
Abstract
Introduction:
A fracture liaison service (FLS) is a coordinated system of care that streamlines osteoporosis management in the orthopaedic setting and can serve as an effective form of secondary preventative care in these patients. The present work reviews the available evidence regarding the impact of fracture liaison services on clinical outcomes.
Methods:
The literature was reviewed for studies reporting changes in the rates of bone mineral density scanning (DXA), antiresorptive therapy, new minimum trauma fractures, and mortality between cohorts with access to an FLS or not. Studies including intention to treat level data were retained. A Medline search for “fracture liaison” OR “secondary fracture prevention” produced 146 results, 98 were excluded based on the abstract, 38 were excluded based on full-text review. Ten level III studies encompassing 48,045 patients were included, of which 5 studies encompassing 7,086 were analyzed. Odds-ratios for DXA and anti-osteoporosis pharmacotherapy rates were calculated from data. Fixed and random effects analyses were performed using the Mantel-Haenszel method.
Results:
Four studies reported, on average, a 6-fold improvement in DXA scanning rates (Figure 1). Six studies reported, on average, a 3-fold improvement in antiresorptive therapy rates (Figure 2). Four large studies reported significant reductions in the rate of new fractures using time-dependent Cox proportional hazards models at 12 months (HR = 0.84, 0.95), 24 months (HR = 0.44, 0.65), and 36 months (HR = 0.67). Five large studies reported mortality improvements using time-dependent Cox proportional hazards models at 12 months (HR = 0.88, 0.84, 0.81) and 24 months (HR = 0.65, 0.67).
Conclusions:
The findings suggest that fracture liaison services improve rates of DXA scanning and antiresorptive therapy as well as reductions in the rates of new fractures and mortality among patients seen following minimum trauma fractures across many time points.
Keywords
Introduction
A minimum trauma fracture is one that occurs due to a fall from standing height or other low energy mechanism. The impact of these fractures on patients and communities can be devastating. The mortality rate is 10% within 1 month and 24% within 1 year of a serious fracture 1 This rate is 33% within 1 year for femoral neck fractures. 1 Up to 50% of patients who sustain minimum trauma hip fractures do not return to their pre-morbid level of mobility. 2 Activities of daily living become a challenge as patients struggle to ambulate. Eighty-five percent of hip fracture patients require assistance with walking and 20% will have needs that necessitate nursing home level of care. 3 -5 The initial fall is frequently a harbinger of subsequent deterioration, as these patients are 2 to 4 times more likely to have a subsequent hip fracture. Ten percent of these patients experience another fracture within 1 year. 6 In patients ages 60 and older, the relative risk of a subsequent fracture is 1.95 in women and 3.45 in men. 6 The risk of mortality is increased in patients with subsequent fractures by 93%. 7
In addition to being physically and emotionally challenging for patients, minimum trauma fractures are also enormously expensive for healthcare systems around the world. They are projected to cost Europe 37 billion Euros by 2025 and China $12.5 billion US dollars by 2020. 8 In the United States, the cost of minimum trauma fractures is projected to exceed $25.3 billion US dollars by 2025. 9
The high rate of initial and recurrent minimum trauma fractures is due, in part, to the low implementation of guidelines designed to prevent fractures in osteoporotic patients. Barriers to successful implementation include the cost of diagnosis and therapy, concerns about medications, and the lack of clarity regarding who is responsible for osteoporosis care once a fracture has occurred. 10 Osteoporosis treatments can reduce fractures by up to half, but 50% of women and 90% of men with minimum trauma fractures are not treated with any anti-fracture medication. 11 -13 Less than 25% of older patients with fractures receive adequate vitamin D Supplementation. 14,15
Fracture liaison services (FLS) are designed to bridge this gap. FLS programs have been defined in various ways. In this article, we focus on what Ganda et al. define as a Type A FLS, namely those that evaluate all patients presenting to a health system with new fractures after a prespecified age and initiate treatment when appropriate. 16 They identify patients who experience an index minimum trauma fracture, assess their bone mineral density, and implement appropriate therapy to prevent subsequent fractures as well as the associated morbidity and mortality. 17 Such services are increasingly regarded as the gold standard in secondary fracture prevention. 18 -21 The American Orthopaedic Association (AOA) has advocated for widespread adoption of the Type A FLS model through its “Own the Bone” campaign. 22 As of 2018, 240 FLS sites have been established in the United States through Own the Bone. 22 The present study systematically examines the impact of FLS programs on rates of DXA scanning, anti-osteoporosis prescribing, rate of new fractures, and overall mortality based on the most rigorous available evidence.
Materials and Methods
This was a protocol-driven systematic review and meta-analysis assessing the impact of FLS programs on DXA scanning, anti-osteoporosis prescribing, the rate of new fractures (refracture), mortality, and hospital readmissions. We adhered to the PICO systematic search framework recommended by the Cochrane Collaboration. 23
Eligibility Criteria
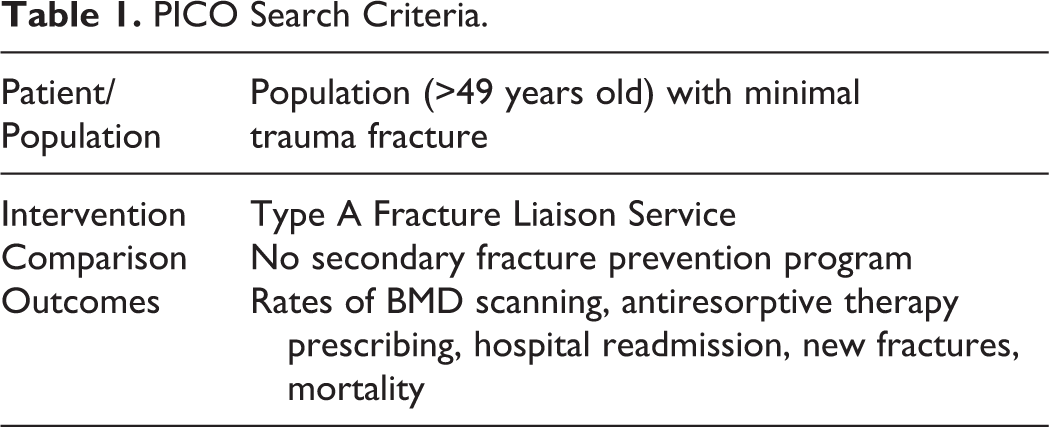
Eligible studies were comparative studies that examined patient outcomes either pre- and post fracture liaison service implementation at a single institution or between 2 different institutions that did or did not have a fracture liaison service. The patients in these studies were adults over the age of 49 who had sustained a fracture due to a fall from standing height or other low energy mechanism. Included studies evaluated at least one of the following as outcomes following the low-impact fracture: rate of DXA scanning, anti-osteoporosis pharmacotherapy prescribing, refracture, mortality, and hospital readmission (Table 1). All eligible studies were included regardless of size. Strictly descriptive articles (e.g. reviews, commentaries) were excluded from this analysis.
PICO Search Criteria.
Study Identification
An electronic search of the English medical literature in Medline was conducted. The Boolean search “‘fracture liaison’ OR ‘secondary fracture prevention’” was employed, yielding 146 non-duplicate citations. Two authors independently reviewed each article and determined its inclusion status, with conflicts resolved through consensus. Ninety-eight articles were excluded after the title or abstract screen. Forty-eight candidate articles underwent independent full-text review by 2 authors. Following the application of the inclusion and exclusion criteria, 11 articles were retained for this analysis. All included studies produced level III evidence.
Data Selection
The authors independently extracted data from full-text versions of eligible studies with conflicts being resolved by consensus. Study characteristics included study duration and the sample sizes at the sites with and without fracture liaison programs. The statistical tests performed, p-value, and test statistic were collected for the rate of DXA scanning, anti-osteoporosis pharmacotherapy administration, refracture, mortality, and readmission. The loss to follow-up, intention to treat, and imbalance at baseline of the studies was recognized.
Statistical Analysis
Odds ratios for DXA and antiresorptive therapy rates were calculated from study data. Random effects meta-analyses were performed using the Mantel-Haenszel method through the “meta” package in R version 3.3.1 24,25 Random effects models were chosen to better account for inter-country and inter-institutional variations in the specific details of FLS implementation.
Results
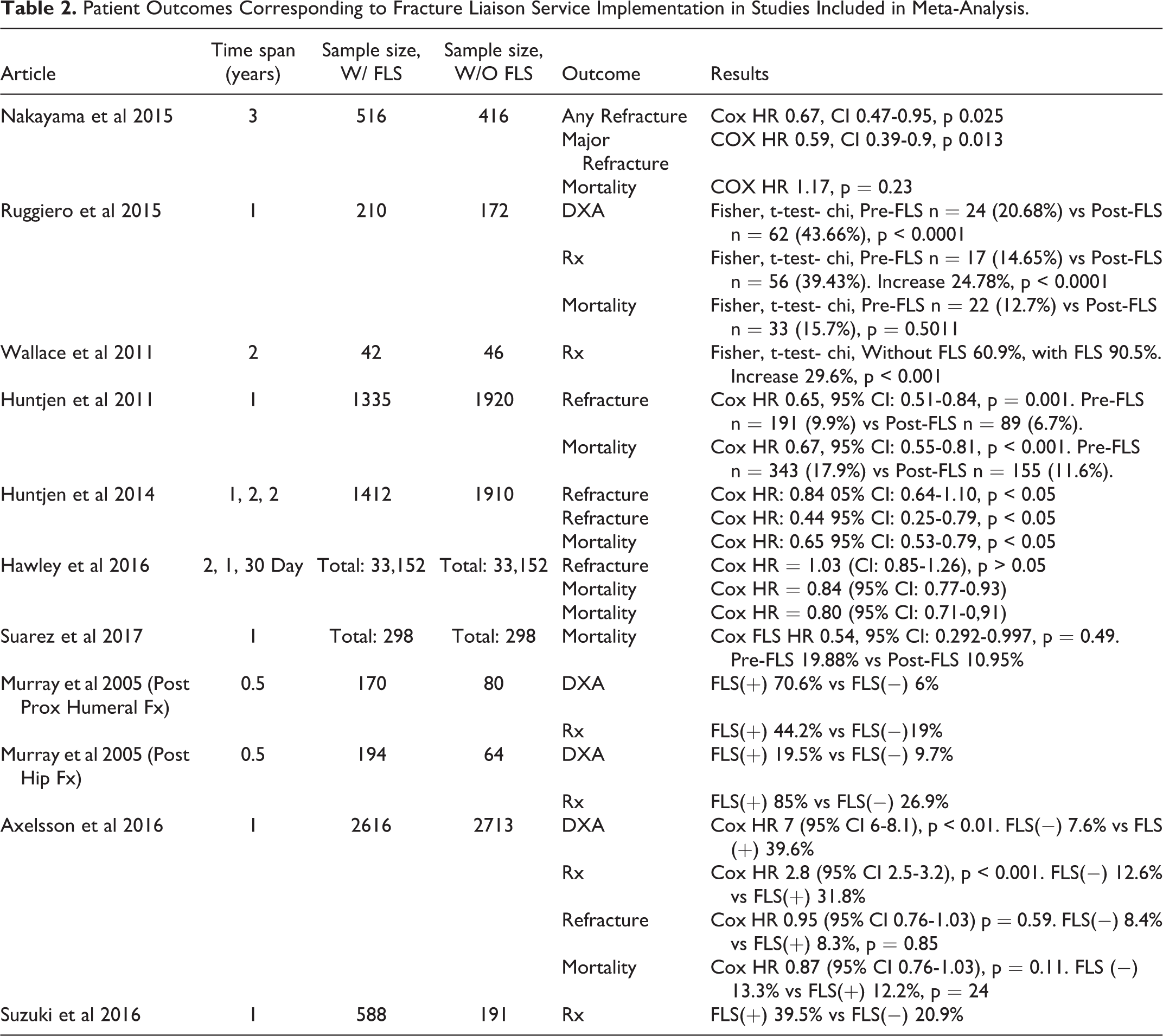
This study is a meta-analysis of 10 studies reporting the implementation of FLS programs and the corresponding patient outcomes in terms of DXA scanning, antiresorptive therapy, refracture, mortality, and readmission rates. All included studies were observational. They evaluated either a single institution pre- and post-intervention or compared 2 comparable institutions that did and did not have an FLS. Included studies encompassed 48,045 total patients, with the sample sizes of individual studies ranging from 88 to 5,239 patients. Table 2 presents a list of included studies and their significant outcomes.
Patient Outcomes Corresponding to Fracture Liaison Service Implementation in Studies Included in Meta-Analysis.
DXA Scanning
Four analyses from 3 studies reported, on average, a 7.5-fold (OR 7.51, 95% CI 3.64-15.48) improvement in DXA scanning rates (Figure 1). In a large Swedish study examining the impact of a resource limited FLS, Axelsson et al. report the overall proportion of patients being evaluated with DXA following a fracture increased from 7.6% of 2713 patients in the control group to 39.6% of 2616 patients in the FLS-intervention group (p < 0.001) 24 Axelsson et al. also observed a decrease in time to DXA scanning after initial fracture from 133 ± 119 days to 85 ± 67 days (p < 0.001) associated with FLS implementation. A British nurse and physician led FLS improved DXA scanning rates among individuals 50 and older following hip fracture from 9.7% to 19.5% (N = 282) and from 6.0% to 70.6% following humerus fracture (N = 181). 26 Ruggiero et al. found a nurse-led Italian FLS significantly improved DXA scanning rates following fracture from 25 of 172 (14.5%) to 62 of 210 (47.6%) among individuals 65 and older (p < 0.001) 27 Wallace et al. report results from a UK based FLS that did not rely on DXA scans for osteoporosis diagnosis, showing one case (2%) who received a DXA scan in the FLS group and zero cases in the control group. 26 Wallace et al was excluded from the quantitative summary of DXA scans for reasons reviewed in the discussion section.

Improvement in DXA scanning rate with FLS implementation.
Anti-Osteoporosis Pharmacotherapy
Six analyses from 5 studies encompassing 7131 patients reported improvements in the rate of prescribing of pharmacotherapy for osteoporosis in the FLS group vs controls. Their results are quantitatively summarized using a random effects model in Figure 2.
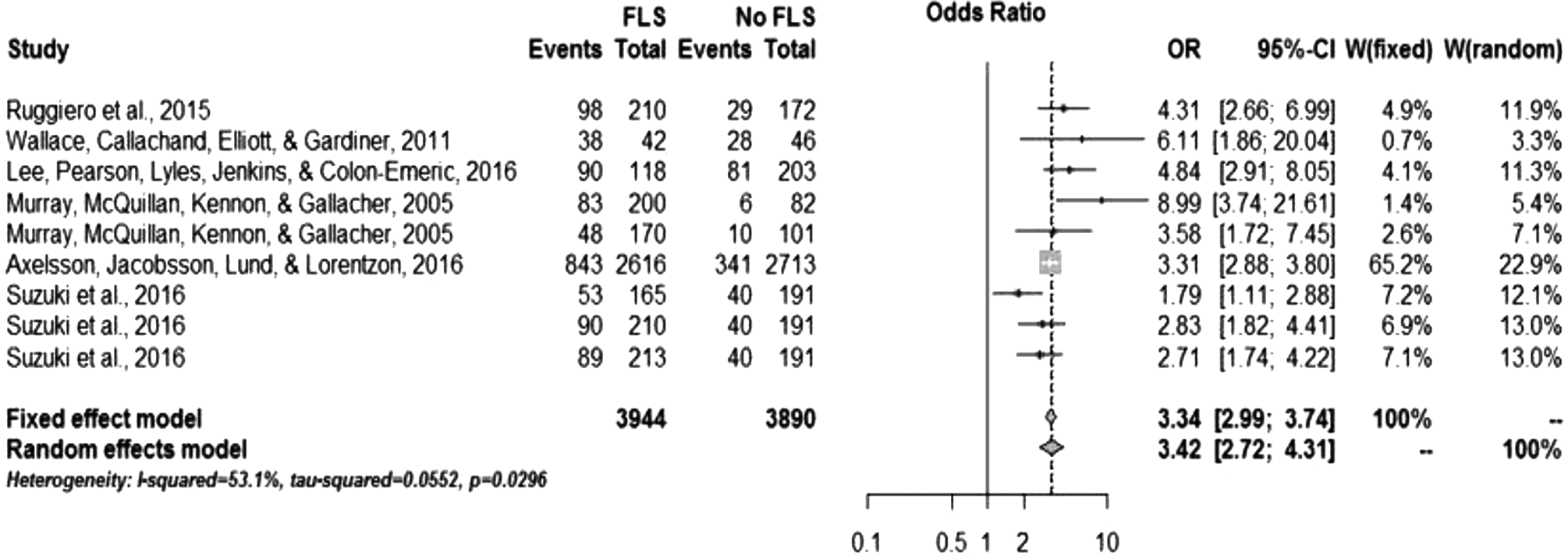
Improvement in antiresorptive pharmacotherapy prescribing rate with FLS implementation.
Axelsson et al showed that a Swedish minimal resource FLS increased the rate of pharmacological treatment following fracture from 12.6% to 31.8% (p < 0.001, N = 5329). 28 Ruggiero et al. reported a nurse-led Italian FLS increased the rate of pharmacological treatment following fracture from 17.1% to 48.5% among individuals 65 and older (N = 382). 29 Murray et al. report a British nurse and physician led FLS improved pharmacological treatment rates among individuals 50 and older following hip fracture from 49% to 88% (N = 282) and from 39% to 65% following humerus fracture (N = 181). 25 Wallace et al. showed that an orthogeriatrician led inpatient FLS in the UK improved pharmacological treatment rates at discharge following hip fracture among individuals 75 years and older from 61% to 91% compared to an institution without such a service (N = 88, p < 0.001). 28 A team-based FLS in Japan produced an improvement in the rate of pharmacological treatment at hospital discharge post hip fracture among individuals 65 and older from 21% at baseline (2009, n = 191) to 32% in the first full year of FLS operations (2012, n = 165), 43% in the second (2013, n = 210) and 42% in the third (2014, n = 213). 30
Refracture Rates
Six studies have reported the results of intention to treat analyses for changes in the rate of new fractures based on FLS implementation. Four of those studies analyzed their results using Cox proportional hazards models, with varying corrections for original fracture type, comorbidities, demographics, and time-dependency. Due to the differences in the models used by these studies and lack of available patient level data, their results are not suitable for meta-analysis.
In 2011, the Dutch group Huntjens et al. found that a nurse-led FLS service reduced their rate of new non-vertebral fractures at 2 years post-fracture from 9.9% to 6.7%, with a time adjusted hazard ratio of 0.65 (95% CI 0.51-0.84, p < 0.001, N = 3255) when considering all non-vertebral minimum trauma fractures. 7 They later replicated this finding using an inter-institutional comparison between their home hospital and a similar neighboring hospital, finding an improvement from crude improvement 6.8% to 6.7% with a time adjusted hazard ratio of 0.84 (0.64-1.10) at 12 months and 0.44 (95% CI 0.25-0.79, N = 3322) at 24 months for all nonvertebral fractures. 31 Both Dutch studies used a nurse coordinator and protocol based FLS model. In the latter study they found the trend was not statistically significant at 6 and 12 months but became significant at 15 months and continued to enlarge with time. A smaller, similar study by Nakayama et al. comparing an FLS hospital to a non-FLS hospital in Australia at 3 years post-fracture found a reduction in the rate of any new fracture from 16.8% to 12.2%, with a time adjusted hazard ratio of 0.67 (95% CI 0.47-0.95, p = 0.025, N = 931) and in the rate of new major osteoporotic fractures, defined as fractures at the hip, spine, femur, pelvis or humerus, from 12% to 8.2% (HR = 0.59, 95% CI 0.39-0.90, p = 0.013, N = 931) among patients with any type of initial fracture. 17 A large Swedish study by Axelsson et al found 1 year refracture rates of 8.3% to 8.4% with a fully adjusted hazard ratio of 0.95 (95% CI 0.79–1.14, p = 0.60, N = 5329) before and after implementation of a resource limited FLS among patients with hip, pelvis, spine, wrist, and ankle fractures. 27 Hawley et al. found no evidence of impact on time to second hip fracture following FLS intervention (HR 1.03, 95% CI 0.85-1.28) or orthogeriatrician appointment (HR 0.95, 95% CI 0.79-1.15). 30
Mortality
Seven studies have reported the results of intention to treat analyses for changes in all-cause mortality based on FLS implementation. Six of those studies analyzed their results using time-dependent Cox proportional hazards models, with varying corrections for fracture type, comorbidities, and demographics. Due to the differences in the models used by these studies and lack of available patient level data, their results are not suitable for meta-analysis. In 2011, a Dutch group found that a nurse-led FLS service reduced their institutional 2-year post-fracture mortality rate from 17.9% to 11.6% (HR = 0.67, N = 3255) when considering all non-vertebral minimum trauma fractures. 7 They later replicated this finding using an inter-institutional comparison between their home hospital and a similar neighboring hospital, finding an improvement from 12.3% to 11.5% (HR = 0.65, N = 3322) for all non-vertebral fractures. 31 A similar, smaller study comparing an FLS hospital to a non-FLS hospital in Australia found no statistically significant difference in 3 year post-fracture mortality after adjusting for age, gender, and fracture type (HR = 1.17, p = 0.23, N = 931) among patients with any type of fracture. 17 A large Swedish study (N = 5329) by Axelsson et al. reported 1 year post-fracture mortality rates in patients of 13.3% and 12.2% before and after implementation of a resource limited FLS, although this difference was not statistically significant among patients with hip, pelvis, spine, wrist, and ankle fractures as either a crude ratio (p = 0.22) or fully adjusted hazard ratio for time to mortality (HR = 0.88, 95% CI 0.76–1.03, p = 0.11). 27 A small (N = 298) Colombian study found an improvement in the 1-year post-fracture mortality rate among hip fracture patients from 20% to 11% (HR = 0.54) following implementation of an orthogeriatric service. 32 A nation-wide study (N = 33,152) in the UK by Hawley et al. found improvements in 1 year post fracture mortality rates in patients following implementation of either an FLS (HR = 0.84, 95% CI 0.75-0.87) or an orthogeriatric service (HR = 0.81, 95% CI 0.77-0.93).32 Hawley et al. report reductions in ageand sex-standardized 30-day mortality (HR = 0.73, 95% CI 0.65–0.82). They found the number of patients needed to treat to avoid one excess death at 30-days is 17 for an FLS intervention. A small (N = 382) Italian study by Ruggiero et al. reported crude 1 year post-fracture mortality rates among patients with proximal femur fractures before and after implementation of a multidisciplinary secondary fracture prevention program as 0.18 and 0.12 respectively (p = 0.50). 29
Readmissions
No studies were found reporting ITT results for hospital readmission.
Discussion
Fracture liaison service (FLS) implementation is a potent intervention for improving postfracture osteoporosis recognition and management in minimum trauma fracture patients. While several FLS models exist and details vary between countries and institutions, all FLS models focus on the use of a dedicated health professional who works to ensure minimum trauma fracture patients are screened for and, as appropriate, treated for osteoporosis. 20,21 Some of these models use a nurse coordinator to help orchestrate this care while others use an orthogeriatric physician or other dedicated healthcare professional to directly screen and treat these patients. In the United States, advanced care practitioners, such as nurse practitioners and physician assistants, often fill this role. 33 Depending on the model adopted, a key factor in optimizing the beneficial effects of an FLS may be the involvement of primary care physicians who monitor patients for continued adherence to treatment. Geriatricians are also frequently included to ensure that patients are receiving comprehensive and targeted care. Improvements in patient outcomes depend not only on the organizational aspects of a multidisciplinary team, but also on patients and their caregivers’ understanding of the deleterious consequences of minimum trauma fractures. Further studies are needed to analyze which components of FLS implementation are most effective. When analyzed holistically as a discrete intervention, we found FLS implementation was associated with statistically and clinically significant improvements in rates of DXA scanning and anti-osteoporosis prescribing as well as reductions in the rates of new fractures and overall mortality.
According to the World Health Organization, osteoporosis may only be diagnosed based on decreased bone mineral density relative to healthy controls on DXA scan. While the National Bone Health Alliance has challenged this standard, suggesting certain characteristic minimum trauma fracture patterns warrant a clinical diagnosis of osteoporosis, the WHO criteria remain the gold standard for osteoporosis diagnosis. 34 Given this dependence of osteoporosis diagnosis on DXA scanning, the rate of DXA scanning provides a robust measure to assess whether patients are being screened for osteoporosis after minimum trauma fractures. Wallace et al. was excluded from the quantitative summary of the impact of FLS implementation on DXA scanning both because only one patient in that study received a DXA scan and because they diagnosed osteoporosis clinically after fractures, rather than using a DXA scan. Because they clinically diagnosed osteoporosis in nearly all their fracture patients, DXA scans are not an adequate surrogate measure for how often patients are being worked-up for osteoporosis in that patient population. The remainder of our included studies, however, did use DXA scans as part of the formal workup for osteoporosis post-fracture and thus could be safely used as a surrogate measure for how often a complete workup was undertaken. We found 4 analyses from 3 level III studies that when analyzed collectively suggested patients who were seen for minimum trauma fractures at hospitals with an FLS were 7.5 times more likely (OR 7.5, 95% CI 3.6-15.5, p < 0.01) to receive a DXA scan than those who were seen at hospitals without an FLS. While this quantitative result is highly dependent on the rate of DXA scanning at the control hospital and details of the FLS model adopted, this result suggests a robust, statistically and clinically significant improvement in DXA scanning rates associated with FLS implementation.
Two core aspects of osteoporosis treatment are pharmacological treatment and supplementation of calcium and vitamin D. 35 Given concerns over the limited efficacy and potential harms associated with routine calcium and vitamin D supplementation, we opted to focus on pharmacological treatment of osteoporosis in this review. 15,36,37 Pharmacological treatment of osteoporosis was defined as initiation of any FDA or EMA approved medication for osteoporosis including a bisphosphonate, denosumab, teriparatide, calcitonin, raloxifene, or strontium ranelate. In 6 analyses over 5 studies we found a 3.6-fold (OR 3.6, 95% CI 2.8 – 4.8, p < 0.01) improvement in the rate of anti-osteoporosis prescribing associated with FLS implementation. This quantitative estimate should be interpreted as a robust demonstration of the statistically and clinically significant improvement in osteoporosis treatment rates associated with FLS implementation. The quantitative impact seen at any particular institution will vary based on the pre-existing treatment rate and the details of the FLS model implemented.
Bisphosphonates are the best researched and most commonly prescribed anti-osteoporosis drug class. The number needed to treat to prevent one hip fracture over 3 years with bisphosphonates is 20. 17 Compared to the number needed to treat with statin therapy to prevent a cardiovascular event in 5 years, 55, the benefit of initiating anti-osteoporotic treatment is impressive. 38 In level I clinical trials, bisphosphonates have been found to reduce not only the rate of new vertebral and non-vertebral fractures but also overall mortality. 11,35,39,40 The exact mechanism for this mortality benefit is unclear, although many attribute it to downstream effects of fracture prevention. 31 Other authors have contended that fracture prevention alone cannot explain the effect. 41 Fitting with this broader literature, we found FLS implementation was associated with downstream reductions in the rate of new fractures and overall mortality in several studies. Although some studies failed to demonstrate statistically significant differences, the overall trend was nevertheless clear.
Perhaps the most remarkable of these studies is Hawley et al., who reported a decrease in mortality associated with FLS implementation but failed to find a decrease in the rate of fractures of the opposite hip after an incident hip fracture in a (UK) National Health Service analysis. 42 This result persisted through fully adjusted time-dependent Cox proportional hazard modeling but also not only at the pre-planned 1-year follow-up period but also in a 3-year follow-up sensitivity analysis. Their result is difficult to explain, although it may be due to some peculiarity of their database or analysis, the fracture site they selected, increased survival producing more fractures, or poor adherence, several of which factors they suggest as possible explanations. In contrast the failure of Axelsson et al. and Huntjens et al (2014) to find statistically significant fracture reductions at 1-year post fracture is likely due to inadequate follow-up. 27,31 As Huntjens et al (2014) demonstrate, the impact of FLS implementation on fracture rates is time dependent. 28 This is consistent with the time-dependent impact of bisphosphonates on new fractures seen in clinical trials. 11 The results of Suzuki et al. also warrant discussion. 29 They recorded changes in refractures and pharmacological intervention as an FLS system was incrementally adopted over a period of 3 years post-implementation in comparison to a pre-implementation year. While simplified to a before-after comparison in the present review, their full results warrant the reader’s further consideration as they show incremental improvement as their system is built to full impact over time.
All types of minimum trauma fractures are associated with increased mortality risk, especially within the first 5 years. 43 As previously noted, bisphosphonates have been associated with a compensatory decrease in mortality rate, which may be partly independent of their effect on refracture rate. These observations provide a theoretical undergirding to support the observed positive impact of FLS implementation on mortality.
Nakayama et al produced perhaps the most striking result with regard to mortality reviewed in this paper. 17 They report increased mortality associated with the FLS hospital relative to its control, despite a decrease in major fractures. The increased mortality that they observe is reduced to a non-statistically significant trend by controlling for age and initial fracture location. They also observe a hip fracture rate in that hospital of 39% vs 19% in the control hospital. Given this observation, the higher unadjusted mortality observed in their FLS hospital relative to its control may be due to higher general medical acuity of the patients seen at that hospital. That higher acuity could mask any nascent mortality benefit that might otherwise be observed. Therefore, this study should not be interpreted as a strong counter example to the 4 larger level III studies which demonstrated mortality benefits associated with FLS implementation. The present study is unique in that we address multiple patient outcomes. While other meta-analyses have examined 1 or 2 outcomes in relationship to the implementation of an FLS, we have examined 5. This work is also unique in that every manuscript we selected had a distinct group of patients who had access to an FLS and a second set who did not. Several important limitations apply to this review. First, this review focused exclusively on cohort comparison studies that examined outcomes from FLS programs using a control (no-FLS) condition and either conducted their analyses according to the intention to treat principle or provided raw data that could be used to conduct such calculations. All these studies were retrospective and thus provide level III evidence. An extensive body of literature exists reporting single institutional outcomes without controls following FLS implementation, however, those studies were not reviewed here as without a comparator group we found them of limited use in demonstrating the impact of FLS implementation. Further, we excluded studies that did not report data from which we could interpret results based on the intention to treat (ITT) principle. While some of these studies provide interesting data, we believe they provide a misleading representation on the impact FLS programs have on the patient populations they are meant to serve. FLS programs are intended to address a population level care gap and as such should be judged primarily on the impact they have on that care gap. All the quantitative results reviewed here are highly dependent on the level of post-fracture osteoporosis care present before FLS implementation. After all, you cannot improve DXA scanning 7-fold if you are already scanning 20% of eligible patients. Any FLS is unique to the providers, needs, and patients that it serves as well as the healthcare system in which it is situated. There is a certain degree of normal variation in how an FLS is implemented. This likely accounts for some of the variation in findings between studies.
These limitations notwithstanding, the patient care value of the FLS is difficult to dispute. Other authors have shown FLS implementation to be fiscally sound as well. 41,43 -45
Conclusion
Osteoporosis recognition and management after minimum trauma fractures represents a substantial international care gap. Fracture liaison services provide flexible, multidisciplinary models through which institutions can systematically act to address this care gap in accordance with internationally recognized guidelines. This study is a systematic review and meta-analysis evaluating the clinical impact of FLS implementation based on the results of 10 level III studies encompassing 48,045 patients, of which 5 studies encompassing 7,086 were meta-analyzed. The findings reviewed here suggest that fracture liaison services significantly improve the rates of DXA scanning and antiresorptive therapy prescription as well as reductions in the rates of new fractures and death among patients seen following minimum trauma fractures.
Footnotes
Abbreviations
Fracture Liaison Service (FLS), Dual energy X-ray Absorptiometry (DXA), Hazard Ratio (HR), Odds Ratio (OR)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.