
Abstract
Introduction:
Opioid-related adverse drug events (ORADEs) are an increasingly recognized complication associated with the common prescription of opioids after orthopedic surgery. In this study, we attempted to understand how potential ORADEs following hip replacement surgery in older patients affected hospital length of stay, hospital revenue, and their association with specific risk factors and clinically relevant diseases occurring during hospitalization.
Methods:
We conducted a retrospective study using the Centers for Medicare and Medicaid Services Administrative Database to analyze Medicare discharges after hip replacement surgery to identify potential ORADEs. The impact of potential ORADEs on mean hospital length of stay (LOS) and hospital revenue was analyzed.
Results:
The potential ORADE rate in patients who underwent hip replacement surgery was 8.6%. The mean LOS for discharges with a potential ORADE was 1.41 days longer than that for discharges without an ORADE. The mean hospital revenue per day with a potential ORADE was US$1708 less than without an ORADE. Potential ORADEs were also found to be strongly associated with poor patient outcomes such as pneumonia, septicemia, and shock.
Discussion:
Potential ORADEs in hip replacement surgery in older patients are associated with longer hospitalizations, decreased hospital revenue per day, certain patient risk factors, and clinically relevant diseases occurring during hospitalizations. Our finding of an association between potential ORADEs and decreased hospital revenue per day may be attributed to the management of these adverse events, as a patient may need to undergo additional testing, may need additional treatment regimens, and may need a higher level of care.
Conclusion:
By reducing the use of opioids and employing a multimodal analgesic approach, we may improve patient care, decrease hospital lengths of stay, and increase hospital revenue
Introduction
There are over 73 million surgical procedures performed in the United States each year, with 75% to 80% of patients experiencing postoperative pain. 1 -4 Opioid-based analgesia continues to be the most commonly used treatment in postoperative pain management, with more than 95% of surgical patients receiving opioids during their hospitalization. 1 -9 Although opioids are extremely effective analgesics, they can potentially predispose the patient to numerous adverse side effects. 1,2,5,7 The potential benefit of opioid use must be weighed against the risk of opioid-related adverse drug events (ORADEs) in the perioperative period. 7,8
Opioid-related adverse drug events are undesired effects that can occur throughout various organ systems in the body. 1,2,5,6 Specifically, these effects include nausea, vomiting, constipation, confusion, decreased psychomotor coordination, and respiratory depression. Opioid-related adverse drug events are common and have been documented in up to 20% of patients treated with opioids. 1,3,4,9 It has been shown in multiple studies that treatment of ORADEs lead to increased hospital length of stay (LOS), increased hospital readmission rates, and increased hospital costs. 1,3 The negative impact of ORADEs on patient care and health-care costs has recently led to studies examining ORADEs within specific classes of surgeries.
Hip replacement surgery is one of the most common surgical procedures performed in the United States, especially in the older population. 10 It is estimated more than 400 000 total hip replacements are done in the United States each year. 1 With the “baby boomer” generation continuing to climb in age, the increased rates of diagnosing and treating advanced arthritis, and the demand for interventions to improve quality of life, the incidence of hip replacement surgeries is expected to rise in the coming decades. 11 While hip replacement surgery is one of the most successful surgeries for restoring mobility and quality of life, it can result in significant postoperative pain. With opioids still being the primary method of pain control in the perioperative setting, there is significant risk for ORADEs. According to Kessler et al, surgical patients aged 65 years and older are at an increased risk for developing ORADEs, as well as patients who are male, obese, used opioids preoperatively, and have a higher score on Charlson Comorbidity Index. 2 Due to age-related physiologic changes, high numbers of present comorbidities, and high rate of polypharmacy seen in the elderly population, the risk of developing these adverse events is significant. 12 Little information is currently available regarding how ORADEs following hip replacement surgery affect hospital LOS and hospital revenue or the association between ORADEs with patient risk factors and clinically relevant diseases occurring during a patient’s hospitalization. We hypothesized that potential ORADEs are associated with increased hospital LOS, decreased hospital revenue, and specific risk factors and clinically relevant diseases occurring during a patient’s hospitalization. Therefore, the aim of the study is to investigate the impact of ORADEs on patient outcome and hospital financial metrics. In understanding the clinical and economic implications of potential ORADEs in hip replacement surgery, we hope to further optimize the clinical and administrative approach to postoperative pain management in an attempt to improve patient care and minimize hospital costs in this older population.
Methods
Study Design
In this retrospective study, we analyzed data from the Medicare Limited Data Sets (LDS) from the Centers for Medicare and Medicaid Services (CMS). The LDS is an administrative claims database containing data from all the hospitals in the United States that provided care to patients with Medicare. This represents approximately 35% of all inpatient hospital discharges in the United States. 13 Hip surgeries were identified by the International Classification of Diseases, 10th Revision (ICD-10) code and were split by Diagnosis-Related Group (DRG) code to account for unmeasured confounders related to patient illness severity. These groups were used to analyze the effect of potential ORADEs on mean hospital LOS and hospital revenue in patients undergoing hip replacement surgery. Within these groups, associations between potential ORADEs and specific patient risk factors and clinically relevant diseases were also analyzed. Since LDS data do not contain specific direct identifiers as defined in the Health Insurance Portability and Accountability Act Privacy Rule, this study was exempted by the institutional review board.
Study Population
The study population included all patients with Medicare discharged between April 2016 and March 2017 who underwent hip replacement surgery. Patients were selected by ICD-10 procedure codes “OSR9” and “OSRB,” which identified all hip replacement procedures of the right and left hip, respectively (Figure 1). In total, 170 042 patients were included in this study.
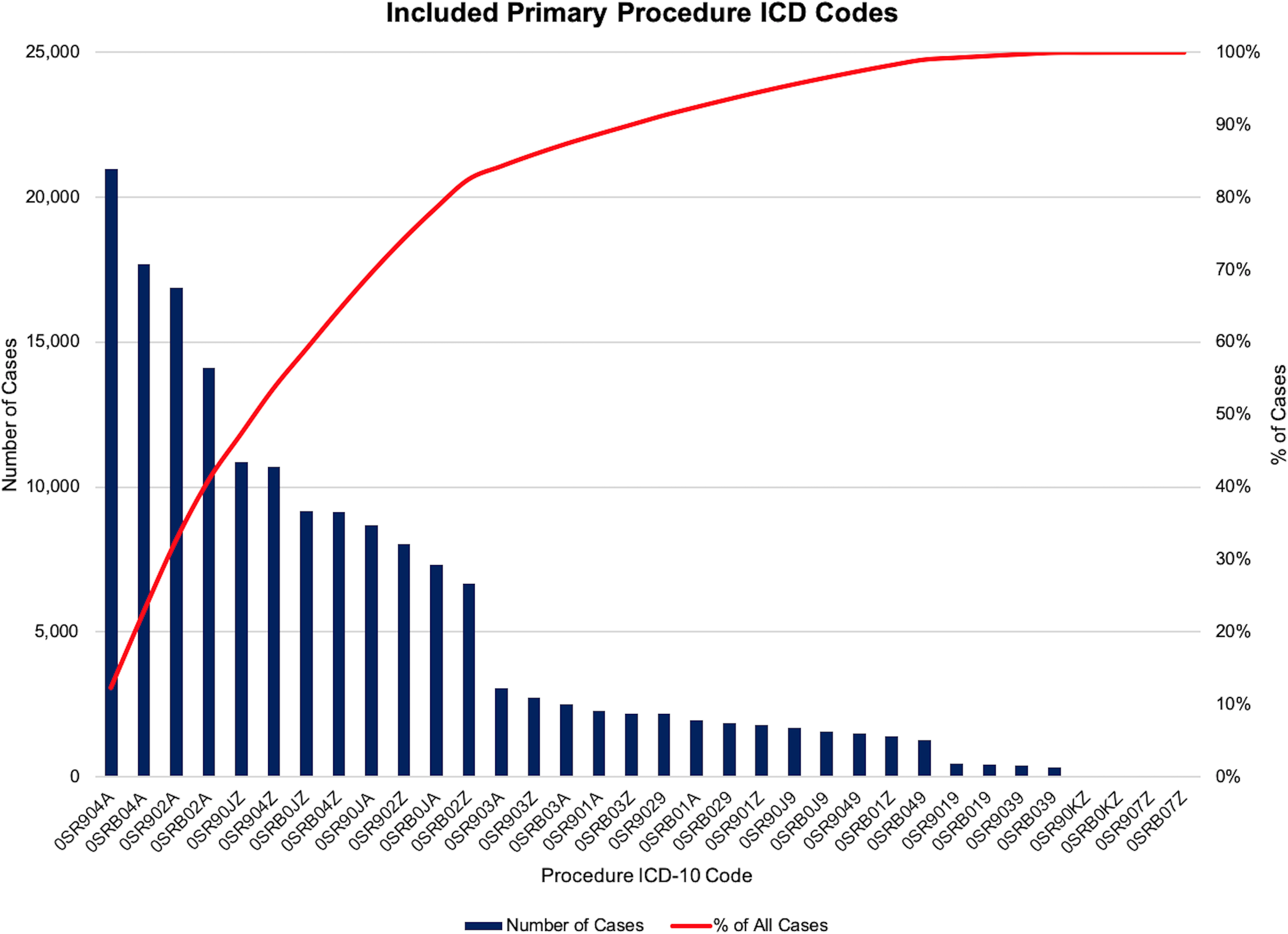
Patients were selected by International Classification of Diseases, 10th Revision (ICD-10) procedure codes OSR9 and OSRB, which identified all hip replacement procedures of the right and left hip, respectively. Patients were selected by ICD-10 procedure codes OSR9 and OSRB, which identified all hip replacement procedures of the right and left hip, respectively.
The patient population contained a mix of indications, as the cases were identified for inclusion based on the ICD-10 procedure codes. Therefore, both elective hip surgery and surgery performed for a fracture were included in the analysis. Our review of the postoperative ICD-10 diagnoses indicates that 87% of the cases (n = 147 914 cases) were for primary osteoarthritis of the hip. Femoral neck and intracapsular fractures were the next most common indication for surgery, representing 4.2% of the cases. The top 20 postoperative diagnoses are listed in Supplementary Table 1.
Two DRG codes were selected for analysis: DRG 469—major joint replacement or reattachment of lower extremity with MCC (defined as major complications/comorbid conditions) and DRG 470—major joint replacement or reattachment of lower extremity without MCC. Examples of MCC include, among others, acute congestive heart failure, endocarditis or myocarditis, acute myocardial infarction, pneumonia, acute respiratory failure, end-stage renal disease, diabetes with ketoacidosis, and sepsis.
Measures
The data collected from the LDS were organized into each of the 2 DRGs. Within each DRG group, data were organized by total discharges, total CMS payments, potential ORADE rate, mean hospital LOS (total, with potential ORADEs, and without potential ORADEs), and mean hospital revenue per day (total, with potential ORADEs, and without potential ORADEs). With these data, the differences in mean hospital LOS and mean hospital revenue per day with and without potential ORADEs were calculated.
Hospital LOS was defined as the total number of days from admission to discharge. Hospital revenue was defined as the CMS reimbursement payment obtained from the LDS. The hospital revenue per day for each DRG was calculated by totaling the Medicare payments for each DRG and dividing by the total hospitalization days within each DRG group.
Potential ORADEs were determined by measuring ICD-10 diagnosis codes that were flagged as not present on admission and those that are associated with ORADEs using a previously validated methodology designed to maximize sensitivity in detection of ORADEs. 8,9,14 The included ICD codes are listed in Table 1.
ICD-10 Codes and Brief Description of the Corresponding Condition.

Abbreviations: GU sys, genitourinary system; ICD-10, International Classification of Diseases, 10th Revision; ORADEs, opioid-related adverse drug events.
Further analysis was conducted to understand the association of potential ORADEs with specific patient risk factors and clinically relevant diseases occurring during a patient’s hospitalization. Using the Agency of Healthcare Research and Quality (AHRQ) Clinical Classification Software (CCS), ICD codes were categorized into groups more suitable for statistical analysis rather than individual ICD-10-Clinical Modification/Procedural Classification System codes. From these groups, CCS categories were selected based on their clinical relevance and statistical significance as related to potential ORADEs within the selected DRG groups in this study.
Statistical Analysis
The CMS payments were expressed in US dollars as the total sum of all revenue from hospital discharges within each DRG. The LOS was expressed as days and is the mean of all hospital discharges within each DRG. A multivariable regression analysis was utilized to determine the odds ratio (OR) of a potential ORADE for each specific CCS category. A P value of <.05 was considered statistically significant for all analyses except for the multivariable regression analysis. To account for making multiple comparisons in the multivariable regression analysis, the Bonferroni adjusted P value of .0019 was considered statistically significant. These analyses were performed using R statistical computing software, v3.2.3 (R Project, Vienna, Austria). In this multivariable analysis, the reference CCS categories were “female” and “age <65.”
Results
Both Tables 2 and 3 summarize the impact of potential ORADEs on hospital revenue and LOS in hip replacement surgery, respectively. The mean hospital revenue per day in discharges with a potential ORADE was US$1708 less than the revenue in discharges without a potential ORADE (US$4753 with a potential ORADE vs US$6461 without a potential ORADE; P < .001). The overall potential ORADE rate in the 2 DRG groups was 8.6% (14 624 out of 170 042 records analyzed). The mean hospital LOS for discharges with a potential ORADE was 1.41 days longer than those without a potential ORADE (3.81 days with a potential ORADE vs 2.40 days without a potential ORADE; P < .001). The number of total discharges with the DRG code 469 (with MCC, 5909 total discharges or 3.5%) was much lower than that for DRG code 470 (without MCC, 164 133 total discharges or 96.5%).
The Impact of Potential ORADEs on Hospital Revenue in Hip Replacement Surgery.

Abbreviations: CMS, Centers for Medicare and Medicaid Services; DRG, Diagnosis-Related Group; ORADEs, opioid-related adverse drug events; MCC, major complications or comorbidities.
The Impact of Potential ORADEs on Length of Stay in Hip Replacement Surgery.

Abbreviations: DRG, Diagnosis-Related Group; LOS, length of stay; ORADEs, opioid-related adverse drug events; MCC, major complications or comorbidities; SD, standard deviation.
The potential ORADE rate for DRG 469 is higher at 41.2% compared to DRG 470 at 7.4%. Diagnosis-Related Group 469 also demonstrates the largest difference in mean hospital LOS for discharges with a potential ORADE at 1.33 days greater than those without an ORADE (P < .001) compared to DRG 470 which has a mean hospital LOS for discharges with a potential ORADE at 0.91 days greater than those without a potential ORADE (P < .001). The mean hospital revenue per day in discharges with a potential ORADE in DRG 469 was US$650 less than the revenue without an ORADE (P < .001). In DRG 470, the mean hospital revenue per day in discharges with a potential ORADE was US$1608 less than the revenue without an ORADE (P < .001).
The multivariable analysis of potential ORADEs with AHRQ CCS categories is listed alphabetically in Table 4. As can be seen in this table, the clinically relevant diseases most strongly associated with potential ORADEs were pneumonia (OR: 5.13; 95% confidence interval [CI]: 4.36-6.05), shock (OR: 4.37; 95% CI: 3.31-5.78), septicemia (OR: 3.63; 95% CI: 2.7-4.89), acute myocardial infarction (OR: 2.95; 95% CI: 2.33-3.73), and gastrointestinal hemorrhage (OR: 2.68; 95% CI: 2.01-3.57). Older age was also associated with potential ORADEs, with patients greater than age 84 having the highest association (OR: 2.1; 95% CI: 1.93-2.29). Patients aged 80 to 84 were the next highest (OR: 1.87; 95% CI: 1.73-2.03), followed by patients aged 75 to 79 (OR: 1.54; 95% CI: 1.43-1.65), patients aged 70 to 74 (OR: 1.37; 95% CI: 1.27-1.47), and lastly patients aged 65 to 69 (OR: 1.16; 95% CI: 1.08-1.25).
Multivariable Association of Potential ORADEs With Risk Factors and Medical Conditions Based on the Clinical Classification Software (CCS) Disease Categories.
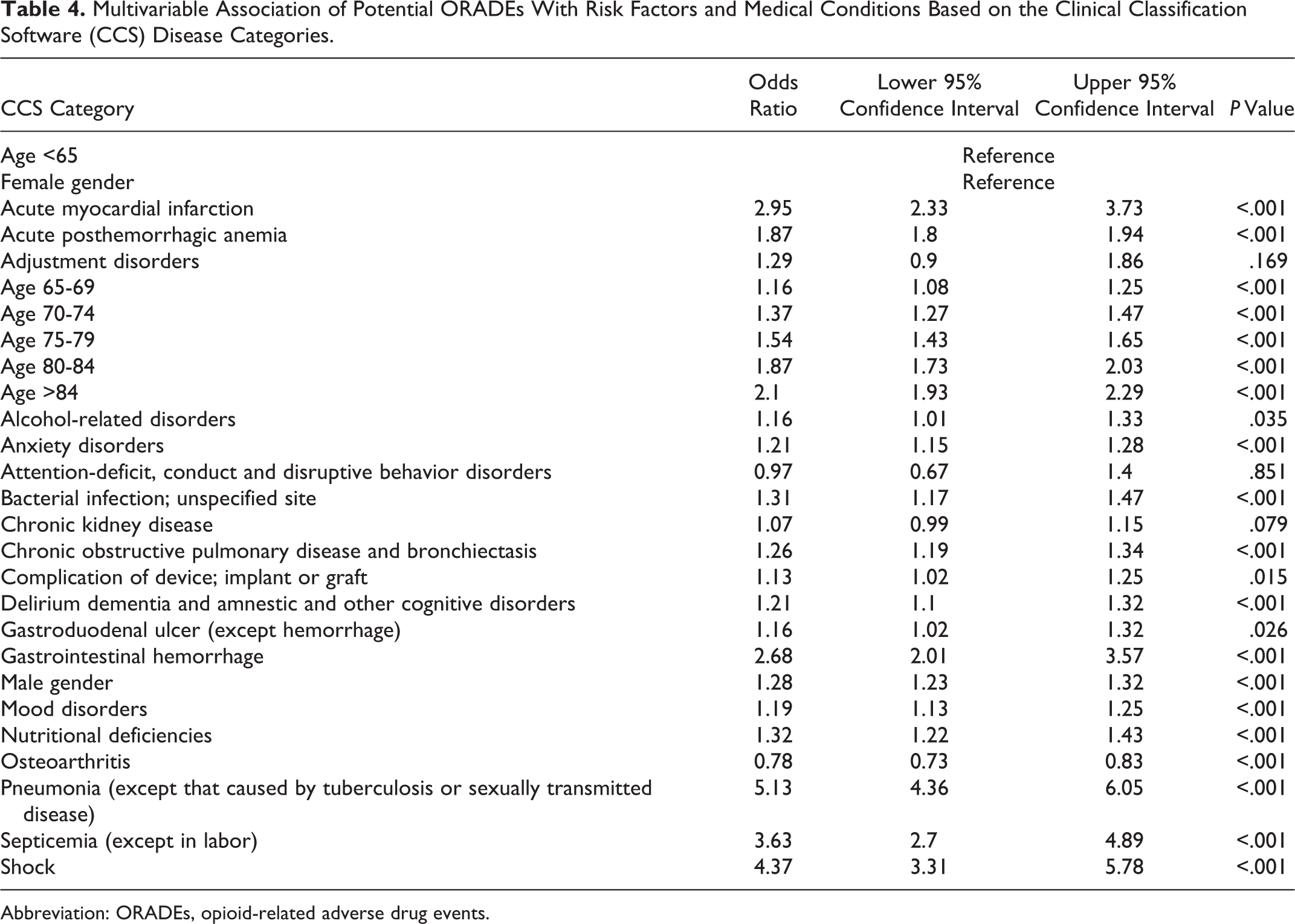
Abbreviation: ORADEs, opioid-related adverse drug events.
Discussion
In our study, we analyzed the effect of potential ORADEs on patients undergoing hip replacement surgery and found that 8.6% of all patients experienced an ORADE, including both major and minor events thought to be possibly related to opioid use. The potential ORADE rate for DRG 469 was higher at 41.2% compared to DRG 470 at 7.4%. Patients with ORADEs had a mean hospital LOS of 1.41 days greater than those without and ORADE and a decreased hospital revenue of US$1,708 per day. Opioid-related adverse drug events were also found to be most strongly associated with poor postoperative outcomes such as pneumonia, shock, septicemia, gastrointestinal hemorrhage, and acute myocardial infarction.
Our finding of increased hospital LOS in patients with potential ORADEs is mostly consistent with prior studies. Kessler et al analyzed 37 031 adult patients who underwent common surgical procedures. 2 Within this population, 98.6% of patients received opioids, and of those patients, 13.6% experienced an ORADE. Patients with an ORADE had a 55% increased hospital LOS. Recently, Urman et al analyzed 13 389 adult surgical patients who were opioid-free at admission and found that 91% of patients received opioids. 3 Of those patients, 9.1% developed a potential ORADE, and subsequently, those patients had an increased hospital LOS of 55%. We hypothesized that the association between potential ORADEs and increased hospital LOS is likely a result of the additional time needed to treat these adverse events. Opioids are associated with a wide range of adverse effects. These adverse effects and potential related consequences such as falls, aspiration pneumonia, and acute respiratory failure all led to prolonged hospitalizations. 15
Our finding of an association between potential ORADEs and decreased hospital revenue per day is likely also attributed to the management of these adverse events. Depending on the type and severity of ORADE present, a patient may need to undergo additional testing, may need additional treatment regimens, and may need to be transferred to a higher level of care. 16 This additional management could ultimately lead to increased hospital costs without a proportional increased reimbursement from Medicare.
As illustrated in Table 4, the CCS categories most strongly associated with potential ORADEs are pneumonia, shock, septicemia, gastrointestinal hemorrhage, and acute myocardial infarction. Pneumonia is likely associated with ORADEs because opioids have the ability to cause respiratory depression and mental status changes. 17 These effects increase the risk of aspiration and can ultimately lead to the development of pneumonia. Additionally, studies have shown that opioids have immunosuppressive properties. 18 By inhibiting the immune system, opioids can place patients at a higher risk for developing pneumonia as well as septicemia and shock—all of which were associated with potential ORADEs in this study.
Increased age was also found to be associated with potential ORADEs in our study, with the highest risk being in patients greater than the age of 80. This finding is consistent with other research in this area. 19 There are many reasons to explain the higher risk of ORADEs seen in patients of increased age. First, there are certain age-related pharmacokinetic changes seen in the elderly population that include a decreased metabolism and elimination of opioids. 12,20 These changes lead to increased levels of opioids and their active metabolites, which increases the risk of developing adverse effects. There is also an enhanced pharmacodynamic sensitivity, where more pronounced effects are observed in the elderly population at an equivalent dose compared to younger patients. 20 These more pronounced effects may lead to increased respiratory depression, confusion, and decreased gastrointestinal motility resulting in a higher risk of pneumonia, falls, nausea, and vomiting. Additionally, the increased number of comorbidities in elderly patients and the resulting polypharmacy may be a factor that increases the risk of ORADEs in the elderly population. 12,20
In an attempt to better monitor ORADEs, Stone et al created a system using data from the CMS National Administrative Database to identify potential ORADEs. 13 In using this system, we attempted to understand the impact of potential ORADEs in hip replacement surgery. Understanding this impact may lead health-care providers to question current management of postoperative pain and lead them to develop improved methods of pain management to reduce ORADEs.
Adequate pain relief has been described as a fundamental right and has been shown to lead to better patient and economic outcomes. 21 Opioids continue to be the primary form of treatment in perioperative pain management, yet up to 80% of postoperative patients report inadequate pain relief. 21 While the benefit of opioids in managing pain is well established, it is important to understand their limitations in pain management as well as the consequences potential ORADEs can have on patient care.
Specifically, in patients undergoing hip replacement surgery, it is important to understand the cost of ORADEs for several reasons. First, hip replacement surgery is one of the most common surgical procedures performed in the United States today and its incidence will continue to grow in the future. 10,11 With over 400 000 hip replacement surgeries done in the United States each year, even a modest ORADE rate of 8.6% can have a significant economic impact on our health-care industry. Another important reason to understand the cost of ORADEs is the fact that the elderly population comprises a large number of patients who undergo hip replacement surgery. Altered physiology, high number of comorbidities, and a high frequency of polypharmacy in this patient population all place them at an increased risk for ORADEs. 12,20 By understanding this increased risk for ORADEs, both major and minor, and their association with poor outcomes, health-care providers can focus on developing a pain management approach to limit adverse events and improve patient outcomes and satisfaction with their care.
Multimodal analgesia is gradually becoming a standard of care in managing both chronic and acute pain. It uses combinations of analgesic medications to manage pain with minimal or no opioid use. 22 Pain is multifactorial and involves many different pathways and mediators. By targeting these multiple pathways with combinations of systemic and regional analgesia, health-care providers can more effectively manage postoperative pain while reducing the use of opioids and the risk of ORADEs. 23 Multimodal analgesia is rapidly becoming commonplace in joint replacement surgery. 24 In a recent study by Memtsoudis et al, 85.65% of patients undergoing hip or knee replacement surgery received some form of multimodal analgesia. 24 Specifically, in hip replacement surgery patients receiving more than 2 modes of analgesia, there were 19% fewer respiratory complications, 26% fewer gastrointestinal complications, and an 18% decrease in opioid prescriptions compared to the use of opioids alone. 24 It is clear that multimodal analgesia is a safer form of pain management than management with opioids alone. While the optimal multimodal regimen is still not known, it is encouraging that health-care providers are making strides to decrease the use of opioids in perioperative pain management in hip replacement surgery. 24
There are several limitations to our study. First, this is a retrospective study using an administrative database. While the database is extensive, it only contains data on approximately 35% of inpatient hospital discharges in the United States, and the CMS database only includes patients aged 65 or above. With the median age of patients undergoing hip replacement surgery being 65 years, our data and analysis do not include information regarding younger patients. Also, since potential ORADEs were determined by certain ICD codes that are associated with ORADEs, it is possible these ICD codes were not related to opioid use and may have led to an overestimation of the ORADE rate. Additionally, the CMS LDS does not list specific medications given during hospitalizations. This lack of information makes it unclear as to whether opioid use caused an adverse event and therefore could lead to an overestimation of ORADE rate. Conversely, it is possible the rate of ORADEs was underestimated, which is an important potential finding of our study. Hospitals are limited in the number of ICD-10 codes that can be submitted and thus can neglect to include less severe complications in their claims data. Despite these limitations, we believe the large sample size from the CMS LDS, our methodology for identifying potential ORADEs, and the associations generated from the AHRQ CCS categories help to better understand how potential ORADEs may affect clinical and financial outcomes in hip replacement surgery.
Further research in this area should be conducted using data that include specific medications administered during a hospitalization as well as their timing in relation to when an adverse event occurs. This research would further strengthen the association between opioid use and adverse events in hip replacement surgery. Additionally, research should be conducted on various multimodal analgesic regimens, specifically in hip replacement surgery patients, to help determine most effective pain management strategies.
Conclusion
Patients who have recently undergone hip replacement surgery commonly experience potential ORADEs, both major and minor, which are associated with increased hospital LOS and decreased hospital revenue per day. Potential ORADEs, which our study has found occurring at rate of 8.6%, are also associated with certain patient risk factors such as increased age and male gender and may lead to poor outcomes such as pneumonia, septicemia, and shock. By reducing the use of opioids and employing a multimodal analgesic approach, we may improve patient care, decrease hospital lengths of stay, and increase hospital revenue.
Supplemental Material
Supplementary_table_1_-_NEW - Potential Opioid-Related Adverse Drug Events Are Associated With Decreased Revenue in Hip Replacement Surgery in the Older Population
Supplementary_table_1_-_NEW for Potential Opioid-Related Adverse Drug Events Are Associated With Decreased Revenue in Hip Replacement Surgery in the Older Population by Justin Baker, Ethan Y. Brovman, Nikhilesh Rao, Sascha S. Beutler and Richard D. Urman in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.