
Abstract
Introduction
Fragility vertebral compression fractures (VCFs) are of major concern due to aging populations worldwide, which may occur after a fall from standing or due to severe osteoporosis, impacting greatly the life quality of the elderly. This study thus determined the factors independently associated with poor functional recovery from a new VCF and changes in sagittal spinal alignment after vertebroplasty in elderly patients with osteoporosis.
Materials and Methods
The data were collected from patients older than 70 years and diagnosed with a new VCF. Logistic regression analysis was performed to determine factors independently associated with function and radiographic status.
Results
We enrolled 8 male and 34 female patients with a mean age of 80.74 ± 8.31 years between January and July 2020. Compared with preoperative data, post-vertebroplasty lumbar sagittal alignments and functional scores improved significantly, and function recovered gradually over 12 weeks. Climbing stairs was the most influential performance indicator at the beginning of the recovery process. At each postoperative follow-up, changes in the C7-sacrum sagittal vertical axis exhibited an influence on functional recovery. Male patients were better able to move from a chair to a bed at the 2-week postoperative follow-up, and positive changes in the spino-sacral angle led to improved function in terms of stair climbing at the 6-week postoperative follow-up.
Conclusions
Vertebroplasty seemed to be effective for functional recovery related to sagittal spinal alignment improvement of the elderly with VCFs during postoperative 12 weeks, which may be a critical stage for the recovery for their life activities. The recovery rate for stair climbing after vertebroplasty was slower than for the other functional performance indicators in our study. In addition, if a patient was unable to demonstrate a marked improvement in sagittal alignment, they were likely to have ongoing impaired function and a poor prognosis after surgery.
Keywords
Introduction
Osteoporosis is one of the most common disorders among elderly adults, especially elderly women. A decrease in bone mineral density (BMD) and reduced bone quality result in structural and microarchitectural destruction of the vertebral body. According to the Nutrition and Health Survey in Taiwan (2004-2008), the prevalence of osteoporosis increases to 22.57% in men and 41.17% in women after the age of 50 years. Of the comorbidities of osteoporosis, osteoporotic vertebral compression fracture (OVCF) is a major health issue because it may have a severe impact on the quality of life and the survival of patients.1,2 The prevalence of OVCF in Europe is 12.1/1000 person-years for women and 6.8/1000 person-years for men after the age of 50. 3 Ballane et al reported higher rates of OVCF in Taiwanese women compared with those in other Asian countries, 4 and Burge et al revealed that OVCF would cost the insurance companies, the state, or the health-care providers at least US$1 billion in the United States by 2025, 5 resulting in a tremendous burden on the health care system and social security due to the increased need for long-term care facilities, hospitalization, and vertebral augmentation procedures.
Symptoms of OVCF include severe back pain, radiculopathy, and severe neurologic deficit, which may induce psychological impairment and poor social function. 6 Adequately controlling pain, correcting deformities, delaying deterioration, and treating underlying osteoporosis are key means of treating symptoms. Conservative treatments, including analgesics, bracing, and bed rest, have achieved only relatively poor outcomes in patients with OVCF, 7 and ongoing mobility and pain control problems after trauma are of great concern. 8 Conventional minimally invasive treatments, such as percutaneous vertebroplasty (VP) and kyphoplasty (KP), have become the main procedures for treating OVCF in recent years.9,10 Both of these procedures result in effective pain relief, functional recovery, increased mobility, and a decreased need for painkillers.11,12
Sagittal balance of the spine ensures minimal muscle effort is required to maintain a stable standing position and is essential for maintaining normal spinal biomechanics. 13 The thoracolumbar region is the most common fracture site because of its specific biomechanical characteristics. 14 KP can correct sagittal alignment, including the T1 pelvic angle (TPA) and spino-sacral angle (SSA) because of the ballon placement, 15 but the change of the sagittal alignment after VP and its correlation with the functional recovery was few mentioned in the literature.
In this study, we investigated the change of sagittal alignment by using percutaneous VP, evaluating the outcomes with the Barthel index (BI). The Oswestry Disability Index is one of the most commonly used tools for quantifying disability related to lower back pain. 16 However, this questionnaire focuses on spondylosis and radiculopathy. By contrast, the BI is used to measure performance in the activities of daily living, and it is the most common tool used by the Taiwanese government and social welfare and medical institutions to evaluate an elderly patient’s function.
Method
This study was performed under the approval of the Research Ethics Committee of our hospital. We recruited the patients diagnosed with OVCF at our hospital between January and July 2020, excluding patients who had undergone previous spinal instrumentation surgery; had a history of cancer, multiple fractures, or cardiopulmonary disorders; or exhibited evidence of spinal infection, pathologic fracture, or difficulty standing straight.
After admitting these patients to the ward, one physician and one nurse practitioner assisted the patients and their family in completing a questionnaire based on the BI and visual analog scale (VAS). In addition to the preoperative BI, we also collected baseline BI scores from before the patient experienced an OVCF. The BI includes three performance indicators, namely transferring from chair to bed (transfer), walking capability (mobility), and stair climbing (stairs), and data on these indicators were extracted from the completed questionnaires to evaluate ambulatory function.
Basic data, including body mass index and underlying diseases, were collected by the nurse. BMD measurements, magnetic resonance imagining (MRI), and plain film and whole spine radiography were performed in the outpatient or emergency department.
Percutaneous VP was performed by two orthopedic attending physicians and two senior residents; procedures were performed under either local or general anesthesia. After adequate pain control and brace assistance, most of the patients were discharged within 24 hours. Subsequent outpatient appointments were scheduled at postoperative weeks 2, 6, and 12. During the outpatient appointments, BI and VAS data were collected by one physician with a nurse practitioner and the patients’ family. Whole spine radiography was arranged at postoperative weeks 2, 6, and 12.
Radiographic Analysis
Whole spine radiography was conducted preoperatively, postoperatively, and then at the 2-, 6-, and 12-week follow-up appointments. We quantitated that the fractured vertebral body changes before and after VP by measuring the angle of the upper end plate and the lower end plate of the fractured column from the lateral view of the plain film. The other radiological parameters of the spine, including the sagittal vertical axis (SVA), SSA, TPA, pelvic incidence, pelvic tilt (PT), sacral slope (SS), lumbar lordosis, thoracic kyphosis (TK), and thoracolumbar kyphosis were recorded by three orthopedic residents. The spino-pelvic sagittal parameters were also described. We divided the patients into three groups: the thoracic group (T1–T9), thoracolumbar group (T10–L2), and lumbar group (L3–L5), according to the location of the fractured vertebra.
Statistical Analysis
An independent t test was used to compare the demographic characteristics between males and females. A stepwise multivariable linear regression analysis estimated the associations between function scores and sagittal spinal parameters. All reported P values <.05 were considered statistically significant. The statistical software SPSS for Windows, version 21.0 (IBM Corp, Armonk, NY, USA), was used for the analyses.
Results
Demographics (n = 42).

Data are presented as n or mean ± standard deviation.
*P value <.05 was considered statistically significant after test.
Change of sagittal alignment parameters (n = 42).

Data are presented as n or mean ± standard deviation.
*P value <.05 was considered statistically significant after test.
Abbreviation: LL, lumbar lordosis; SSA, spino-sacral angle; SVA, sagittal vertical axis; TK, thoracic kyphosis; TPA, T1 pelvic angle.
Recovery rate of individual part of Barthel index at each follow-up timepoint (2 W/6 W/12W) (n = 42).
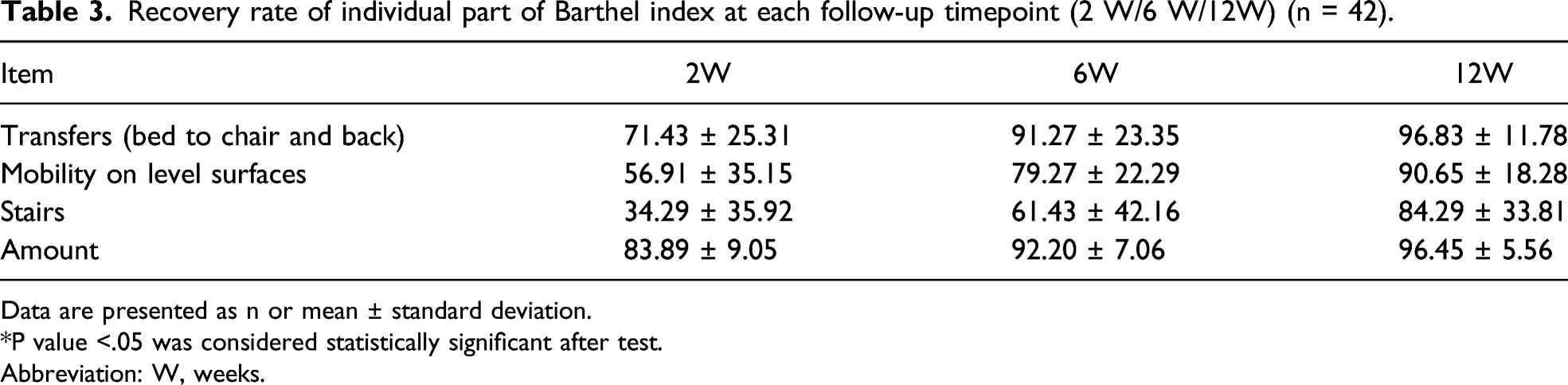
Data are presented as n or mean ± standard deviation.
*P value <.05 was considered statistically significant after test.
Abbreviation: W, weeks.
Change of low back pain VAS at each follow-up timepoint (n = 42).

Data are presented as n or mean ± standard deviation.
*P value <.05 was considered statistically significant after test.
Abbreviation: W, weeks.
Factors associated with change of Barthel Index at post-fracture 2 weeks (n = 42).
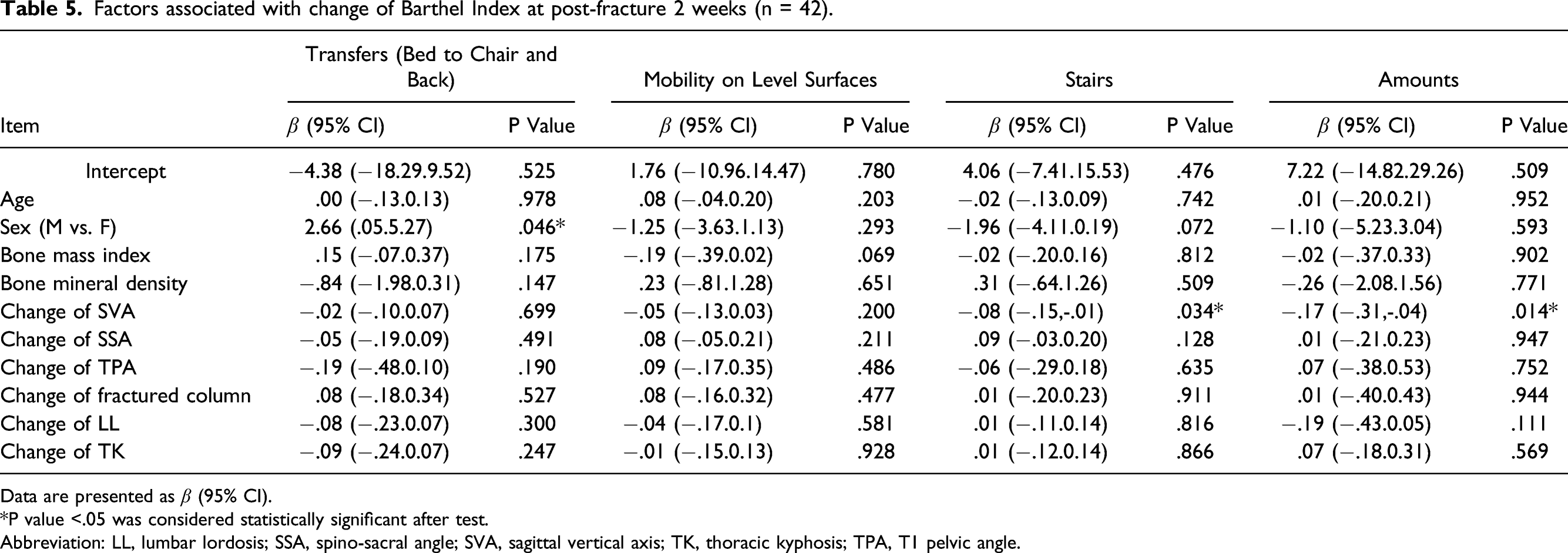
Data are presented as β (95% CI).
*P value <.05 was considered statistically significant after test.
Abbreviation: LL, lumbar lordosis; SSA, spino-sacral angle; SVA, sagittal vertical axis; TK, thoracic kyphosis; TPA, T1 pelvic angle.
Factors associated with change of Barthel Index at post-fracture 6 weeks (n = 42).

Data are presented as β (95% CI).
*P value <.05 was considered statistically significant after test.
Abbreviation: LL, lumbar lordosis; SSA, spino-sacral angle; SVA, sagittal vertical axis; TK, thoracic kyphosis; TPA, T1 pelvic angle.
Factors associated with change of Barthel Index at post-fracture 12 weeks (n = 42).

Data are presented as β (95% CI).
*P value <.05 was considered statistically significant after test.
Abbreviation: LL, lumbar lordosis; SSA, spino-sacral angle; SVA, sagittal vertical axis; TK, thoracic kyphosis; TPA, T1 pelvic angle.
Discussion
When conservative treatment fails, percutaneous VP is considered the most effective treatment for symptomatic OVCF. Studies have demonstrated excellent pain relief, functional recovery, and increased mobility following this treatment.11,12 Percutaneous VP is more effective for short-term pain relief, and KP has demonstrated increased effectiveness for medium-term functional improvement. 10 However, no significant difference has been demonstrated between VP and KP in terms of long-term functional recovery and pain relief.10,17 Although KP appears to result in improved radiologic outcomes, this procedure has not been associated statistically with any clinical outcomes. VP improves the kyphosis angle in cadavers, depending on the amount of cement, and Ates et al preferred VP to KP because it was an easier and cheaper method to perform. 12 In our study we found that VP could effectively improve the function of the elderly patients with VCFs and the sagittal spinal alignment of them also improved at the same initial 12-week stage. The change of the sagittal spinal alignment may be cause of the improvement of back pain symptom after VP, which seemed to be an addictively positive effect for the daily function restoration of the elderly.
Sagittal balance plays a key role in maintaining the spine’s straight posture, thus preventing progressive spinal deformity; this is achieved by contributing to the minimal effort required of the core muscles, minimal tension in the ligamentous structure, and minimal energy consumption. 18 The pelvis and spine must be in a harmonious relationship with the lower extremities and trunk to maintain an ergonomic and stable posture. If the torso’s centroid cannot remain at a certain distance from the pelvis, the cone of economy, which refers to the stable region in a standing posture, cannot be maintained, causing an increasing expenditure of energy. 19
The SVA, SSA, and TPA were measured to assess global alignment. A patient’s position and pelvic rotation and deviation in the X-ray projection distance can influence the final SVA result 20 ; thus, we measured the SSA and TPA as angular parameters not requiring proportional calibration. The SSA can reflect global alignment and kyphosis, 21 and the TPA not only indicates global and local spino-pelvic sagittal alignment but also the compensatory mechanism of the spine and pelvis. 22
Local deformity of the spine, such as OVCF or degenerative spondylosis, may result in an abnormal sagittal alignment and gravity line. To adapt to this phenomenon, pelvic posterior rotation, including decreased SS, increased PT, and decreased TK, was performed to maintain the torso in an upright position. Failure of the compensatory mechanism may lead to both hip and knee flexion, which represents positive sagittal alignment at this stage. 23 In the later stages of OVCF, after the failure of the compensatory mechanism and core muscle fatigue, horizontal gaze fails.
A combination of core muscle fatigue, failure of the cone of economy, decreasing global alignment, and horizontal gaze failure may result in a traumatic fall. Falling is a worldwide problem for the elderly population, causing unexpected hospitalizations or visits to the emergency department. 24 Elderly patients who have fallen face a decline in physical function, a deterioration in mental status, and a risk of death 25 ; falls also have a negative impact on financial and social support systems. Furthermore, if a patient is hospitalized, they can be exposed to nosocomial infection with highly virulent microorganisms, resulting in diseases such as pneumonia or urinary tract infection. Hospital-acquired infections lead to increased morbidity, complications, and mortality in older patients compared with younger patients. 26 Furthermore, older patients with lower BI scores at the time of hospital admission have a relatively high mortality rate, especially female patients. 27
In terms of the results of this study, the SVA, TPA, TK, and VAS scores were improved at the 2-week follow-up. Improved global alignment and pain result in easier rehabilitation for elderly patients. At the 2-week follow-up, the male patients had an improved transfer function compared with the female patients, which may be related to their higher muscle mass. The BI score and mobility and stair functions were not significantly related.
In addition, the more the SVA improved, the more the BI score and stair function improved. This phenomenon was also observed at the 6- and 12-week follow-ups. Improvements in global alignment can help patients achieve a straighter posture and improved horizontal gaze, preventing further falls when climbing stairs.
The limitation to our study is relatively small sample size and short-term follow up even though spinal alignment may be changed by time. In addition, we couldn`t enforce the patient to keep a relative up-straight posture in the acute stage of compression fracture, but the cobb angle and body height of the fractured vertebral body were corrected. It may be related to the postural reduction with spine table which can make the thoracolumbar spine more lordotic, and this way may mimic the vertebral shape improvement and kyphosis correction of kyphoplasty. Despite the above limitation, the result of our study still pointed out that vertebroplasty for the elderly with acute VCFs in the subacute phase was effective for their functional restoration and spine alignment improvement and this stage was very critical for the recovery of life quality of them.
In conclusion, vertebroplasty was effective for the elderly patients with acute VCFs in the improvement of function and sagittal spinal alignment in 12 weeks, which was a critical stage for their future recovery. Falling is traumatic for the elderly population, especially when it occurs on stairs. The recovery rate for stair climbing after VP was slower than for the other functional performance indicators in our study. In addition, the poorer functional recovery seemed to be related to the less change of sagittal spinal alignment. In these circumstances, the family can be provided with guidance on postoperative care. Patients must be careful when climbing stairs, and their family or caregiver must ensure that the patient’s accommodation is obstacle free and pay attention to the patient when they are on th e move.
Footnotes
Acknowledgment
This manuscript was edited by Wallace Academic Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study received ethics approval from the Research Ethics Committee of Hualien Tzu Chi Hospital (IRB- 107-255B)