
Abstract
Introduction:
Recent literature suggests that surgical fixation of elderly sacral fractures may reduce time to mobilization and ultimately self-sufficiency. However, it is unclear if predictors of success exist in this subpopulation. The objective of this study was to characterize relative change in ambulation and residential living statuses (pre-injury vs. post-surgery) of elderly patients who received surgical fixation of sacral fractures, as well as determine whether or not demographics and injury characteristics influence these findings.
Methods:
Fifty-four elderly patients (≥60 years old) receiving percutaneous screw fixation of sacral fractures were retrospectively reviewed. All fractures were traumatic in nature; insufficiency fractures were excluded. Patient and surgical demographic data, as well as 1-year mortality status, was reported. Primary study endpoints included relative change in patient ambulation and residential living statuses (pre-injury to post-surgery). Statistical analyses were performed to assess relative change in ambulation/living status from pre-injury to post-surgery and to determine if predictors of outcome existed.
Results:
Of the 54 patients who met inclusion criteria, 4 expired prior to discharge, 2 expired post-discharge, and 4 were lost to follow-up. Of those patients discharged, 95.7% regained some form of ambulation at last follow-up (mean: 22.4 ± 18.9 weeks). Of patients living independent pre-injury, 94.9% would eventually return to independent home living. Neither time-to-surgery, concomitant orthopaedic injury, Charlson Comorbidity Index, or injury mechanism were predictors of final ambulation or residential status (p ≥ 0.07). Mortality at 1-year was 11.1%.
Discussion:
Operative fixation supported a high rate of return to pre-injury ambulation and residential living status. However, there did not appear to be measures predictive of final functional status. Further efforts with larger, prospective cohorts are warranted.
Introduction
Sacral fractures in the aging and elderly population are a common and continued challenge. Increased patient comorbidities and declining functional status make successful treatment difficult. While fragility and insufficiency fracture mechanisms are prominent in this injury population, trauma plays a contributory role as well. It is estimated that over half (51.6%) of all sacral fractures (with no associated osteoporosis) occur in patients 65 years or older (years 2002 to 2011; United States). 1
Given the inherent stability of the sacrum within the pelvic ring, conservative therapy, typically consisting of bed rest, analgesia, and physical therapy, has traditionally been considered adequate in treating these patients. Approximately only 2% of elderly sacral fractures (with no associated osteoporosis) receive surgical management, compared to an estimated 18% in the population under 65 years old. 1 However, the evidence remains disconcerting for those patients receiving conservative therapy, as approximately only 40% regain pre-injury ambulation status by 1-year, with a mortality rate of 14.3 to 22.6%. 2,3
Prolonged immobilization of these patients lends to loss of self-sufficiency, increased co-morbidity, and increased cost of care. 2,4,5 Furthermore, risk of progressive lumbosacral instability or even neurologic insult from these fractures can be devastating. 6 -8 While surgical fixation is typically considered a last line treatment given its invasive nature, the ability to reduce time to mobilization and ultimately self-sufficiency is clinically appealing. As a result, the literature has seen an emergence of evidence characterizing the utility of surgical fixation in treating sacral fractures within the aging population. 9 -12 Outcomes suggest that surgical fixation in these patients can afford immediate ambulation (mean distance post-operative Day 1: 114.4 feet), as well as a high rate of return to independent living (73-75%). 10 -12
However, while this evidence has been encouraging and effective in establishing the utility of surgical fixation in the elderly population, especially in comparison to non-operative treatment, it has yet to explore many factors that may influence outcome. 9 -12 It is unclear whether such variables as baseline function (i.e. ambulation status, place of residence), time-to-surgery, concomitant injury, and fracture mechanism (i.e. low- vs. high-energy) effect the quality of outcome in these patients. Accordingly, the objective of this study was to characterize functional outcomes (i.e. return to ambulation and living residence) of elderly patients receiving percutaneous fixation for sacral fractures and to determine what, if any, demographics may be predictive of these outcomes.
Methods
Study Design
A retrospective study of 54 elderly patients (≥60 years) receiving percutaneous screw fixation of sacral fracture(s) between 2010 and 2018 was performed. Institutional Review Board (IRB) approval was obtained prior to study commencement (Cooper University Hospital IRB) and no active informed consent was required. All patient information was used in a de-identified manner. All study patients received surgical treatment at Cooper University Hospital (Level I Trauma Center; Camden, NJ USA). Study inclusion criteria required patients to be of ≥60 years of age and have sustained a U-type, Zone I-III (Denis classification), and/or lateral compression type 2 (LC II) sacral fracture. Fracture types were classified by the senior author (K.G.). An example of a Denis II classification, in a high-energy trauma patient (motor vehicle crash), is captured in Figure 1. Any fracture without an explicit eliciting injury (i.e. stress or insufficiency fracture) was excluded. Pathologic fractures were also excluded. Given that these fractures are chronic in nature, time to diagnosis and/or date of occurrence can be either delayed and/or unknown. Accordingly, these patients did not make appropriate subjects in the current study as time-to-surgery (from date of injury) is a key consideration.

Imaging of an 81-year-old patient who experienced a high-energy trauma (motor vehicle crash), resulting in complete unstable left S1& S2 sacral fractures (Denis 2 classification), left segmental superior-inferior ramus fractures, and a right parasymphyseal superior ramus fracture. Pre- (top) and post-operative (middle) A/P radiographs. Pre-operative CT imaging (bottom).
All patients with injuries were surgically fixed with unilateral ilio-sacral, bilateral ilio-sacral, or trans-sacral cannulated screws, with anterior fixation as deemed surgically necessary. Patients who had experienced a low-energy trauma (resulting from any fall from a standing height or less), with a vertically stable fracture pattern, were first trialed on 3 to 5 days of conservative care with subsequent ambulation testing. Surgery was indicated in the event of failed ambulation. An example of a Denis I classification, in a low-energy trauma patient (fall from standing height) is captured in Figure 2. Following surgery, all low-energy trauma patients were made weight bearing as tolerated (WBAT) upon discharge, while high-energy trauma patients were advanced to WBAT on a case-by-case basis.

Imaging of an 83-year-old patient who experienced a low-energy trauma (fall from standing height), resulting in complete right S1 & S2 sacral fractures (Denis 1 classification), a right high superior pubic ramus fracture, and a left comminuted displaced parasymphyseal pubic ramus fracture. Pre- (top left) and post-operative (top right) A/P radiographs. Pre-operative CT imaging (posterior A/P view - bottom left; anterior A/P view – bottom right).
Patient demographic data was collected, including age (at time of injury), gender, smoking status, comorbid conditions (diabetes mellitus, osteoporosis), concomitant musculoskeletal injury (including type), injury mechanism (high- or low-energy trauma), and sacral fracture pattern. Charlson Comorbidity Index (10-year survival) (%) was determined for each subject. Surgical variables collected included time-to-surgery (TTS) and length-of-stay (LOS). Mortality and time-to-mortality were also collected. Follow-up was not standardized; however, all patients were seen by the same orthopaedic practice (Cooper Bone and Joint Institute; Camden, NJ USA) affiliated with the institution that performed the initial surgery. Mortality status at ≥1-year was determined systematically by first consulting the patients electronic medical record (EMR). Patients mortality status was adequately determined if their EMR indicated an attended appointment (any specialty) and/or hospital admission at ≥1-year post-discharge or their EMR indicated they were deceased <1-year post-discharge. For those patients who did not have any record ≥1-year or were determined deceased >1-year (without interval follow-up/admission ≥1-year) further determination was required. For those patients without any record, the principle investigator (K.G.) attempted contact via telephone. All patient requiring such contact were confirmed to be living. For those patients indicated deceased at >1-year without interval history or date of passing, their date of passing was determined via obituary records.
Primary study endpoints included the relative change in patient ambulation status and patient residential living status (place of residence status) from pre-injury to post-surgery. Patient ambulation and living status were recorded at baseline (pre-injury) and at all subsequent follow-up visits. Time to earliest ambulation was also determined, representing the elapsed time (weeks) to earliest full-time weight-bearing ambulation (any form; established on in-office visit only). Ambulation status was defined as either ambulatory (independent, cane, or walker) or non-ambulatory (wheelchair or bedridden). Ambulatory patients were further broken down into those who were ambulating independently without any assistance and those who were ambulatory only with an assisted device (cane, walker). Living status was defined as either independent (home) or assisted (nursing home, assisted living facility, rehabilitation facility). All living statuses were determined either from patient reporting or post-operative care facility transcripts. Of note, change in ambulation status and associated duration/time-point (post-discharge) was acknowledged only when established formally in-office. For example, if a patient anecdotally stated they had resumed unassisted walking at 6 weeks but did not report to office follow-up until 8 weeks, 8 weeks was considered the time-point at which change had occurred. This ensured that change in status was established by physician evaluation. Furthermore, a change in ambulation status was only acknowledged when the advance in status was performed full-time throughout all aspects of daily life (i.e. not just during physical therapy or rehabilitation sessions).
Of the 54 patients who met initial inclusion criteria, 4 died prior to discharge, 2 died after discharge, and 4 were lost to orthopaedic follow-up after discharge (mortality status obtained). The 4 patients lost to follow-up were included in the calculation of 1-year mortality rate but excluded from all other analyses. The authors rationale for the inclusion of these patients in the mortality rate was due to the possibility that mortality was the cause of follow-up loss. Exclusion of these patients would potentially omit a mortality case. Also, of note, the 2 patients who expired post-discharge were included in all follow-up analyses as their living and ambulation status was determined at the time of their passing. Hence, demographical descriptive statistics included all patients who expired pre-discharge or had follow-up post-discharge (n = 50), while all follow-up analyses included only those patients who had at least 1 known functional follow-up status post-discharge (n = 46). Of those 46 patients with at least 1 known post-discharge functional status, 44 patients possessed clearly delineated pre-injury and post-surgery ambulation statuses and 42 patients possessed clearly delineated pre-injury and post-surgery living statuses.
Patient Demographics and Follow-Up Outcomes.
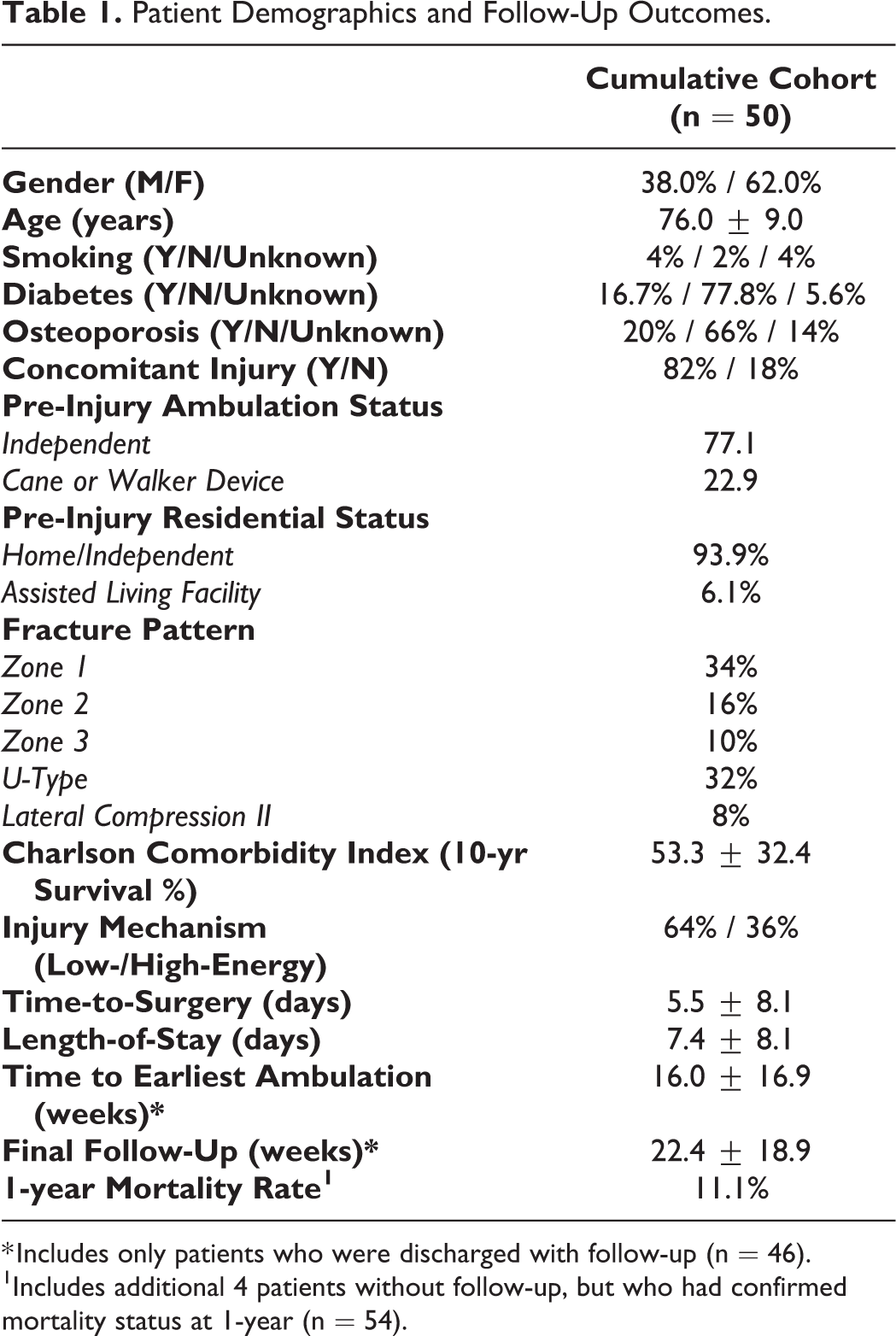
* Includes only patients who were discharged with follow-up (n = 46).
1Includes additional 4 patients without follow-up, but who had confirmed mortality status at 1-year (n = 54).
Statistical Methods
Demographic data, when applicable, was reported as a mean value ± standard deviation or as a percentage. A Fisher’s exact probability test was performed to assess change in ambulation status and living status pre-injury/post-surgery. Additionally, a Wald chi-squared test was performed to determine whether time-to-surgery, concomitant injury, Charlson Comorbidity Index (CCI), and injury mechanism (i.e. low- vs. high-energy) were predictive of final ambulation and living statuses. Statistical differences were considered significant for values of p<0.05. Statistical software used was SAS v9.4 (SAS Institute, Cary, NC).
Results
General Data
Patient demographics of the 50 patients who met study inclusion are summarized in Table 1. Patients demographics, stratified by injury mechanism (low- vs. high-energy), are summarized in Table 2.
Patient Demographics and Follow-Up Outcomes Stratified by Injury Mechanism.
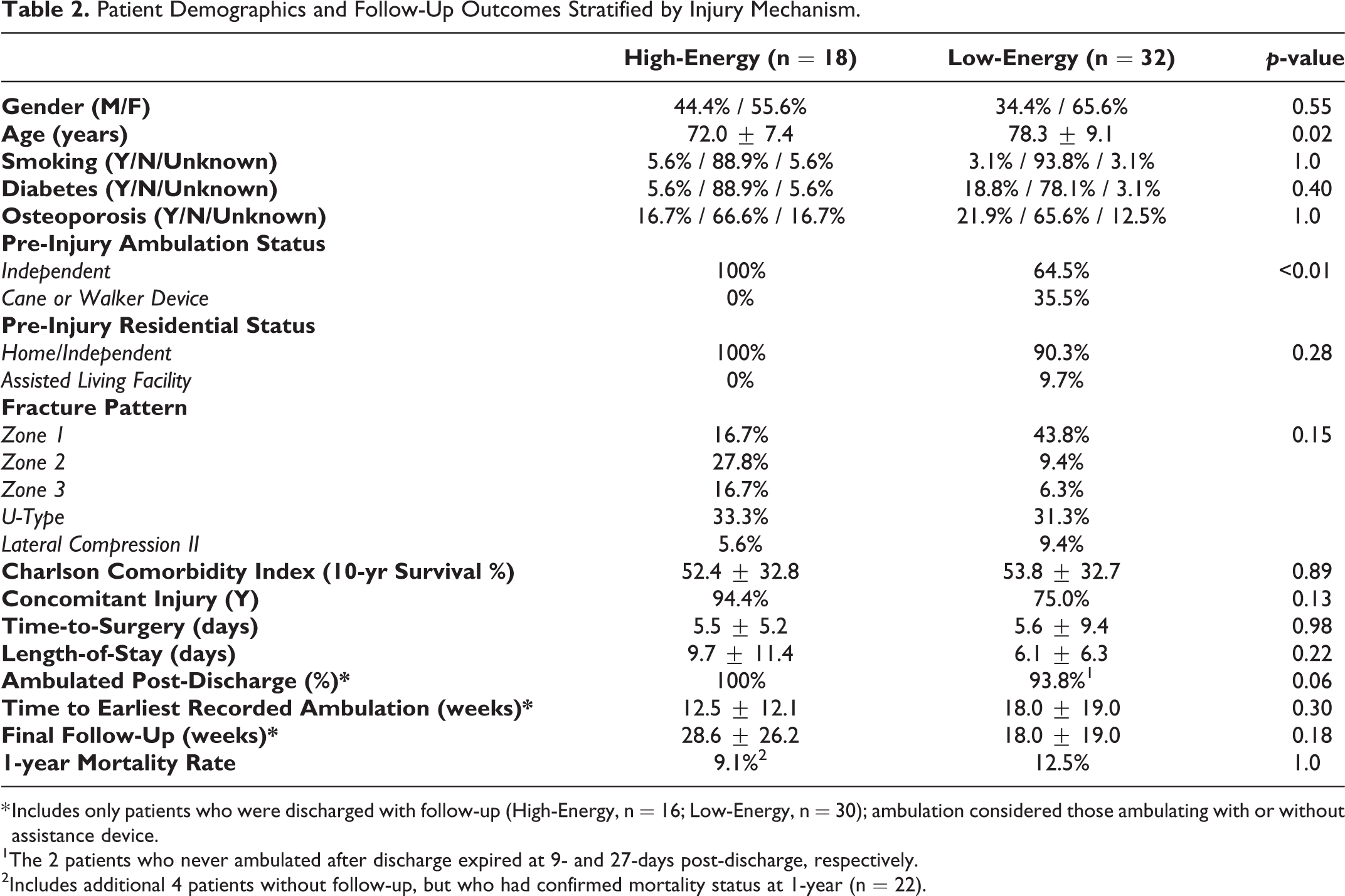
* Includes only patients who were discharged with follow-up (High-Energy, n = 16; Low-Energy, n = 30); ambulation considered those ambulating with or without assistance device.
1 The 2 patients who never ambulated after discharge expired at 9- and 27-days post-discharge, respectively.
2 Includes additional 4 patients without follow-up, but who had confirmed mortality status at 1-year (n = 22).
Hospital Course
Mean TTS and LOS for the collective cohort were 5.5 ± 8.1 days and 7.4 ± 8.1 days, respectively. TTS was not a predictor of LOS (p = 0.66). TTS and LOS were not significantly different between the low- and high-energy trauma cohorts (p ≥ 0.22) (Table 2). CCI was not a significant predictor of LOS (p = 0.19).
Ambulation
Of those patients receiving hospital discharge, 95.7% (44/46) would regain ambulation (i.e. independent or with cane or walker device). The 2 patients who did not resume ambulation expired at 9- and 27-days post-discharge. With respect to relative change in ambulation, 44 patients had clearly established pre-injury and post-discharge statuses (Table 3). Thirty-four of these patients ambulated independently pre-injury, while 10 patients utilized a cane or walker device. Of the 34 patients ambulating independently pre-injury, 91.2% (31/34) would regain independent ambulation by last follow-up. The remaining 3 patients would regain ambulation with a cane or walker device. Of the 10 patients who utilized a cane or walker device pre-injury, all (100%) would regain some form of ambulation post-discharge, with 3 patients eventually advancing to independent ambulation. The authors recognize that those patients that advanced from non-independent ambulation pre-injury to independent ambulation post-discharge (last follow-up) appear as an anomaly. In all 3 cases, adoption of an assistance device had been recent, secondary to unrelated injury and/or concern for fall. All patients actively participated in physical therapy following discharge.
Change in Ambulation, Pre-Injury to Post-Surgery, in Collective Cohort.

Those patients ambulating independently pre-injury were significantly more likely to independently ambulate post-discharge, as compared to those who utilized a cane or walker device pre-injury (p < 0.01). With regard to injury mechanism, there was no significant difference in final ambulation post-surgery when stratified by low- vs high-energy trauma (p = 0.07). CCI was not a significant predictor of pre-injury or post-surgery ambulation status (p ≥ 0.23). Neither TTS or presence of concomitant orthopaedic injuries were a predictor of final ambulation status (p ≥ 0.46).
Residential Living Status
Forty-two (n = 42) patients had clearly established pre-injury and post-discharge residential/home living statuses (Table 4). Thirty-nine (92.9%) patients were living independently at home prior to injury, while 3 (7.1%) patients were living in a facility with assistance. Of the 39 patients living at home pre-injury, 37 (94.9%) would eventually return to their home residence, while 2 (5.1%) were still at an assisted living facility at last follow-up. Of those patients living in an assisted facility pre-injury (n = 3), one (n = 1) would return to independent living by last follow-up (33.3%). Of note, the authors do recognize that the advancement from assisted facility (pre-injury) to independent living (by last follow-up) appears counterintuitive. However, this patient had recently been admitted to in-patient rehabilitation for pelvic fractures (no radiographic evidence of sacral fracture on admission), after which a new diagnosis of a U-type sacral fracture was made. Per current study protocol, the patients baseline pre-injury status was determined to be in-patient/assisted. Those patients living independently prior to injury had a greater likelihood of living independently following discharge than those who were in assisted living pre-injury (p = 0.02). (Table 4). All high-energy trauma patients (100%) would eventually return to an independent home living environment by last follow-up, in comparison to 85.2% in the low-energy cohort, however, this difference was not significant (p = 0.27). CCI was not a significant predictor of pre-injury or post-surgery living status (p ≥ 0.79). Neither TTS (p = 0.42) or presence of concomitant orthopaedic injuries (p = 0.57) were significant predictors of final living status.
Change in Residential Living Status, Pre-Injury to Post-Surgery, in Collective Cohort.

Mortality
Overall, mortality at 1-year was 11.1% in the collective cohort, while low- and high-energy trauma mortality rates were 12.5% and 9.1%, respectively (p = 1.0) (Table 1, 2). Four patients expired prior to discharge, while 2 patients expired at 9- and 27-days post-discharge. A summary of the diseased patients is included in Table 5.
Summary of Deceased Patients.

Discussion
Percutaneous fixation of sacral fractures in the elderly population provides a minimally invasive means to achieving immediate mechanical stability of the sacrum. While considered a more invasive up-front treatment modality in comparison to conservative measures, the ability to weight-bear sooner may have profound effects with respect to return to ambulation and residential living status. To date, the evidence suggests that sacral fixation in these patients is a safe procedure, with good survivorship, and advantageous pain/functional trends at discharge, however, it is not well understood whether these patients are regaining pre-injury functional status. Furthermore, it is not well understood as to what may be predicative of functional success in these patients. The current study sought to answer both questions.
In the current study, 95.7% of patients with known pre-injury ambulation status would again full-time ambulate in some form. The only 2 patients who did not resume ambulation expired at 9- and 27-days post-discharge. This trend is similar to Walker et al, which found that 100% of operatively fixed elderly sacral fracture patients (U-type and LC1 fractures types) could ambulate discharge, as demonstrated on measured walking test (mean distance: 95ft). 12 In comparison to non-operative treated patients, these outcomes were significantly improved (72% ambulating, mean distance: 35ft; p ≤ 0.03). However, a key differentiator of Walker et al is that some patients (37.5%) had regained ambulatory status prior to surgery, compared to none (0%) in the current study. Additionally, it is unknown as to whether ambulation on discharge was suggestive of full-time ambulation once in their daily environment.
Mears et al, characterizing conservative care for displaced and non-displaced sacral fractures in elderly patients (low-energy falls) found that 39.1% of patients who ambulated without assistance pre-injury had regained the same status by 1-year follow-up. 3 Similarly, Taillandier et al, evaluating conservative care of sacral insufficiency fractures in the elderly, reported that only 39.3% of patients returned to the same level of self-sufficiency by 1-year. 2 In contrast, in the current study, full-time ambulation was achieved by 95.7% of patients by last follow-up of 22.4 ± 18.9 weeks. Furthermore, 91.2% of patients who ambulated independently pre-injury had regained that same status at last follow-up. Given that the current study only reported change in status at the time of formal office evaluation, it is possible these timelines were shorter than reported.
While the current study did not assess any quality-of-life outcomes secondary to surgical intervention and subsequent return to ambulation, the implication of such is profound. Hirvensalo et al found that independently living elderly patients (65- to 84-years old; n = 1109) had a relative risk of death that was 2 times (or more) greater in individuals with impaired mobility than those with intact mobility. 13 Similarly, Campbell et al found that decline in functional ability directly correlated with increased mortality of elderly patients. 14 One-year mortality in the current study was 11.1%. This appears consistent with other reported mortality rates in operatively treated elderly sacral fracture populations (≥10%). 10,12 Reported mortality rates in non-operative treated elderly sacral fracture patients (insufficiency and fragility) range from 14.3 to 22.6% at 1- year. 2,3
Regarding injury mechanism (low- vs high-energy), no significant differences were found between groups regarding final ambulation status (p ≥ 0.07). All but 1 high-energy trauma patient returned to independent ambulation by last follow-up, while all but 2 returned to independent home living by last follow-up. This trend is of note given that these patients traditionally have a higher rate of concomitant orthopaedic injury, with 94.4% of high-energy patients possessing such injuries in the current study (vs. 75.0% in low-energy patients). While the decision to perform surgery in these patients is typically dictated by their severity, which included risk of fracture displacement and/or neurovascular compromise in the current study, these trends suggest strong outcomes in these patients. While high-energy elderly sacral fractures are more likely to be treated surgically in comparison to low-energy fractures, given that reduction is often necessary, these outcomes suggest similar success across both demographics. 15
With respect to living or residential status, 94.9% of patients in the current study who had been living independently pre-injury returned to their same residential living status by last follow-up. The relative change in residential living status from pre-injury to post-surgery was statistically significant, such that those living independently prior to injury had a greater likelihood of living independently following surgery than those who were in assisted living facility pre-injury (p = 0.02). This compares favorably to Eckardt et al, who similarly assessed fixation in elderly fragility fractures of the sacrum, finding that only 73% of patients were living at home by 1-year follow-up. 10
Mears et al, assessing conservative care for sacral fractures in elderly patients, found that 69.8% of patients who were living independently prior to injury had returned to the same status by 1-year follow-up. 3 In contrast, the current study found that 94.9% of independent living patients would eventually return to the same living status by last follow-up (22.4 ± 18.9 weeks). The implication of this on patient mortality and quality-of-life is not well understood in the literature. However, the ability to avoid long-term rehabilitation at an assisted-living facility presents with substantial economic upside. In 2003, Braithwaite et al estimated that 44% of lifetime costs for hip fractures ($81,300; 1997 USD) were from nursing facility expenses alone. 16 Similarly, Gu et al, also assessing associated costs of hip fractures in the elderly, found that those receiving surgical treatment saved a lifetime mean of $83,118-$87,188 in associated nursing-home costs. 17 These cost-savings values cannot be directly extrapolated to sacral fractures given differences in fracture type/extent, diagnosis interval, time-to-surgery, etc. however, they indicate a clear cost burden associated with early or pro-longed facility care in the elderly fracture population.
Furthermore, when considering the potential cost burden of sacral fractures in the elderly it is also crucial to consider the role of cost incurred during hospitalization. In the current study, mean LOS was 7.4 ± 8.1 days for the collective cohort. When stratified by low- and high-energy trauma mean LOS was 6.1 ± 6.3 and 9.7 ± 11.4 days, respectively. TTS in the low-energy group (6.2 ± 9.9 days) was near equal to the that of LOS, suggesting that patient’s hospitalization duration was driven primarily by pre-operative course rather than post-operative course. This is consistent with the treatment protocol of conservative care (3 to 5 days) with failed ambulation testing prior to surgical intervention in the low-energy cohort. Hoch et al reported a similar TTS of 6.4 ± 4.1 days in surgically treated elderly patients with lateral compression fractures. 9 In the same study, mean LOS for those surgically treated and those receiving conservative care was 9.2 ± 6.2 and 18.1 ± 10.0 days, respectively. 9 Mears et al reported a mean LOS ranging of 5.7 to 9.3 days for conservatively treated elderly sacral fracture patients. 3 Walker et al has reported the lowest mean LOS (3.6 days) in this surgically fixed subpopulation. 12 Patients treated non-surgically in the same study had a mean LOS of 4.2 days. 12 Lastly, in consideration of trends in the general population (both elderly and non-elderly), Bydon et al demonstrated that from years 2002 to 2014 the mean LOS for surgical fixed sacral fractures decreased from 11.9 to 9.6 days. 1 Collectively, these trends suggest that the LOS in the current study is consistent with other surgically treated sacral fracture cohorts, regardless of age. However, as evident by the higher mean LOS of high-energy trauma patients in the current study (vs. low energy), concomitant orthopaedic injury remains a likely confounding element in any sacral fracture cohort.
In addition to characterizing ambulation and living status outcomes, a second primary objective of the current study was to understand whether there are predictive measures of functional success in these patients. TTS, concomitant orthopaedic injury, and injury mechanism were all considered in the current study. It was found that none of these parameters were a significant predictor of final ambulation or living status (p ≥ 0.07). Additionally, TTS was not a significant predictor of LOS in the collective group (p = 0.66). However, use of a conservative care trial in low-energy patients is a likely cofounder in this relationship. Of note, high-energy trauma patients did have a lower mean TTS. The lower TTS may be explained by the more urgent need to stabilize these patients and, conversely, the need to attempt conservative treatment in low-energy patients. As noted by Ruatti et al, early biomechanical restoration of the sacrum diminishes the progression of soft-tissue damage. 18 Furthermore, early surgical intervention can prevent delayed neurological injury due to callus and hematoma formation, as well as possible bone fragment migration. 19
As observed in the geriatric hip-fracture population, time-to-surgery may be a significant predictor of complication and mortality and should be explored further within the sacral fracture population. 20,21 Pulley et al has foreshadowed this phenomena in the elderly sacral fracture population, showing that acute surgical intervention in these patients produces greater mean decrease in pain from pre- to post-surgery as compared to delayed intervention (p = 0.15). 11 However, the difference in mean TTS for these 2 cohorts was drastic (5 vs. 83 days). 11 Future efforts with larger cohorts and incremental decrease in TTS may be beneficial in better delineating the role of surgical timeliness in this sacral fracture subpopulation.
Limitations
This study was performed retrospectively, possessing an inherent patient selection bias. Study sample size is also a potential limitation. The authors goal was to be consistent with current reports in the literature assessing operative fixation in the geriatric population (range: 16 to 50 patients). 9 -12 The authors realize that these historical reports do not justify or dictate what is considered adequate, however, the current study appears to not regress within the context of established reports. Lack of a non-operative control group is also a primary limitation of the current study. While predictive analyses allowed for quantitative insight into the singular cohort, a control cohort assessing the same predictive measures would be further telling. However, the authors do believe that the novelty of the current study is its consideration and analyses regarding predictive metrics. No study to date has given this consideration. Regardless of current study outcomes, the authors intent is that future studies will continue to propagate this consideration and explore the implications of patient and surgical demographics on outcome success. Future analysis of a non-operative therapeutic group would be a valuable comparison. The short duration of follow-up could also be considered a potential limitation. The authors do recognize that follow-up out to >12-months is not uncommon in this population in the literature. 2,3,9,10 However, given the high functional success achieved (>90% return to pre-injury living and ambulation status) by last follow-up in the current study (22.4 ± 18.9 weeks), further follow-up was often not pursued by patients. Regression beyond last follow-up is certainly possible, however, no patient exhibited any final ambulation/living status lesser than that of a previous post-discharge status. Additional limitations included heterogenous fracture pattern, variation of concomitant injuries and comorbid conditions, non-standardized time-to-surgery, and variable injury mechanism. However, predictive analyses allowed for advantageous use of these varied metrics. Additionally, comparative analyses of injury mechanism cohorts showed no statistical differences in functional outcome.
Conclusion
Operative fixation of traumatic sacral fractures in elderly patients supports a high rate-of-return to pre-injury ambulation and residential living status. These findings are consistent between low- and high-energy sacral fracture populations. Further analysis is required to understand the economic impact of these trends, as well as to optimize the treatment algorithm, which includes the role of time-to-surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
The authors and their associated institutions received no sources of funding or compensation regarding participation or contribution to any aspects of this work. No commercial entities are discussed within this work. No discussion of off-label device usage is discussed in this work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.