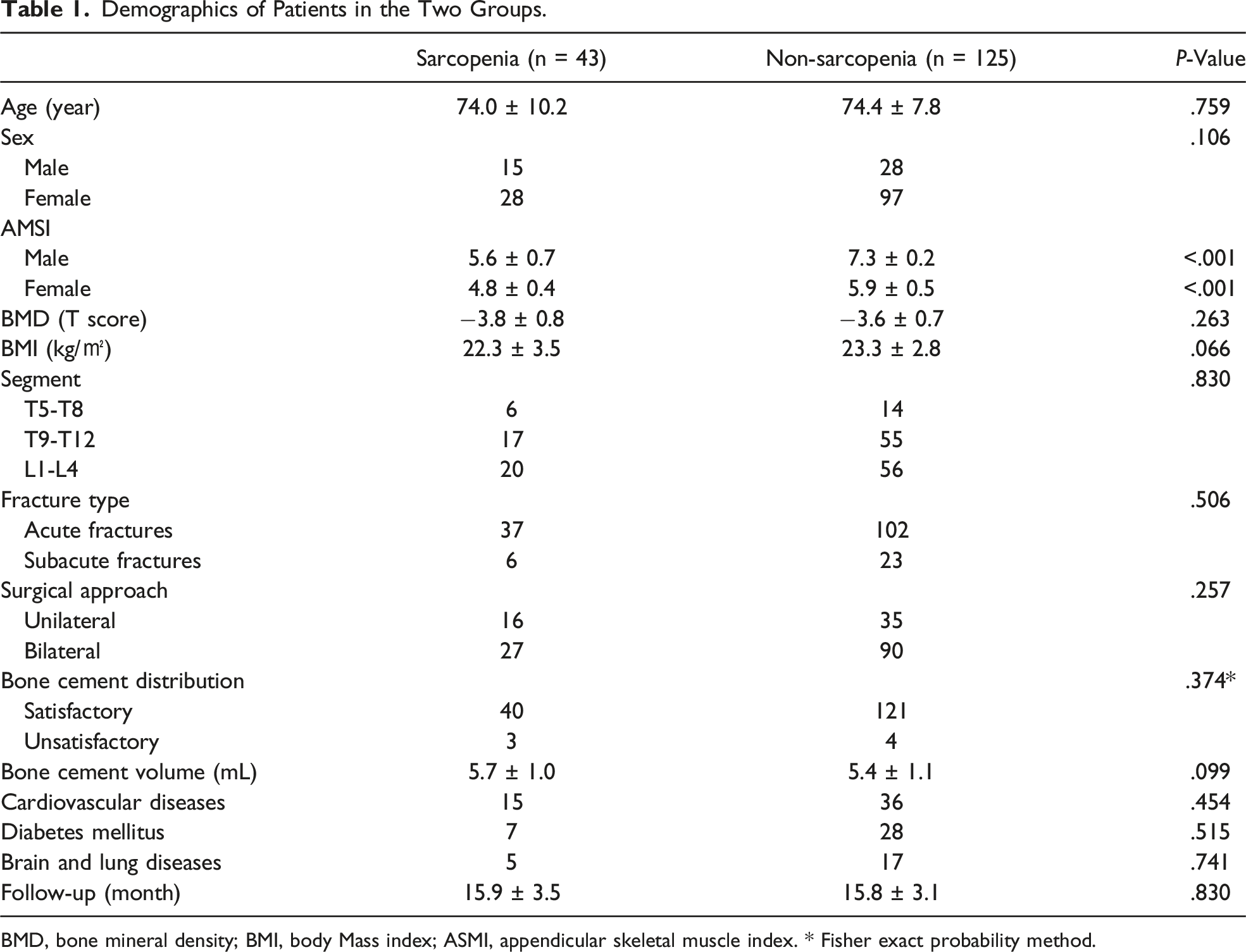
A total of 609 patients were eligible for the study. Following the application of the inclusion and exclusion criteria, 168 patients were ultimately enrolled and 441 individuals were excluded (Figure 4). Based on the ASMI, 43 patients were assigned to the sarcopenia group and 125 patients to the non-sarcopenia group. No significant differences in sex, age, BMD, BMI, fracture type, fractured segment, surgical approach, bone cement volume, bone cement distribution, or comorbidities were found between the sarcopenia and non-sarcopenia groups (P > .05) (Table 1). Flow chart for screening patients. Demographics of Patients in the Two Groups. BMD, bone mineral density; BMI, body Mass index; ASMI, appendicular skeletal muscle index. * Fisher exact probability method.
Clinical Outcomes
Comparison of Clinical Outcomes Between the Two Groups.

VAS, visual analog score; ODI, oswestry disability index.
Radiological Outcomes
Comparison of Radiological Outcomes Between the Two Groups.
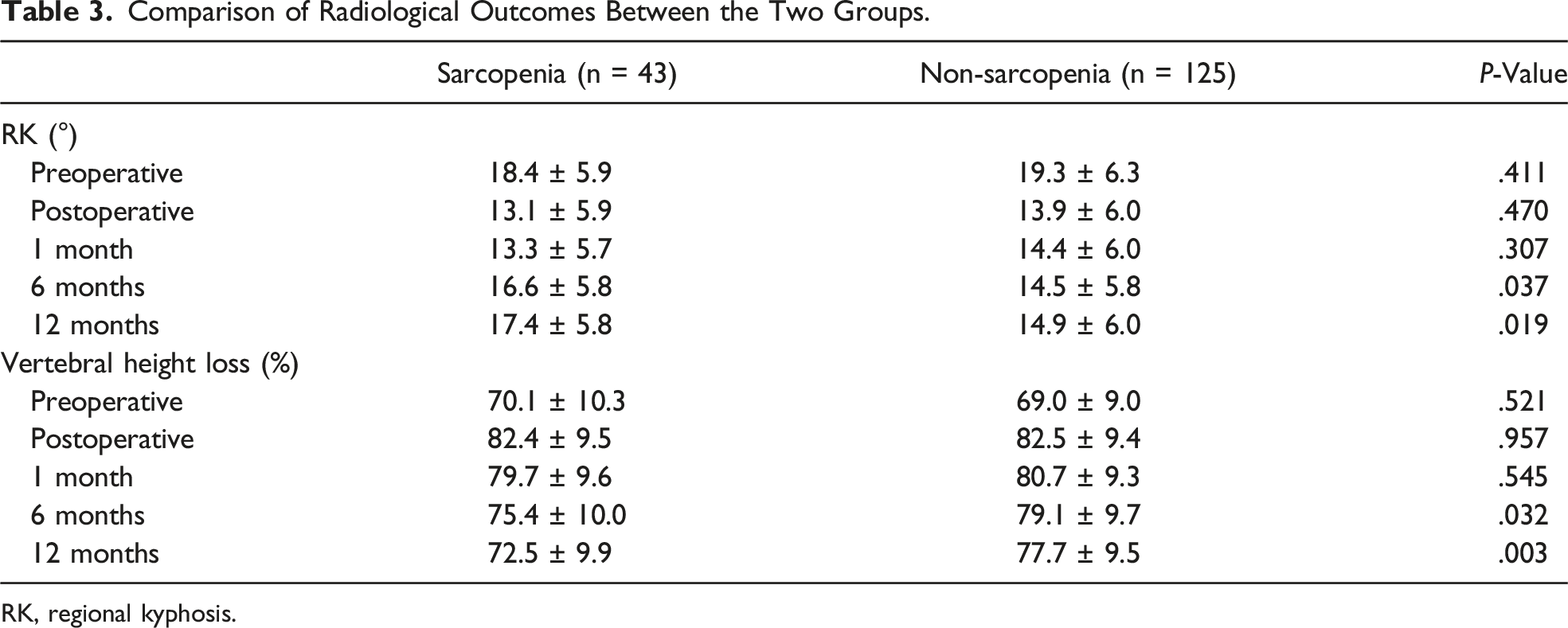
RK, regional kyphosis.
Discussion
Despite the fact that PKP delivers rapid pain alleviation, enhances quality of life, and recuperates vertebral height effectively, a subset of patients still encounter substantial residual back pain and recurrent fractures. Moreover, though sarcopenia is acknowledged to deleteriously affect the quality of life and elevate the risk of falls and disability in elderly individuals, limited research has examined the correlation between sarcopenia and clinical outcomes after PKP in patients with OVCF. Consequently, we scrutinized the impact of sarcopenia on clinical outcomes in patients with OVCF. At 1 year follow-up, especially in the late follow-up period (6 months and 12 months), low back pain (VAS), quality of life (ODI), and imaging findings (regional kyphosis and vertebral height loss rates) were significantly improved in the non-sarcopenia group compared with the sarcopenia group (P < .05). In addition, residual back pain and refractures were less likely in the sarcopenia group (P < .05). The sarcopenia group had a substantially longer time to ambulation (2.1 ± 1.3 d vs 1.7 ± 1.1 d, P < .05) and hospital stay (5.1 ± 2.6 d vs 4.1 ± 3.2, P < .05) than the non-sarcopenia group. At the last visit, the MacNab score was significantly better in the non-sarcopenia group than in the sarcopenia group (P < .05).
Since its initial recognition by Irwin Rosenberg 16 in 1989, sarcopenia has garnered heightened interest amongst scientists worldwide and was progressively acknowledged as a significant public health concern due to its link with falls and fractures, diminished quality of life, mobility impairment, susceptibility to hospitalization, and augmented mortality risk. Sarcopenia was first described as age-related weight loss and, in 2016, was classified as a separate disorder. In 2010, EWGSOP 17 proposed a three-component diagnosis of sarcopenia: reduced muscle mass, strength, and physical function. For the diagnosis of “sarcopenia”, EWGSOP recommended the simultaneous diagnosis of low muscle mass + low muscle function (strength or performance). Following this trend, several international working groups have released revised consensus definitions of sarcopenia in recent years.18,19 However, in 2018, the European Working Group on Sarcopenia in Older People 2 proposed an improved perspective. They considered reduced muscle strength as a primary characteristic of sarcopenia, advocating for its diagnosis through the assessment of both low muscle quantity and quality, and the identification of poor physical performance as indicative of severe sarcopenia indicators. 15 Previously, CT-based measurements of the psoas major muscle were also used to detect low muscle mass to simplify and predict morbidity in certain conditions (cirrhosis, bowel surgery). 20 However, because the psoas is a small muscle, some experts argue it is not representative of overall sarcopenia. 21 In contrast, DXA, a technique that has emerged in recent years, directly and accurately measures muscle mass and fat mass in different body parts, thereby improving diagnostic accuracy. In practice, DXA has been most commonly recommended for diagnosing sarcopenia by measuring ASMI. In our study, due to the constraints of retrospective research, muscle strength measurements (grip strength and chair stand test) were not available for all patients. Therefore, sarcopenia was diagnosed solely based on the muscle mass threshold required by EWGSOP2, with muscle mass primarily assessed through ASMI measured by DXA.
Sarcopenia is strongly correlated to OVCF. Isaacson et al 22 pointed out in a study that the interaction mechanism between bone and muscle is mainly reflected in 2 aspects: (1) both bone and skeletal muscle have the function of secreting cytokines, and a variety of endocrine factors work together to coordinate the synthesis and catabolism of the bone-muscle system; (2) muscle contraction can promote osteogenesis, and the increase in bone mass can enhance the biomechanical effect of muscle on bone. Vertebral fractures are clinically more likely to occur in patients with sarcopenia, especially trunk muscle loss combined with osteoporosis. In a study conducted by Didier et al, 23 it was found that men with both low bone mineral density (BMD) and sarcopenia had a significantly higher risk of fracture compared to men with normal BMD and no sarcopenia. The hazard ratio (HR) for this group was 3.79, with a 95% confidence interval (CI) of 2.65-5.41. Men with low BMD only also had an increased risk of fracture, with an HR of 1.67 (95% CI = 1.45-1.93). However, men with sarcopenia only did not show a significant increase in fracture risk, with an HR of 1.14 (95% CI = .62-2.09). Moreover, the dual role of osteoporosis and sarcopenia has a substantial adverse effect on the survival prognosis of the elderly. Mortality in men with both osteoporosis and sarcopenia was shown to be significantly higher than in patients with either osteoporosis or sarcopenia alone, with a 1.8-fold increase in the former compared to the latter. 24
Several studies have illustrated that sarcopenia is not only highly correlated with the development of OVCF, but is also one of the strongest risk factors for residual pain and refractures after PKP. Bo et al 12 reviewed the clinical data of 56 OVCF patients with residual back pain and 100 OVCF patients without residual back pain and revealed that sarcopenia may be a potential factor contributing to the incidence of residual back pain after surgery. Wang et al 13 followed 237 OVCF patients after PKP and found that 64 (27.0%) patients had a refracture. Sarcopenia was found in 48 patients (20.3%), including 21 refracture patients and 27 non-refracture patients. In our study, the occurrence of residual back pain (9/43,20.9% vs 11/125,8.8%; P < .05) and refractures (12/43,27.9% vs 15/125,12.0%; P < .05) were higher in the sarcopenia group than in the non-sarcopenia group (P < .05), which corroborated existing studies.
In our study, VAS scores, ODI scores, regional kyphosis, and rate of vertebral height loss were significantly improved in the non-sarcopenia group compared with the sarcopenia group at 6 and 12 months (P < .05). We believe that this clinical outcome may be due to a compensatory mechanism of the sagittal balance of the spine. Muscles operate as tension bands during the spinal compensation process, according to the bowstring theory. 25 The greater the muscle quality, the better the spine’s compensating ability. In patients with sarcopenia, the paraspinal muscle mass is reduced and is not strong enough to compensate for the sagittal imbalance of the spine caused by compression fractures. As the disease progresses, the paravertebral muscles become overstretched, taking on too much tension over time. The result is increased back pain and reduced quality of life for the patient. In a study by Hiroyuki et al, 26 85 spinal surgery patients were classified into the sarcopenia group and the non-sarcopenia group based on appendicular skeletal muscle mass (ASM). The study found that the postoperative JOA scores were substantially lower in the sarcopenia group compared to the non-sarcopenia group (P < .05), and a higher proportion of patients in the sarcopenia group required postoperative rehabilitation (P < .05). Our clinical outcomes are partially consistent with their study.
In OVCF patients with sarcopenia, sarcopenia must be intervened and treated concurrently with fractures treatment. Rehabilitation training and early nutritional support can be given to patients during the perioperative period, such as supplementing essential amino acids, appropriate amounts of protein, and fatty acids. Patients undergoing surgical rehabilitation should be instructed to wear their braces properly and to refrain from experiencing more falls during exercise.
We note some limitations of this study. Firstly, due to the retrospective nature of the research, sarcopenia was diagnosed solely based on DXA-measured ASMI, lacking evidence of decreased muscle strength. Secondly, to avoid the influence of various factors, this study used strict inclusion criteria to select patients, which resulted in a relatively small sample size. Lastly, we chose 12 months as the postoperative study period, which was too short a follow-up period, whereas the effects of sarcopenia on OVCF patients are much longer term. Therefore, multi-center, large-sample, long-term follow-up studies are needed to further investigate how clinical outcomes after PKP in OVCF patients are affected by sarcopenia.
Conclusion
According to our data, clinical outcomes after PKP in patients with OVCF could be negatively affected by sarcopenia. These include prolonged postoperative bed rest and hospital stay, poor long-term pain relief, reduced quality of life and spinal function, or even residual pain and re-fractures. Therefore, in OVCF patients with sarcopenia, it may be beneficial to intervene and treat sarcopenia in conjunction with fracture treatment.
Footnotes
Acknowledgements
We acknowledge to the multidisciplinary team in the Second Affiliated Hospital of Chongqing Medical University, including colleagues in orthopedics, radiology and anesthesiology, for their participation in the treatment planning and implementation and the preparation of this article.
Author Contributions
This study was designed and organized by Yang Wang and Shan Wu. Data cleaning, analysis and writing of the first draft was by Shan Wu, supported by Guosheng Zhao, Dian Zhong, Yang Liu, Yang Wang. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
Shan Wu, Dian Zhong, Guosheng Zhao, Yang Liu, Zhenyong Ke, and Yang Wang declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Program for Youth Innovation in Future Medicine, Chongqing Medical University(W0021).