
Abstract
Study design:
The study was a retrospective cohort analysis for a 41 month period; from January 2013 to May 2016.
Introduction:
It is suggested that patients following a distal radius fracture (DRF) achieve a comparable outcome at 3 and 6 months post surgery regardless of the time they begin mobilization. In previous studies there has been limited analysis of outcomes within the initial 3 months: functional return, time taken from work and use of therapy resources are key outcomes which have not formally been investigated in previous studies.
Purpose of the study:
To analyze short term outcomes of patients following open reduction internal fixation (ORIF) for a DRF.
Methods:
A retrospective cohort analysis was conducted to determine primarily if there is a difference in time from work, number of therapy appointments, cost of therapy materials, time to discharge from therapy and secondarily range of motion (ROM) and grip strength (GS); when measured in patients who begin mobilization prior to 2 weeks compared to those who begin mobilization at 4 or greater weeks post surgery.
Results:
Patients mobilized early were discharged from hand therapy significantly quicker (p = 0.033) and returned to work significantly faster (p = 0.019) than those mobilized later. Patients who began mobilization at 2 weeks or earlier post surgery had significantly greater wrist extension/flexion arc at 4 weeks (p < 0.001) and 6 weeks (p < 0.001) and rotation at 4 weeks (p < 0.001).
Conclusions:
Patients who begin mobilization at 2 weeks or earlier following ORIF for a DRF will lose less time from work and will be discharged sooner from hand therapy. They will additionally have increased ROM in the early post surgery phase.
Introduction
Distal radius fractures (DRF) occur frequently, predominantly in those aged over 50; 1 incurring a large cost to medical systems. A proportion of DRF will require surgical fixation to achieve fracture stability and improve functional outcome. 2 An open reduction internal fixation (ORIF) with a volar locking plate (VLP) is currently the most common surgical procedure for a DRF with dorsal displacement. 1 In this specific patient population studies have shown comparable range of motion (ROM) and grip strength (GS) outcomes at 3 and 6 months post-surgery; regardless of the specific time they begin to mobilize. 3,4 Limited studies have investigated therapy time, use of therapy resources or lost time from work in the short term. These are also important aspects for the quality of life of the patient and a paying health provider.
Background
A distal radius fracture (DRF) is defined as a fracture occurring in the distal radius within 3 cm of the radio-carpal joint. 2 DRF are one of the most common fractures that occur in adults, accounting for approximately 15% of all fractures. 5 The incidence is increasing with an aging population. It is predicted that wrist fractures will increase by 25% in the next 4 years in people aged over 50. 1 A large percentage of the annual health cost is utilized by DRF patients; as a result of the initial assessment and investigation, surgery, treatment materials, therapy costs and time at work lost. The determination of the most efficient and effective care available is of benefit to the patient and health provider combined.
Surgery offers an obvious increased potential risk of infection and soft tissue damage, therefore internal or external fixation is reserved for more complex injuries. Fracture fixation using a VLP is currently the most common surgical treatment for this population. 1,6 Studies by McCamley et al, 6 Wigg et al, 7 Wilcke et al. 8 and Rozental et al. 9 have compared VLP to other fixation methods (external fixation, k wires, non-locking plates and bridging external fixation). These studies indicate that earlier function is obtained if a VLP is used surgically.
Early movement post surgery is beneficial in prevention of adherence of the tendons to the metal work or skin, 10 reducing joint adhesions and finger stiffness, 11 reducing neural tightness, 12 and preventing unnecessary muscle atrophy. It has been shown that patients with finger stiffness (following a DRF) have a greater pain intensity score and disability than those without stiffness. 11 Motion will aid reduction of swelling and stiffness that is a result of oedema. This enables the patient to experience a return of motion to the hand; improved motion will allow functional gains.
Therapy that is begun too early post surgery may disrupt the inflammatory phase and early proliferative phase of healing. 13 Proliferation of the repair material peaks at approximately 2 to 3 weeks post surgery, 13 this is when the bulk of the scar tissue is formed. Beginning motion around this time will allow the collagen to respond favorably to the mechanical stress applied to it. Delaying motion for longer than this period may result in adherence of the soft tissues and joint stiffness. The optimum period to begin therapy post fracture and fracture fixation remains inconclusive, despite several small studies. 8,9,14 -16
Valdes 14 showed a significant difference in the amount of therapy visits between patients when mobilization began at 1 week or 6 weeks post operatively. Driessens et al. 4 did not show a difference in ROM or therapy appointments attended by participants when the late mobilization group began movement on average of 24 days post surgery. This potentially indicates the detrimental effects of immobilization may occur after this 24 day period.
Purpose of the Study
The purpose of this study was to assess short term outcomes of patients receiving hand therapy following volar ORIF for a DRF. The primary objective was to evaluate for any difference in return to work, time to discharge from therapy and cost of therapy resources. In addition to this evaluating objective outcomes of grip strength and range of motion.
Methods
Study Design
The study was a retrospective audit cohort analysis for a 41 month period from January 2013 to May 2016.
Participants and Setting
Participants were identified through an electronic coding system using trauma diagnosis codes (S234. Closed fracture radius and ulna, distal; S234E Closed fracture distal radius, intra-articular, other type; S234D Closed fracture distal radius, extra articular, other type; S232. Closed fracture of radius and ulna, shaft; S2341 colles’ fracture) from the database at a private outpatient Hand Therapy Clinic. Institutional approval was obtained for this project. Participants were included when over the age of 16 with a DRF that required volar ORIF. Patients mobilized between 2 weeks and 4 weeks post surgery were excluded to try and show an obvious effect of the immobilization. Other exclusions included: patients with bilateral fractures or patients with a previous injury that severely compromised the ROM and GS of the contralateral side e.g. a fusion. Patients with an ulna styloid fracture on the ipsilateral side were included.
Participants were referred to the Hand Therapy clinic by their surgeon or clinic registrar from 1 local operating hospital. The Hand Therapy clinic has 18 treating senior registered hand therapists across 5 satellite locations. Participants were scheduled for follow up appointments according to their clinical need as assessed by the treating therapist. Participants were retrospectively organized into Group A or B using time from surgery to mobilization in weeks (Figure 1.)

Treatment groups. Key: ORIF =Open reduction internal fixation, DRF= distal radius fracture.
Hand Therapy modalities were prescribed according to clinical need at the discretion of the treating therapist. This included a variety of options for wound and scar management, oedema management, splinting, home and work advice, exercises, home exercise programmes, strengthening, proprioceptive retraining and return to sport or function specific training.
Outcomes
Demographic information was collected from the electronic patient records and included age, gender, hand dominance, operated side and occupation. ROM was collected from clinical notes at 2, 4 and 6 weeks, and 3 months post surgery when available. GS was collected at 6 weeks and 3 months post surgery when available. Number of treatments attended, cost of therapy materials used, time calculated in days until return to work and time (in days) until discharge from therapy was collected from the electronic clinical notes. The time to surgery was calculated in days from the date of injury to the date of surgery. Hand dominance, side of surgery and occupation was identified from clinical notes when available. Activity level was determined by the manual reviewer through assessment of the subjective notes. Occupation and hobbies were assessed and patients were grouped into high and low levels of functional upper limb demand. Patients who had an occupation that was heavy work (for example a manual laborer or builder), or who had a hobby that involved repeated upper limb motion (for example tennis) were categorized as high function. Patients who had a sedentary or desk based occupation and hobbies involving mostly lower limb activity (for example walking) were categorized as low function.
Procedure
Patients were identified by review of clinical notes. To ensure patients’ privacy and confidentiality, all clinical data was de-identified and converted into a non-identifiable format by the same member of the research team conducting the manual review. All available information from patient’s notes was entered into an electronic database for analysis. The study database was password secured and accessible only to the primary research team.
ROM is frequently used to identify change and evaluate ongoing treatment. It is widely used as an outcome measure to define the effectiveness of therapeutic and surgical interventions. 17 Extension and flexion of the radio carpal joint was measured by a 180° goniometer, using the volar method. 18 In extension the goniometer arms were placed in the palm in line with the third metacarpal, and mid volar forearm. In flexion the goniometer was placed on the dorsum of the hand in line with the third metacarpal and mid dorsal forearm. Rotational measurements were performed with the use of a wrist inclinometer – see Figure 2 (Baseline Measurement Instrument, Fabrication Enterprises, Inc. White Plains, New York 10602, and USA). The dial of the inclinometer reads an angle which is relative to the line of gravity (therefore fixed). The accuracy of inclinometers has been evaluated with x-ray angles and shows excellent correlation (r < 0.9997 and p < 0.05). 19 Repeated measures with inclinometers have also been shown to provide reliable results. 20 In this study the participant was asked to be seated with elbow by their side and elbow at 90° of flexion. The participant began in forearm neutral while holding the inclinometer and then pronated to end of range where the therapist recorded the ROM in degrees and then repeated into supination.

Wrist Inclinometer: Baseline Measurement Instrument, Fabrication Enterprises, Inc. White Plains, New York 10602, and USA.
GS was measured by therapists when clinically appropriate but not prior to 6 weeks post surgery. GS measures were recorded by therapists in subsequent therapy sessions when pertinent to patient treatment. GS is a quick and practical measure of hand impairment and function. 21,22 GS in the clinic is measured with a Sammons Preston, Inc. Dynamometer (Jamar, Sammons Preston US) in handle setting 2, according to the American Society of Hand Therapists (ASHT) guidelines on bilateral hands. 23 One measure on each side was recorded. 24 The surgical side measure (in Kilograms) was divided by the unaffected side and reported as a percentage of GS; this reduced inter- subject variability.
The number of therapy appointments attended was counted from the electronic patient notes. Cost of materials used for each patient and cost of therapist time is calculated as a total by the electronic system as it is billed to the treatment provider. Time until discharge was calculated in days, as time from surgery until final HT appointment. Participants attended until they had achieved an adequate level of function as determined by the treating therapist and patient; or they were referred onward due to unsatisfactory outcome.
Data Analysis and Results
A total of 378 participants were identified. Following review of patient notes those patients that did not meet the inclusion criteria or who were not from the specific local operating hospital were removed. Forty participants remained in the study. The majority of exclusions was related to patients not being from the specified study hospital. Participants included 12 males and 28 females between the ages of 16 years and 88 years. Table 1 provides a summary of patient demographic data. A total of 19 patients began therapy before or at 2 weeks post surgery (Group A). Twenty-one patients began therapy at or after 4 weeks post surgery (Group B). Following surgery patients receive an appointment ranging from 1 to 2 weeks at the Outpatient Orthopaedic Department. Within this appointment patients have a wound review and consultation with an Orthopaedic specialist. The patients are referred for therapy based on the referring clinician’s preference of mobilization time. Patients contact the Hand Therapy clinic to make an appointment. The variability in this process and availability of appointment times (for Orthopaedics and Hand Therapy) is what makes the initial mobilization time so variable. The length of time before mobilization was not specified by the surgeons relating to fracture complexity or complications. Group A had 15 female patients and 4 male, with an average age of 51 years. Group B had 13 female patients and 8 male with an average age of 56 years. Group A had an average time from fracture to surgery of 7 days, and Group B of 6 days. Group A had ten dominant sided DRF operated on; Group B had 11 dominant sides operated.
Key: M: F = Male to Female Ratio. Age Calculated as a Mean in years. * = P value 0.4029.

ROM for Groups A and B are presented in Table 2. Active flexion and extension were added as a total arc of motion, and pronation and supination as an arc of active rotation. At 4 weeks Group A had significantly better ROM than group B with 49° greater active extension / flexion arc and 81° greater rotation. At 6 weeks Group A continues to demonstrate significantly better ROM than Group B with a 40° greater extension / flexion arc and a 64° greater arc of rotation. At 3 months post surgery ROM of the 2 groups was similar; Group A demonstrated a 12° greater active extension / flexion arc and 11° greater active rotation arc.
Key: E/F Total Degrees of Active Extension and Flexion Measurement Combined in Degrees, Rotation = total Degrees of Active Pronation and Supination Measurement Combined in Degrees. N = number of Patients whose Measurements were Recorded. * = 2 Patients had Measures not Completed and 9 Patients Remained in POP Until 6 Weeks or over. + = Missed Data at this Point Due to Patients Already Discharged from Therapy. CI = Confidence Interval.

Abbreviation: GS, Grip strength; NA, not applicable.
The GS (See Table 2) of Group A measured at 6 weeks was 59% of the unaffected side and 40% in Group B. At 3 months GS was 85% in Group A and 59% in Group B. These differences were not significant. Average return to work (RTW) in days was significantly shorter (p = 0.0193) for Group A with 34 days than for Group B at 79 days.
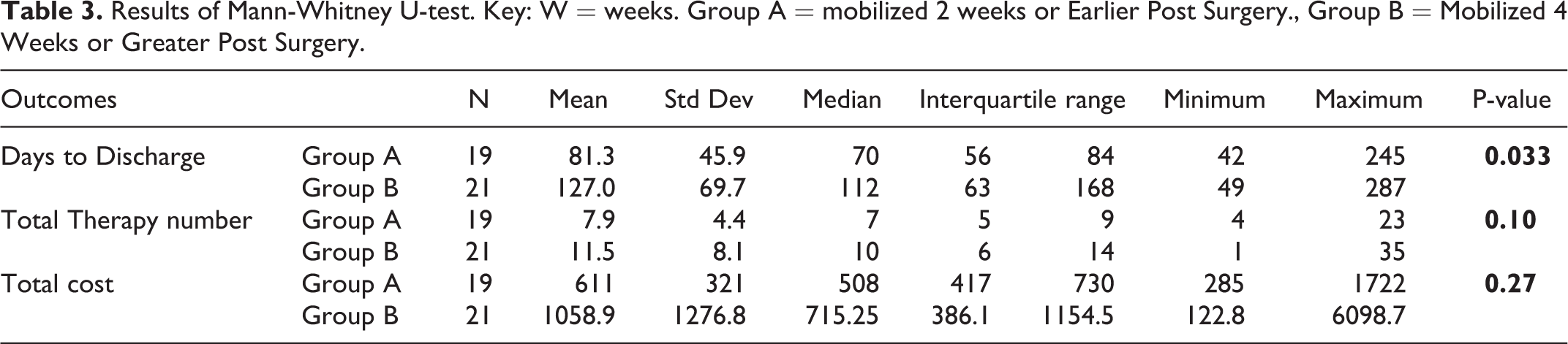
The average number of days from surgery to discharge from therapy, number of therapy sessions and total hand therapy treatment cost are displayed in Table 3. A Mann-Whitney U-test was used to compare differences across the groups. The days to discharge was significantly higher (p = 0.033) in Group B (127 days) compared to Group A (81 days). The average number of treatments utilized by group B was higher (11.5) than Group A (8) but this difference was not significant. The total mean therapy cost which included therapist time and materials was higher in Group B ($1058.9) compared to Group A ($611), but this difference was not statistically significant.
Results of Mann-Whitney U-test. Key: W = weeks. Group A = mobilized 2 weeks or Earlier Post Surgery., Group B = Mobilized 4 Weeks or Greater Post Surgery.
Missed data is presented in Table 2. In addition, RTW was documented in 13 patients in Group A with five retirees or unemployed; and 11 patients in Group B, 6 of those retired or unemployed. In Group B 3 patients developed Complex Regional Pain syndrome which was managed with therapy and medication. There were no documented complications in Group A.
Discussion
This retrospective audit analyzed patients beginning mobilization before 2 weeks (Group A) or at 4 weeks or greater (Group B) following surgery (ORIF) for a DRF. The results show patients mobilized earlier will RTW quicker and will be discharged from hand therapy significantly earlier than those mobilized at 4 weeks or greater. In addition to this, patient’s who begin mobilization and hand therapy 2 weeks or earlier post surgery have a significantly greater wrist extension / flexion arc at 4 and 6 weeks and significantly greater rotation at 4 weeks.
The study groups had comparable patient numbers (p = 0.40) and male to female ratios between groups. In this study 43% of operated patients were males; comparable with Valdes 14 DRF study of 38%. The average patient age within groups (A = 51 years and B = 56 years) was comparable (P value 0.4029). This corresponds with studies showing the majority of these fractures occur in people over the age of 50 years. The groups were comparable in hand dominance, proportion undergoing surgery to the dominant side and ratios of heavy versus light functional activities. Time to surgery was similar in both groups.
Quadlbauer et al. 25 studied a comparable patient population (ORIF for DRF) in which patients began mobilization at 1 week or five weeks post surgery. The early mobilization group had a significantly better flexion to extension arc until 9 weeks post surgery. Valdes 14 investigated patients beginning motion early (1 week post surgery) and late (6 weeks) following ORIF for a DRF. Patients in the early mobilization group were deemed to achieve a functional range of combined radio-carpal motion (40° extension and 40° flexion) and forearm rotation (50° pronation and 50° supination) 37 days earlier (p < 0.005) than the late mobilization group. In the current study Group A (mobilization before or at 2 weeks) achieved this combined functional ROM at 4 weeks post surgery; Group B (mobilization at or after 4 weeks) achieved this only at 3 months. The results of the current study therefore are consistent with the results of previous studies; demonstrating a delay in return of ROM when mobilization is delayed greater than 4 weeks.
An additional comparable study was conducted by Watson et al. 26 The randomized controlled trial compared the effects of mobilization at 1, 3 and 6 weeks post ORIF for a DRF. There was a beneficial early reduction of pain within the first 6 weeks for the groups that began mobilization at 1 or 3 weeks post surgery. The 1 week (p = 0.003) and 3 week (P = 0.001) groups had significantly lower Patient-Rated Wrist Evaluation scores (measuring pain and disability in activities of daily living) in comparison to the 6 week group; at 6 weeks post surgery. The earlier mobilization groups also had significantly greater wrist extension motion at 6 weeks. The recurring concept between studies is that the beneficial effects of early mobilization are diminished at 3 and 6 months post surgery. 25,26 The initial advantages of the early mobilization have significant positive effects on a patient’s function, well being and finances.
In isolation wrist extension is a functionally relevant objective measure because tasks are best performed with the wrist in 40-45° of extension. 27 Considering the extension measure alone, Group A achieved a functional wrist extension (46°) at 4 weeks; Group B again not until 3 months. The wrist extension ROM difference between groups indicates that mobilization of an ORIF DRF greater than 4 weeks delays the achievement of a functional ROM.
Previous studies have compared GS to the subjective evaluation of ability to perform functional tasks. Nordenskiold 28 reported a significant correlation between reduced grip and perceived difficulties with certain ADL. Karnezi and Fragkiadakis 29 report that GS in patients post DRF is a better predictor of self-reported outcome than ROM (flexion – extension) of the wrist. Chung and Haas 30 report GS to be the best predictor of satisfaction post surgery in patients who have had a VLP. Therefore increased GS will improve the quality of a patient’s function. In this study at 6 weeks and at 3 months post surgery Group A had greater GS than Group B, although this difference was not statistically significant. The higher GS of Group A may suggest improved function at the 6 week point; a greater sample size would be required to determine this. Quadlbauer et al. 25 showed the improved GS in the early mobilization group was significantly greater than the late mobilization group until 6 months post surgery.
Previous studies 4,16 have shown at 3 months post surgery patients within early and late mobilization groups achieve similar ROM and GS results. There were no significant differences in ROM and GS measures between groups within this study also. The variance in outcomes between the treatment groups is greatest within the first 3 months. Early mobilization allows patients to be discharged from therapy significantly (p = 0.033) earlier. At 3 months post surgery 58% of Group A patients had been discharged, in comparison to 19% of Group B. An early discharge allows patients to resume work, hobbies and their social life without the time and financial requirement of attending Hand Therapy. Group B required on average a further 46 days of therapy. The additional therapy time equated to Group B requiring on average 3 and a half additional 30 minute therapy appointments to achieve an acceptable functional outcome for discharge. Although this is not significant it is consistent with the Valdes 14 study in which the average number of therapy visits in the early mobilization group (commencing at 1 week post operatively) was 6.57 and 17 visits for the late mobilization (commencing after 6 weeks mobilization). These results suggest that the later mobilization is commenced post surgery, the higher number of therapy appointments required to achieve function. Any increased therapy time incurs an additional cost to the treatment provider. The current study showed an overall mean cost of therapy time and materials of $611 NZD for Group A and $1058 NZD for each patient in Group B. The cost difference supports the argument that late mobilization (after 4 weeks) increases patient therapy time and cost. In order to determine if a significant difference between the groups exists with regard to cost, a population of 160 patients would be required
The length of time taken by patients to return to work was greater in Group B by 45 days on average. No known previous studies have analyzed this outcome measure. The sizable difference in the RTW time between the groups would have substantial financial implications for workers, employers and insurers. More than half of the population that sustain a DRF are in employment at the time of their injury. 31 MacDermid et al. 32 reported lost time from work as an average of 9.2 weeks (64.4 days) in patients following non-surgical DRF. Group A only required 34 days and Group B 79 days on average to return to work and Group B had a similar length of time to that reported by MacDermid et al., 32 due to the comparable duration of immobilization. Patients who have an occupation of high demand are at risk of increased time from work. 32 The proportion of patients with high activity levels were similar in each group; strengthening the evidence that the immobilization rather than the nature of their occupation is the element increasing time from work.
Complications
It is noteworthy that 3 patients in Group B were treated for complex regional pain syndrome (CRPS). CRPS is a pain condition that is disproportionate to the inciting event with possible symptoms of burning pain, hyperesthesia, temperature asymmetry, vasomotor or sudometer changes. 33 During immobilization, changes in the cortical processing and organization in the central nervous system potentially allow the development and / or maintenance of CRPS. 34 The potential beneficial effect of early mobilization post surgery may have reduced this complication in Group A.
Clinical Implications
This study indicates that mobilization before 2 weeks following surgery has important benefits for the patient and the funder of therapy. Patients mobilized prior to 2 weeks demonstrate a more rapid recovery of functional ROM at 4 and 6 weeks post surgery. These patients return to work 45 days earlier than those patients mobilized after 4 weeks. Early mobilization results in reduced disruption to daily activities, less attendance at therapy appointments and patients are discharged with a satisfactory level of function on average 46 days earlier. The paying treatment provider will have reduced cost in therapy time and resources. This study data could be used to facilitate effective communication with operating departments about timely referral and expectations for patients within the initial 3 months post surgery.
Study Strengths and Limitations
The strength of this study is that it is a ‘true to life’ pragmatic reflection of therapy outcomes. Limitations of this study include non-randomization of participants, no blinding of assessors and that the data was collected retrospectively. There is a possible selection bias for those who are more motivated to RTW and function quicker may seek an earlier HT appointment than other patients. The generalisability of the research may be limited due to the data being collected from a single referral source of 1 therapy clinic. A further limitation may include the involvement of multiple surgeons and the varying skills of operating surgeons.
Conclusion
The retrospective audit results show that patients that begin mobilization before 2 weeks following ORIF for a DRF will have recovery of functional ROM sooner, significantly fewer days until discharge from hand therapy and a quicker RTW than those mobilized at 4 or greater weeks post surgery. These benefits enable the patient to resume function, hobbies and a return to the financial benefits of working quickly. An advantage for the treatment provider is that patients mobilizing before 2 weeks post surgery may require a reduced number of hand therapy appointments and therefore a reduction in cost of therapist time and therapy materials used. Within the current health system this would help with meeting financial constraints. Health research has focused more on psychosocial factors and patient rated outcomes, these factors are improved in patients mobilized earlier following surgery. There needs to be a bigger sample size in order to determine if these factors are significant between groups. A prospective randomized group study would be of benefit to determine if there is a critical time point for mobilization post surgery and improving short term outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.