
Abstract
Introduction:
Postoperative outcomes in the elderly patients with intertrochanteric fracture were generally poor with a low rate of return to prefracture ambulatory level (RPAL). Recent studies showed that proximal femoral nail antirotation (PFNA) with cement augmentation might be useful for postoperative functional recovery. This study aimed to compare the outcomes in elderly patients with high surgical risk, American Society of Anesthesiologist (ASA) grade 3 or 4, who sustained intertrochanteric fractures and were treated with PFNA with and without cement augmentation, and to correlate perioperative surgical factors with the RPAL.
Methods:
A retrospective consecutive series was conducted based on 135 patients with prefracture ambulation classified as independent in community with or without a single cane (68 in augmented group and 67 in control group). Perioperative data and data on the complications within 1-year postsurgery were collected and compared. Predictive factors for RPAL were analyzed via logistic regression analysis.
Results:
The overall 1-year postoperative mortality rate was 10% (n = 14) with no significant difference between groups (P = .273). The proportion of elderly patients with RPAL in the augmented group was significantly higher than for those in the control group (48% vs 29%, P = .043). Via univariate analysis, ASA grade 4 (P = .077), history of stroke (P = .035), and use of cement augmentation (P = .041) were correlated with RPAL. However, multivariate regression analysis showed that ASA grade 4 (odds ratio [OR] = 0.40, 95% confidence interval [CI]: 0.18-0.90, P = .026) and use of cement augmentation (OR = 2.72, 95% CI: 1.22-6.05, P = .014) were the significant predictors for RPAL.
Discussion and Conclusions:
The results of the present study showed that PFNA with cement augmentation is safe and effectiveness in the intertrochanteric fracture treatment of elderly. Postoperative functional recovery, like RPAL, in elderly patients who sustained intertrochanteric fractures is relatively low, especially in those with ASA grade 4. However, cement augmentation with PFNA might be helpful for increasing the RPAL in high-surgical-risk geriatric patients.
Keywords
Background
Intertrochanteric fractures in elderly patients are one of the most common geriatric traumas, resulting in a major public health problem due to a high rate of mortality and morbidity, poor functional outcomes, and reduced quality of life. 1 -3 Although surgical fixation is the gold standard of treatment to achieve stable fixation and the ability to start early rehabilitation, previous studies showed that only a small number of elderly patients (18%-34%) could return to their prefracture ambulatory level (RPAL). 4 -6 This is because their postoperative functional recovery depends on many factors, such as patient demographics, comorbid disease, prefracture ambulatory level, muscle strength, perioperative complications, postoperative care, and early mobility level. 7 -10 Moreover, elderly patients are more likely to have difficulty with rehabilitation protocols due to the inability to maintain postoperative weight-bearing restrictions. 11 Elderly patients are also strongly associated with poorer recovery than younger patients requiring a prolonged time to recover ambulation levels. 12,13
Nevertheless, recent meta-analysis studies 14,15 demonstrated that a surgical option with great biomechanical property, as intramedullary nail (IMN), resulted in significantly better functional outcomes and higher RPAL than extramedullary implants (such as dynamic hip screw). Among IMN devices, the proximal femoral nail antirotation (PFNA) is one of the most preferable surgical options due to the biomechanical advantages of IMN and additional fixation stability from the helical blade design. 16,17 These factors improve the postoperative outcomes with PFNA via a very low fixation failure rate, less perioperative blood loss, and shorter length of hospital stay when compared to other devices. 18,19 Moreover, the PFNA system also provides the ability to augment the helical blade fixation in the femoral head with bone cement, without any harm to subchondral bone. 20 Cement augmentation with PFNA fixation has been found to increase the implant stability in osteoporotic intertrochanteric fracture. 21,22 In turn, the increased stability has resulted in many advantages, such as early full-weight bearing after surgery, facilitating postoperative functional recovery with an excellent clinical outcome without implant-related complications and osteonecrosis of the femoral head. 23,24
To the best of our knowledge, only a few previous studies have addressed the effect of PFNA with cement augmentation on RPAL 25 or compared the postoperative functional outcomes between elderly patients who sustained intertrochanteric fractures and treated with PFNA with and without cement augmentation. 26 We hypothesized that PFNA with cement augmentation would improve postoperative functional recovery and result in excellent clinical outcomes with significant increase of RPAL in elderly patients with intertrochanteric fractures, especially in those who had high surgical risk. Therefore, the present study aimed to report the comparative outcome in high surgical risk elderly patients treated with PFNA with and without cement augmentation and to correlate between perioperative surgical factors and RPAL in these patients.
Methods
This study was designed as a single-centered retrospective study that compared elderly patients with intertrochanteric fractures treated with a standard PFNA fixation in Faculty of Medicine Ramathibodi Hospital between 2010 and 2013 (control group), with the consecutive cases of those treated with PFNA and cement augmentation (augmented group) in the same center between 2014 and 2017. The study protocol was reviewed and approved by the institutional review boards at Mahidol University, based on the Declaration of Helsinki (COA no. MURA2019/158).
The inclusion criteria for patients were (1) aged older than 70 years, (2) having an isolated closed intertrochanteric fracture (AO 31-A1, A2, and A3) from low-energy trauma and treated with PFNA with or without cement augmentation, (3) having high surgical risk classified as American Society of Anesthesiologist (ASA) classification grade 3 or 4, and (4) having prefracture ambulatory level classified as independent in community ambulation without gait aids or using only single cane. 27 The exclusion criteria were (1) a pathologic fracture other than osteoporosis, (2) having high-energy trauma or multiple trauma or additional fracture other than intertrochanteric fracture, (3) having open fracture, (4) having active cancer; and (5) having a known hypersensitivity or allergy to any of the components in bone cement.
Surgical Procedure and Postoperative Protocol
After admission, all patients were rapidly optimized based on their medical conditions and sent for Doppler ultrasonography as a preoperative screening for deep vein thrombosis. 28 Surgery was generally performed within 48 hours after admission, unless an unstable medical condition was present. The decision on anesthesia technique depended on the anesthesiologist (T.C.). All operations were performed by 1 of 3 experienced orthopedic trauma surgeons. Regarding the control group, the fracture was reduced on a traction table, and the PFNA implant (Synthes, Oberdorf, Switzerland) was inserted with a minimally invasive technique, as previously reported. 29,30 In the augmented group, the perforated blade was used instead of the standard one, and the cement augmentation was performed with a 3 to 4 mL high-viscosity polymethyl methacrylate (PMMA) cement (Traumacem, Synthes) under image intensifier using the standard technique. 31 One static distal locking screw was inserted before wound closure.
The postoperative care protocol was identical in both groups. Mechanical venous thromboembolism (VTE) prophylaxis using early mobilization and intermittent pneumatic compression was applied in all patients. Pharmacological prophylaxis with anticoagulants was given to the patients at high risk for VTE, such as having previous VTE, history of malignancy, and those who had delayed surgery. All patients were allowed to perform weight-bearing exercise on the injured hip with a walker as tolerated. Radiographic and clinical follow-ups were scheduled at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year postoperatively.
Data Collection and Outcome Measurement
The demographic data included the following: age, gender, body mass index (BMI), prefracture ambulatory level classified on the basis of standard definitions of community and household ambulation, 27 ASA physical status, 32 comorbidity disease, and fracture classification according to Arbeitsgemeinschaft für Osteosynthesefragen/orthopaedic trauma association (AO/OTA) classification. 33 Age and comorbid diseases were further used for calculating the Charlson Comorbidity Index (CCI). 34 The following perioperative information was recorded: preoperative laboratory values (hemoglobin, lymphocyte count, glomerular filtration rate [GFR], and albumin), time from admission to surgery, anesthetic technique, operative time, intraoperative blood loss, number of packed red cell (PRC) transfused units, and length of hospital stay.
Data about perioperative complications and postoperative outcomes within 1 year related to hip fracture surgery were also collected; these included death, ambulatory level at 1 year, 27 surgical complications (intraoperative fracture, nerve and vascular injury, and wound complication), and medical complications (infection, delirium, VTE event, cardiac complication, pulmonary complication, gastrointestinal complication, renal complication, and pressure ulcer). 35 The postoperative radiographs were evaluated by 3 authors for the position of helical blade according to Cleveland and Bosworth, 36 the sliding length of blade by comparing between the initial and 1-year postoperative radiographs, 37 and the time for fracture union. Return to their prefracture ambulatory level was defined as the recovery of 1-year postoperative ambulatory level to the preinjury ambulatory level.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) software version 18.0 was used to analyze the data. Continuous data with normal distribution were presented as means and standard deviations, and compared with t test. Meanwhile, those with non-normal distribution were presented as medians and interquartile ranges and compared to Mann–Whitney U test. Categorical data were presented as a proportion of cases and compared with Fisher exact test or χ2 test as appropriate. Risk factors for RPAL were compared between the patients with and without RPAL. Univariate logistic regression analysis was used to evaluate the association between risk factors and RPAL, and the predictive factors with values of P < .10 were calculated by multivariate logistic regression analysis. Significance was defined as values of P < .05.
Results
General Characteristic Data of the Study Population
This study included a total of 135 (36 males and 99 females) patients. All patient demographic data and the comparison of preoperative data between patients treated with PFNA with (n = 68) and without cement augmentation (n = 67) are shown in Table 1. The average patient age was 84 ± 6 years (range 71-96 years). Eighty-eight (50.4%) were classified as ASA grade 3, while 67 (49.6%) patients were assessed as ASA grade 4. The fractures were categorized as A1, A2, and A3 in 30 (22.2%), 97 (71.9%), and 8 (5.9%) patients, respectively. Prefracture ambulatory level was classified as independent ambulator (IA) without gait aids and IA with single cane in 62 (45.9%) and 73 (54.1%) patients, respectively. The median time to surgery was 35 hours (range 2-347 hours). Proximal femoral nail antirotation was used in 67 (49.6%) patients, whereas PFNA with cement augmentation was used in 68 (50.4%) patients. Regarding the data comparison between those treated with PFNA with and without cement augmentation, no significant difference in age, gender, BMI, CCI, fracture classification, time of surgery, and prefracture ambulatory level was found in either group (P > .05 all). Comorbid diseases—diabetes, hypertension, ischemic heart disease, chronic kidney disease, cancer, and dementia—and preoperative laboratory values (eg, hemoglobin, GFR, and albumin) were also not significantly different between groups (P > .05 all). However, a significantly higher proportion of patients treated with PFNA with cement augmentation were ASA grade 4, but a significantly lower proportion had comorbidities of stroke, chronic obstructive pulmonary disease, and lymphocyte count, compared to those with PFNA (P < .05 all).
Demographic Data in 135 Elderly Intertrochanteric Fracture Patients and Comparison Between Those Treated With PFNA With and Without Cement Augmentation.
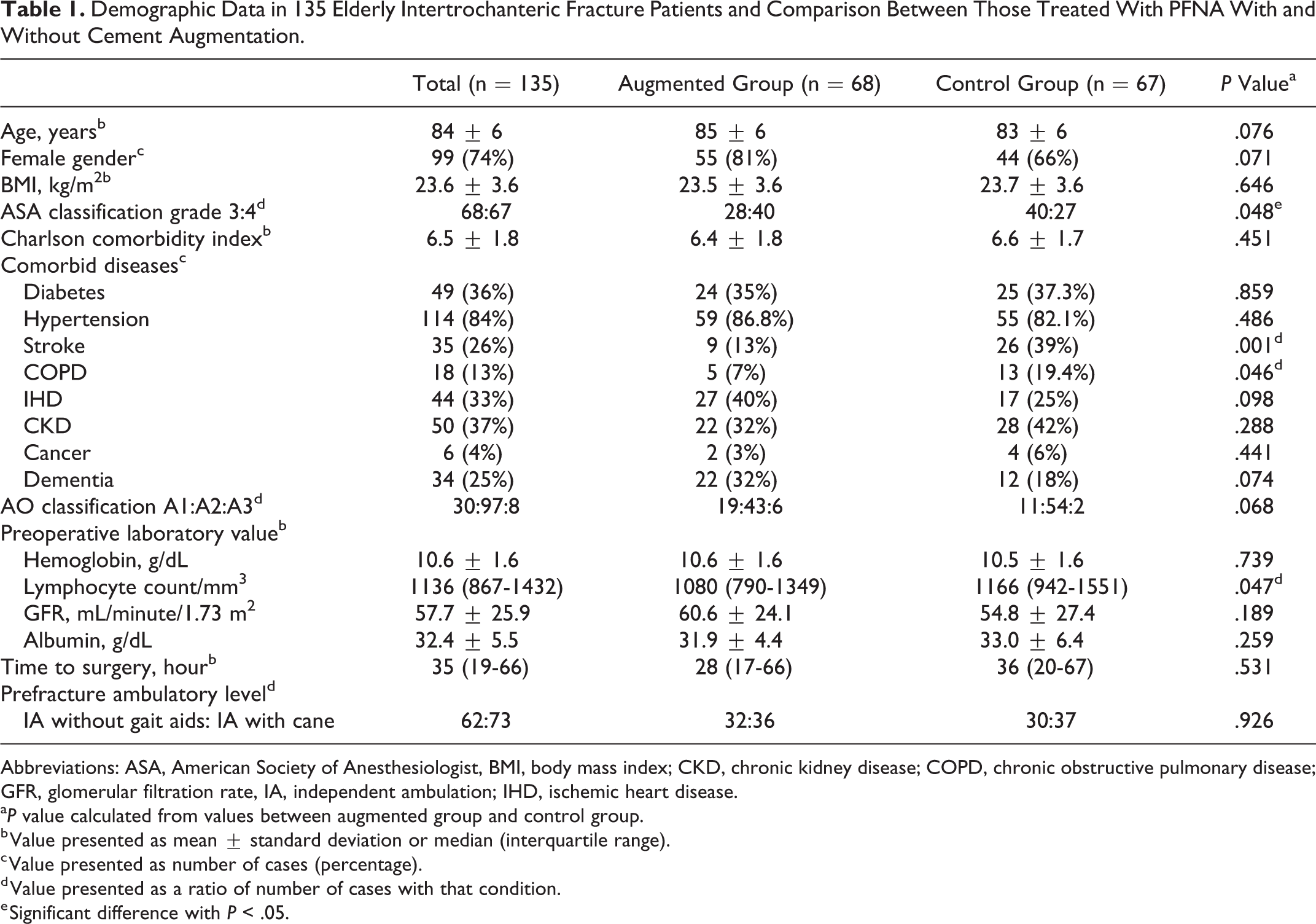
Abbreviations: ASA, American Society of Anesthesiologist, BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; GFR, glomerular filtration rate, IA, independent ambulation; IHD, ischemic heart disease.
a P value calculated from values between augmented group and control group.
b Value presented as mean ± standard deviation or median (interquartile range).
c Value presented as number of cases (percentage).
d Value presented as a ratio of number of cases with that condition.
e Significant difference with P < .05.
Perioperative Data and Postoperative Outcomes
Table 2 illustrates the comparison of perioperative data and postoperative outcomes between the patients treated with PFNA with and without cement augmentation. There was no significant difference in anesthetic technique, operative time, blade position, intraoperative blood loss, PRC transfusion, overall perioperative complication, time to union, 1-year readmission rate, and 1-year postoperative mortality between groups (P > .05 all). However, compared to the control group, the augmented group showed a significantly higher incidence of perioperative delirium (4% vs 18%, P = .014), a smaller blade sliding length (3.8 vs 5.0 mm, P = .033), shorter length of hospital stay (6 vs 8 days, P = .008), and higher in proportion of RPAL (48% vs 29%, P = .043). Postoperatively, 14 patients (5 in the augmented group and 9 in the control group) died within 1-year post-operation. Therefore, only 121 patients were accessible for assessing ambulatory level and available for regression analysis.
Comparison of Perioperative Data and Postoperative Outcomes Between the Elderly Intertrochanteric Fracture Patients Treated With PFNA With and Without Cement Augmentation.

Abbreviations: GA, general anesthesia; PRC, packed red cell; RA: regional anesthesia.
a P value calculated from values between augmented group and control group.
b Value presented as a ratio of number of cases with that condition.
c Value presented as mean ± standard deviation or median (interquartile range).
d Value presented as number of cases (percentage).
e Significant difference with P < .05.
Risk Factors for RPAL
The relationship between each factor and the RPAL is shown in Table 3. A simple comparison revealed that the patients who could RPAL, compared to those who could not, had a lower proportion of history of stroke (15% vs 32%, P = .035), greater number of cement augmentation applications (64% vs 45%, P = .043), and shorter length of hospital stay (6 vs 8 days, P = .048).
Simple Comparison Between the 121 Elderly Intertrochanteric Fracture Patients Who Could and Could Not Return to Prefracture Ambulatory Level at 1-Year Postoperatively.
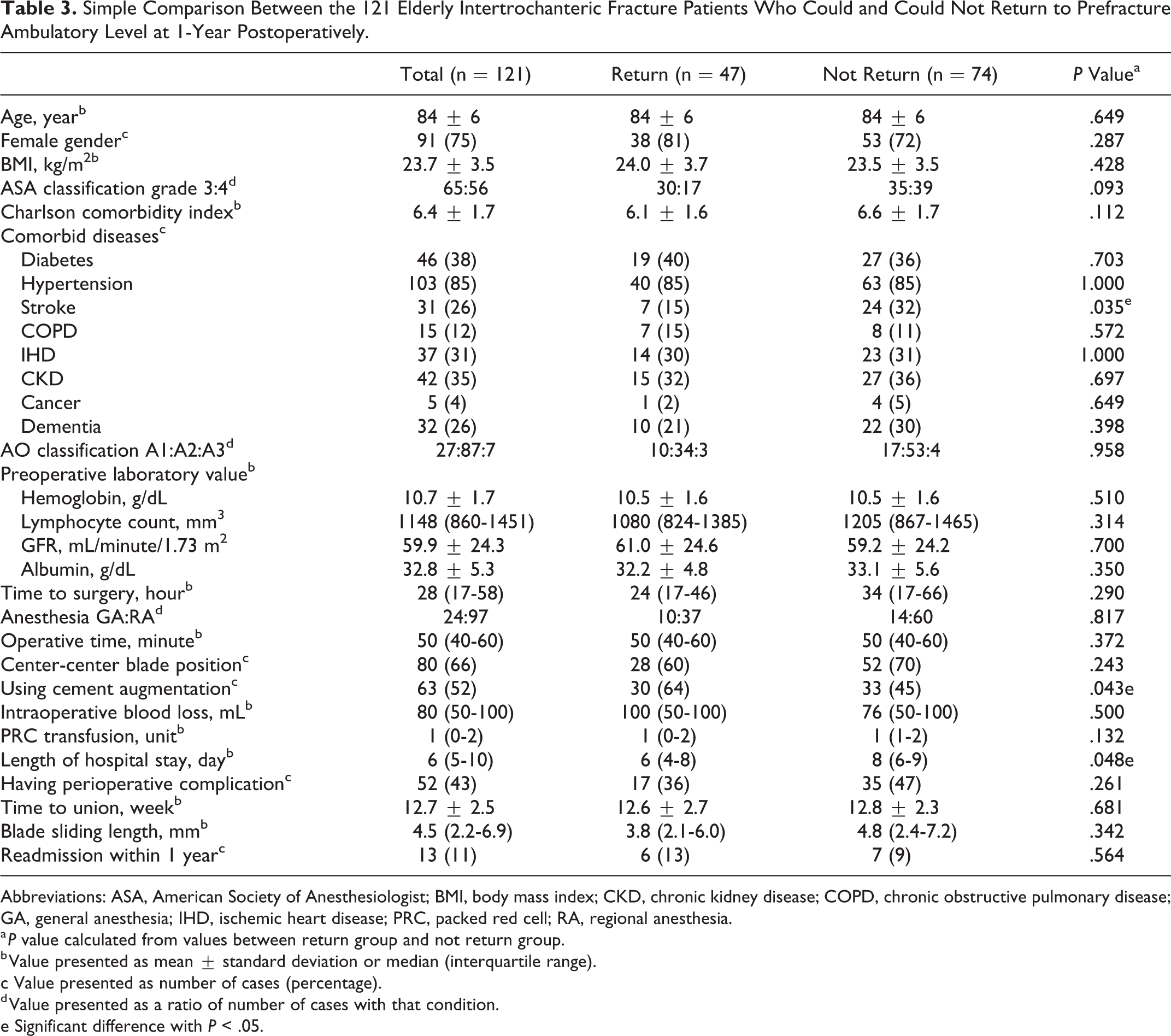
Abbreviations: ASA, American Society of Anesthesiologist; BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; GA, general anesthesia; IHD, ischemic heart disease; PRC, packed red cell; RA, regional anesthesia.
a P value calculated from values between return group and not return group.
b Value presented as mean ± standard deviation or median (interquartile range).
c Value presented as number of cases (percentage).
d Value presented as a ratio of number of cases with that condition.
e Significant difference with P < .05.
Table 4 shows the univariate and multivariate regression analyses of the predictive factors for the return to prefracture ambulation in 121 elderly intertrochanteric fracture patients. Via univariate analysis, the predictive factors significantly associated with the RPAL with P < .10 were ASA grade 4 (P = .077), history of stroke (P = .035), and use of cement augmentation (P = .041). Nonetheless, multivariate logistic regression analysis revealed that the significant independent predictors for RPAL were ASA grade 4 (odds ratio [OR]: 0.40, 95% confidence interval [CI]: 0.18-0.90, P = .026) and use of cement augmentation (OR: 2.72, 95% CI: 1.22-6.05, P = .014; Table 4). The area under the curve for this model was 0.649 (95% CI: 0.557-0.733).
Logistic Regression Analysis for the Predictive Factors of Return to Prefracture Ambulatory Level at 1-Year Postoperatively in the Elderly Patients Having Intertrochanteric Fracture.a

Abbreviations: ASA, American Society of Anesthesiologist; BMI, body mass index; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; GFR, glomerular filtration rate; IHD, ischemic heart disease; OR, odds ratio; PRC, packed red cell; MVA, multivariate analysis; UVA, univariate analysis.
a n = 121.
b Significant difference with P < .05.
Discussion
Postoperative functional recovery is one of the most important clinical outcomes after hip fracture treatment in elderly patients and an interesting area for developing research in the treatment of elderly hip fractures. 38 This study aimed to demonstrate the outcomes of high surgical risk geriatric patients with intertrochanteric fractures who had been treated with PFNA fixation with and without cement augmentation and to correlate the RAPL at 1-year postoperatively with the perioperative factors.
The results showed that, after surgical treatment, these high-risk elderly patients who had prefracture ambulation as IA without gait aids or IA with single cane still had poor postoperative outcomes with an overall 1-year mortality rate of 10%, which was not significantly different between groups (7% in augmented group vs 13% in control group, P = .273). However, the augmented group showed a significantly higher rate in RPAL (48%) than the control group (29%); these results were comparable to the previous studies on elderly hip fractures. 4,12,25 Our findings also revealed that RPAL was predictable given the factors of ASA grade 4 (OR: 0.40, 95% CI: 0.18-0.90, P = .026) and use of cement augmentation (OR: 2.72, 95% CI: 1.22-6.05, P = .014; Table 4). This finding supports that severe comorbidities with ASA grade 4 are useful as a significant risk factor for poor postoperative functional recovery in elderly hip fracture patients. 9 The increase of RPAL in the augmented group might be explained by how the cement augmentation had improved the mechanical stability of the fixation construct, especially in the severe osteoporotic bone, resulting in a significant postoperative reduction of pain on weight-bearing ambulation and, therefore, ensuring early functional recovery. 31,39,40
Nevertheless, although the present study demonstrated that the cement augmentation with PFNA is significantly associated with the higher rate of RPAL in these elderly patients, the findings are not comparable with the previous study by Kammerlander et al, which showed no significant difference in the postoperative walking speed, assessed by the Timed Up and Go (TUG) test, between those treated with PFNA with and without cement augmentation. 26 This might be explained by the different functional outcome assessment methods between the previous study (TUG) and our study (RPAL). Although TUG is a simple tool to assess the walking ability and physical mobility in hip fracture patients and is known to provide valuable prognostic information about postoperative functional recovery, this test is unable to perform preoperatively in hip fracture patients; the studies on TUG were focused on femoral neck fracture treated with hemiarthroplasty. 41 Besides, TUG was not a suitable tool for predicting the walking ability at 1-year postoperation due to the low sensitivity and specificity. 42 Moreover, 42.5% of patients in the previous study could not perform the postoperative TUG test due to mortality and withdrawal, which could affect the statistical power of analysis. Therefore, in our opinion, the simpler functional outcome with RPAL would be useful and more applicable in elderly patients who have sustained intertrochanteric fractures.
None of the mechanical failures, symptomatic implant migrations requiring reoperation, and complications related to cement augmentation were found in this study, comparable to the results from previous studies. 24,26,31 Therefore, our findings confirm that cement augmentation with PFNA is safe and advantageous in the surgical treatment of high surgical risk elderly patients with intertrochanteric fractures.
Nevertheless, this study has some limitations. First, it was retrospective, which potentially makes it imperfect given the nature of the study and the completeness of the patient medical records. Second, our sample size was also relatively small and might not be able to detect other significant prognostic factors related to the PFNA with and without cement augmentation. Finally, our results from the use of PFNA with or without cement augmentation might not be directly applicable to other surgical options due to the differences in implant design and biomechanical properties. Therefore, a multicentered prospective study with a larger sample size should be performed to discover the genuine effect of cement augmentation with PFNA fixation in elderly patients with intertrochanteric fractures.
Conclusion
This study revealed that the functional recovery toward the prefracture ambulatory level in elderly patients with intertrochanteric fractures treated with PFNA is low, with an RPAL of only 39%. However, RPAL significantly correlates with the ASA grade-4 comorbid status. Moreover, our findings suggest that cement augmentation with PFNA might improve the postoperative functional outcome for high surgical risk geriatric patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.