
Abstract
Introduction:
Patient outcomes following modern dual-mobility cup total hip arthroplasty (DM-THA) remains a concern. Few reports have focused on the use of modern DM-THA in the setting of Asian populations for displaced osteoporotic femoral neck fractures (FNFs). This study aimed to investigate the outcomes of Chinese population with displaced osteoporotic FNFs initially treated with modern DM-THA.
Materials and Methods:
Data from 112 consecutive patients (112 hips) with displaced osteoporotic FNFs initially treated with modern DM-THA during 2011-2018 were retrospectively analyzed. Follow-ups were performed at 3 months, 6 months, 12 months, and then every 1 year after surgery. The primary endpoint was the Harris Hip Score (HHS); the secondary endpoint was the main orthopedic complication rate.
Results:
The mean HHS improved from 58.62 (±15.79) prior to surgery to 86.13 (±9.92) at the final follow-up. The main complication rate was 14.2% (16/112). Sixteen complications in 10 patients were recorded. Of the 16 complications, there were 2 (1.7%) cases requiring revision DM-THA, 3 (2.6%) cases of loosening, 2 (1.7%) cases of migration, 3 (2.6%) intra-prosthetic dislocation (IPD), 4 (3.5%) cases of tilting, and 2 (1.7%) cases of severe wear. The need for revision was attributed to prosthesis loosening associated with poor bony quality.
Conclusion:
In patients with displaced osteoporotic FNFs, DM-THA may yield favorable functional outcomes and a low rate of main orthopedic complications, in particular, a low dislocation rate.
Introduction
Dislocation or instability following total hip arthroplasty (THA) is well-known, is attributable to diverse reasons, and frequently requires revision. 1 -6 Among mostly active patients, dislocation that occurs secondary to THA has increasingly become a concern. 2,7,8 The use of small cups can lead to prosthesis loosening or instability instigated by large forces, 9 which are associated with poor outcomes of THA and the markedly high incidence of revision THA, as well as the short time between failures. 10 -12 Although THA has become less preferred, surgeons have attempted to overcome this issue of dislocation using diverse strategies to decrease the risk of post-surgical dislocation, including using large cups, modular components that can be exchanged, or components made of cross-linked polyethylene. 3,13 -15
The dual-mobility THA(DM-THA) has exceptional dislocation-free survivorship in primary or revision THA, ranging from 95% at 5 years to 80% at 15 years after primary THA and more than 95% at 10 years after revision THA; therefore, it has been used increasingly more frequently in clinical practice in recent decades. 11,16 DM-THA is another procedure that is performed to reduce the rate of post-surgical dislocation. 10 Through the unique DM design, with the femoral head captured within polyethylene, DM cups can maximize the impingement-free arc of motion, have a superior head-to-neck ratio, and increase the safety area required for dislocation. 2,13 Theoretically, it is a safe, effective and durable solution for preventing dislocation. 17,18 Several studies 10,17,18 have demonstrated that DM-THA significantly reduces the rate of dislocation in the management of FNFs. Conversely, serious complications have occurred following the utilization of non-modular DM cups, primarily early dislocation triggered by the premature wear of the polyethylene component. 19
Displaced FNFs are frequently treated using either THA or hemiarthroplasty; nevertheless, treatment selection tends to be controversial. 20 Given that the most common indication for conversion of failed hemiarthroplasty to a THA is pain that is usually attributed to acetabular erosion, especially in patients with osteoporosis, 21 we prefer THA over hemiarthroplasty in the management of displaced FNFs among these patients. Recent data 21,22 have shown that THA may be a better alternative compared with hemiarthroplasty in reducing pain and improving quality of life.
Modern DM cups is frequently used in our level III medical center due to its low dislocation rate. The theoretical effects of modern DM cups matched with crossed-linked polyethylene have not been properly confirmed in the literature. 23,24 Currently, no definitive consensus exists on the outcomes following displaced osteoporotic FNFs initially treated with modern DM cups in Chinese population. Hence, we performed a retrospective study to investigate the outcomes of Chinese population with displaced osteoporotic FNFs initially treated with modern DM-THA.
Methods
Study Population
This study was approved by the Investigational Ethics Review Board (The Affiliated Hospital of Jiangnan University, Jiangsu, China), and an exemption from informed consent was obtained from the board. A total of 176 consecutive patients (176 hips) who initially underwent a modular DM-THA (an uncemented cup, Smith and Nephew Synergy; a uncemented stem, Memphis, TN) due to displaced osteoporotic FNFs from August 2011 to May 2018 were identified in the Joint Surgery Data Sharing Center database at our level III medical center. The DM articulations consisted of a socket, a free polyethylene liner, and a metal head. The acetabular shell consists of titanium alloy with a porous coat of titanium on the outer surface, and a bearing surface with screw holes for additional fixation, if necessary. The modular femoral head is stainless steel with a diameter of 22.2-28.0 mm. The DM cup size is optional with a diameter of 48-60 mm. The main inclusion criteria for this study were patients with FNFs (OTA/AO: 31-B2 and 31-B3); all surgical procedures having been conducted using a direct anterior approach (DAA), as previously described 16 ; a bone mineral density T-score of ≤ 2.5 at the femoral neck; a freshly closed FNF. The main exclusion criteria were as follows: non-modular DM cups; concomitant contralateral FNFs; pathological FNFs; lacking study data (i.e., imaging data and follow-up data); severe systemic infection (i.e., acquired immune deficiency syndrome); dyskinesia prior to fracture; bone-related diseases (i.e., osteoarthritis, rheumatoid arthritis, osteomalacia, osteonecrosis, bone metabolism disorder, or hip deformities); a previous hip surgery; the inability to undergo a follow-up; an injury severity score (ISS) of ≥8; dysfunction of a vital organ (i.e., brain, heart, lungs, kidneys, or liver); the consumption of drugs that affect bone metabolism; and an American Society of Anesthesiologists (ASA) physical status of IV or V.
Of 176 patients, 64 were excluded because they met 1 or more exclusion criteria, resulting in 112 patients with a displaced osteoporotic FNF (OTA/AO: 31-B2 or B3) who initially underwent modern DM-THA were included for the final evaluation, as shown in Figure 1. There were 48 men and 64 women, with a mean age of 64 years (53-74 years). Table 1 summarized the baseline data of patients who underwent modern DM-THA. Mean body mass index (BMI) was 27.1 kg/m2 (20.4-24.2 kg/m2). The median follow-up was 60.8 months (25-75 months).

Flow diagram demonstrating methods for identification and exclusion of study to investigate the outcomes following displaced osteoporotic femoral neck fractures (FNFs) treated with modern dual-mobility cup total hip arthroplasty (DM-THA) as an initial process in Chinese population.
Patient Demographics and Outcomes.
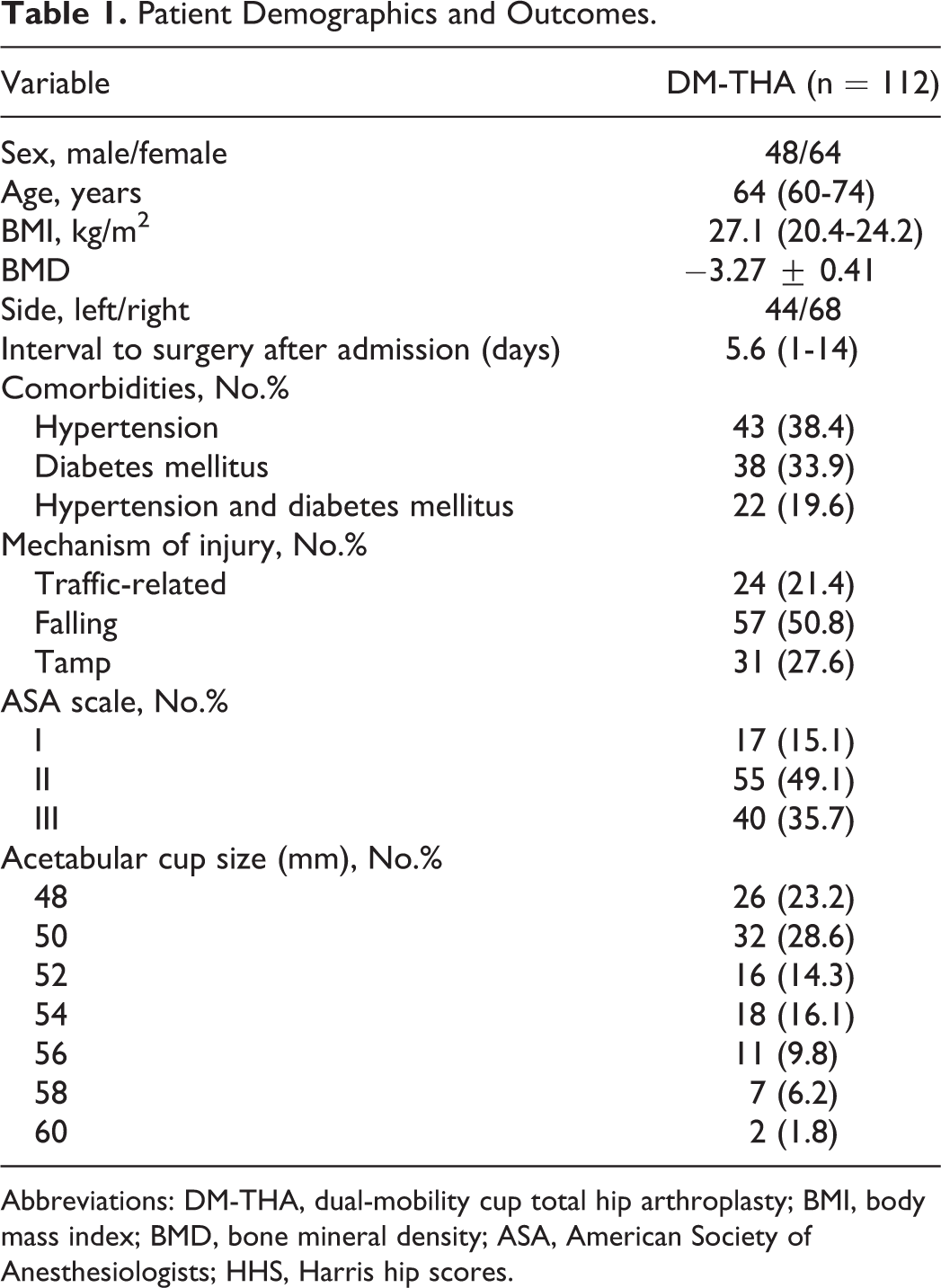
Abbreviations: DM-THA, dual-mobility cup total hip arthroplasty; BMI, body mass index; BMD, bone mineral density; ASA, American Society of Anesthesiologists; HHS, Harris hip scores.
Post-Surgical Management
The image of the implanted prosthesis is shown in Figure 2A-D and Figure 2E. Figure 2F shows a satisfactory prosthesis position. Patients without contraindications underwent low-molecular-weight heparin to prevent thrombus and wore stockings. Passive and active exercises of the affected hip were performed the day after surgery. Partial weight-bearing was permitted with the aid of functional crutches within 1 month after surgery. Full weight-bearing exercises were encouraged from 1.5 months after surgery. An experienced rehabilitation therapist prescribed specific functional exercises and detailed training for patients.

Intra-operative clinical photographs of a femoral neck fractures (FNFs) being performed using dual-mobility cup total hip arthroplasty (DM-THA): (A) the location of the acetabular cup; (B) the position of the stem in the intertrochanter; (C and D) the position of the distal end of the stem in the medullary cavity; (E) Intraoperative fluoroscopic image of the stem and cup after implantation; (F) immediate post-surgical radiograph of DM-THA for FNFs showing satisfactory prosthesis position.
Outcome Evaluation
A standard protocol was conducted to gather clinical and radiographic data. Post-prosthesis follow-ups were performed at 3 months, 6 months, 12 months, and then every 1 year after surgery. The primary endpoint was the HHS, which was assessed at each follow-up by the 2 co-authors (WY and MC) who were not involved in the surgery; the secondary endpoint was the main orthopedic complication rate. Serial radiographs were analyzed by experienced radiologists. The occurrence of main orthopedic complications was documented during the follow-ups. Loosening of the DM cup was defined as cup migration or angular rotation exceeding 3 mm3. Intra-prosthetic dislocation (IPD) was defined as more than 4-mm eccentric displacement of the femoral head from the polyethylene liner. 25 The classification of IPD is based on the previous description. 26 Revision was defined as the removal or exchange of any component. 24
Statistical Analysis
The descriptive statistics include continuous variables (i.e., age, BMI, and HHS) expressed as means, standard deviations (SD) and ranges, as well as categorical variables (i.e., sex, complications) expressed as percentages. Categorical data were compared using Chi-Square tests; continuous data were compared using Student t-test for normally distributed variables and Mann- Whitney U test for non- normally distributed variables. All analyzes were performed using SPSS, version 26.0 (IBM, Armonk, NY). A 2-sided p value of 0.05 was used as the significance level for all comparisons.
Results
Primary Endpoint
Table 2 exhibited the median HHS after surgery. The mean HHS improved from 58.62 ( ± 15.79) prior to surgery to 86.13 ( ± 9.92) at final follow-up. Approximately 78% of patients with a displaced osteoporotic FNFs (OTA/AO: 31-B2 or B3) had a favorable functional score (≥85) at final follow-up.
Long-Term Follow-Up: Functional Outcomes.

Abbreviation: DM-THA, dual-mobility cup total hip arthroplasty.
Secondary Endpoint
Table 3 exhibited the main orthopedic complications. The main complication rate was 14.2% (16/112). Sixteen complications in 10 cases were recorded including revision, loosening, migration, dislocation, tilting, and wear. Of 16 complications, there were 2 (1.7%) revision, 3 (2.6%) loosening, 2 (1.7%) migration, 3 (2.6%) IPD (Type 1), 4 (3.5%) tilting, 2 (1.7%) wear. Two patients requested a revision surgery due to a failed DM-THA surgery. One patient had revision surgery for cup loosening that occurred at 32 months postoperatively. The other patient had the liner exchange that occurred at 34 months postoperatively. Revision was attributed to cup loosening associated with poor bony quality. For 3 patients with an IPD, the diameters of their cups were 56 mm, 58 mm, 58 mm, respectively; the diameter of each person’s femoral head was 28 mm; the abduction and anteversion angles of their cups were 38 degrees and 16 degrees, 39 degrees and 17 degrees, and 40 degrees and 18 degrees, respectively. None of the patients had revision surgery for groin pain attributed to psoas impingement. No periprosthetic fracture, heterotopic ossification, or unbearable hip pain was observed, neither was any visible pattern of lower limb shortening.
Prosthesis-Related Complications.
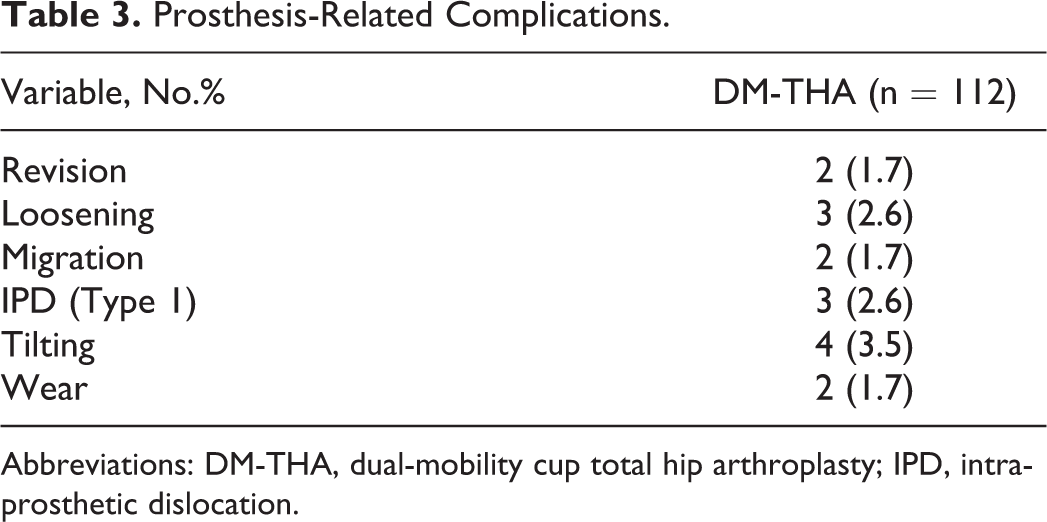
Abbreviations: DM-THA, dual-mobility cup total hip arthroplasty; IPD, intra-prosthetic dislocation.
Discussion
Our results may provide evidence that DM-THA performed initially for displaced osteoporotic FNFs in Chinese population yields favorable HHSs and a low rate of common orthopedic complications, in particular, a low dislocation rate. To the best of our knowledge, this is the largest study on DM-THA in Chinese population.
Complications of THA related to dislocation in particular were associated with substantial destruction of the surrounding tissue of the hip as well as an increased risk of revision, especially in patients with osteoporosis, potentially escalating the difficulty of additional interventions and posing a challenge for surgeons. 2,27 DM cups can include bearings involving a polyethylene liner between the prosthetic head and the outer metal shell, which has been increasingly used in primary or secondary THA for the management of FNFs, with a significantly reduced risk of dislocation and instability, which are regarded as causes of failure. 1,28 Thus, this technique can eventually yield favorable outcomes in the treatment of FNFs. 29 Whether hip instability decreases after THA is regarded as an essential indicator. 1,29 In our tertiary medical center, dislocation occurs from 0.5 to 8% after primary THA and up to 25% after revision THA. In recent years, there has been an increasing interest in the use of DM-THA as our clinical practice results show that they tend to provide good hip stability when used in primary displaced osteoporotic FNFs, with dislocation rates ranging from 0 to 4.0%. In the present study, the IPD rate is 2.6% (3/112). A previous report 16 demonstrated a high rate of IPD or instability following DM-THA. IPD or instability due to the design of acetabular cup occurs frequently in the fixed-bearing THA. 30 There is an increasing amount of evidence showing the efficacy of employing DM-THA as a primary or secondary treatment, with a low rate of IPD and instability. 7,17 Undeniably, concerns about the potential consequences of IPD induced by polyethylene liner wear due to a large femoral head, which can lead to IPD and the need for revision DM-THA, have been introduced by many authors, but there is a paucity of convincing evidence. 3,10,13,17,18
IPD is a rare but specific complication initiated by the excessive wear of the polyethylene retentive rim. 31 The failure mechanism of the IPD, which is associated with locking mechanism failure and is characterized by the snap-out of the femoral head from the polyethylene liner, is not yet entirely clear. 32,33 Impingement was involved in the occurrence of long-term polyethylene wear. 34 For DM cups with the concentric design, the wear leads to the generation of distance between the center of the femoral head and the center of rotation of the mobile liner. 31 In turn, the distance between the 2 centers of rotation intensifies the wear of the mobile liner, although the distance instigates a torque under loading which might be associated with a re-alignment of the mobile liner. 31,35 The factors associated with IPD remain unclear. 26,31,34 Previous reports 31,34 showed that unfavorable head-to-neck ratio, skirted femoral head, extensive fibrosis at the large articulation, and cup loosening or malposition (excessive abduction and / or excessive anteversion) tends to result in the occurrence of IPD. The strategy to manage long-term wear-related IPD are generally based on the regimens (cup removal, liner exchange, synovectomy) reported by Philippot et al. 26 Several authors have assessed the efficacy of DM-THA in this context. Bloemheuvel et al. 36 performed a study involving 215,953 FNFs treated using an uncemented DM cup and showed a low IPD rate (2%). Epinette et al. 3 reported 437 cases of displaced FNFs treated with DM-THA; 1 IPD (1.2%) was observed, and there was little evidence of prosthesis loosening or migration at a mean follow-up of 8 years. Nich et al. 11 performed a retrospective review of 82 patients (83 hips) aged older than 75 years with for FNFs treated with DM-THA and showed that DM-THA tends to be the most efficient treatment in preserving patients’ independence after fracture, with a satisfactory risk of IPD. Wheelton et al. 37 retrospectively reviewed prospectively collected data on consecutively included cases treated with DM cups to address instability induced by fixed-bearing prostheses; the authors reported acceptable early to mid-term results for the utilization of DM cups in managing continuing instability. Mohammed et al. 17 retrospectively assessed the outcomes of patients undergoing primary and revision THA with DM cups, and the early results for DM-THA performed to manage acute FNFs favorably reduced the risk of instability.
DM cups were introduced to reduce the risk of THA. 38 A growing but still very limited body of literature 28,29 has reviewed loosening and osteolysis behind the cup associated with IPD after DM-THA. DM cups are suspected of causing high rates of loosening and osteolysis due to coerced-mobile polyethylene being used in the design, but these rates remain unknown. 16 The previously reported rates of IPD induced by polyethylene liner wear are variable, ranging from 0% to 5.2%. 1,2,28,29 Although the use of DM cups with anatomical designs has prevented ilio-psoas tendon impingement, the factors promoting instability (large or small cups) remain unclear. 17,18,23,30 The available literature regarding the application of DM cups, even with non-modular DM cups, are extremely promising. 1,7,10,13 Indeed, the main cause of failure with “non-modular” DM cups is excessive wear, but prosthetic loosening has also been reported to occur, even though screws were included to increase the strength of fixation. 3,28,29
When interpreting the results of this study, several limitations should be acknowledged. Firstly, this is a retrospective study that involves all the issues inherent in this approach. Secondly, a lack of control group of individuals treated using THA with a fixed-bearing prosthesis. Nevertheless, this type of fixed-bearing THA has been well reported in the published literature. Thirdly, metal junctions subject to fretting corrosion is less involved in the observation of results. However, prosthesis instability can be to some extent the result of fretting corrosion. Fourthly, only 1 specific type of DM using uncemented fixation was assessed that precludes generalization of our findings.
Conclusions
The results reported in this study may support a growing body of evidence that DM-THA is associated with favorable functional outcomes and a low rate of common orthopedic complications in the treatment of displaced osteoporotic FNFs in Chinese population. We explore the potential clinical benefits in patients, including minimization of the risk of instability following DM-THA. Whether DM cups can replace fixed bearings has been reported as a concern by a host of authors. 1,7,13 Active patients with displaced osteoporotic FNFs, even in the absence of a clear risk factor for IPD, prefer to minimize the risk of IPD of the hip and return to all physical activities as soon as possible. In this context, DM-THA may be a priority for internal fixation.
Footnotes
Authors’ Note
Zhenfa Zhang, Guixing Xu, Lei Cao, and Wei Sun contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.