
Abstract
Introduction:
Malnutrition is common in older people, is known to interact with frailty, and is a risk factor for wound complications and poor functional outcomes postoperatively. Sustaining a hip fracture is a significant life event, often resulting in a decline in mobility and functional ability. A poor nutritional state may further impede recovery and rehabilitation, so strategies to improve perioperative nutrition are of considerable importance. We provide a review of nutritional supplement practices in this vulnerable and growing population.
Method:
Systematic review of preoperative oral nutritional supplementation (ONS) in hip fracture patients.
Results:
We identified 12 articles pertaining to this important area of perioperative care. The findings suggest postoperative ONS can improve postoperative outcomes in hip fracture patients, especially in terms of increasing total serum protein, improving nutritional status to near-optimum levels, and decreasing postoperative complications.
Discussion:
There is an absence of evidence specific to preoperative ONS in patients admitted following hip fracture. Literature relating to other populations is encouraging but is yet to be robustly studied. It is unclear whether these results are generalizable to the frailer hip fracture population. There is a need for studies clearly defining outcome measurement and complication assessment pertaining to preoperative ONS. The potential benefit is considerable, and this review will provide a means to inform the construction of meaningful trials in preoperative ONS of patients sustaining hip fracture.
Conclusion:
Oral nutritional supplementation in hip fracture patients may decrease postoperative complications while increasing elderly patient’s nutritional state to a near-optimum level. This is extrapolated from postoperative literature, however with a clear gap in research pertaining specifically to preoperative care. The need for well-constructed studies focused on the impact and assessment of early ONS in this population is transparent.
Keywords
Introduction
In the United Kingdom, over 65 000 patients attend hospital with a hip fracture annually, the most common reason for admission to an orthopedic ward. 1,2 The incidence is rising, with an estimated 11.9% more patients presenting with hip fractures by 2030 compared to 2010. 3 Morbidity and mortality are high, with mortality rates of 27.3% at 1 year post fracture. 4 In direct health-care costs, a single hip fracture measures approximately £25 000 per episode, nearly £1 billion per annum for the United Kingdom alone. 5,6
Over 25% of elderly patients admitted to hospital are malnourished, 7 leading to apathy, depressed mood, and worsening cardiorespiratory dysfunction. 8 For these reasons, mobility and recovery from surgery are impaired, increasing the risk of pneumonia, pressure ulcers, deep vein thrombosis, and wound infection. 9 Recent data from the UK National Hip Fracture Database found up to 24.5% of hip fracture patients were malnourished. 10
Oral nutritional supplementation (ONS) are solids or liquids containing macronutrients that augment background nutritional intake. Some ONS are carbohydrate (CHO) predominated, while others focus on protein delivery. Generic ONS use and benefits toward reducing mortality, complications, and length of hospital stay have been studied before. However, their focus is on postoperative strategies to optimize recovery and/or are based on preoperative supplementation in elective surgeries. There is little literature addressing preoperative supplementation related to hip fracture surgery and outcomes.
Materials and Methods
Evidence search was undertaken using the “Ovid” search system. Databases searched include MEDLINE, Embase, the Cochrane library, and NICE evidence search. Search terms, “Oral Nutrition” or “Oral Supplement” or “Nutritional Intervention” or “Nutritional Supplement,” “Hip Fracture” or “Hip Surgery” or “Intertrochanteric Fracture” or “Femoral Neck Fracture,” and “Old” or “elderly,” were used to search titles, abstracts, and subject headings. The initial search results were supplemented with reference lists and expert consultation to reduce the risk of missing eligible studies.
Inclusion criteria used for selection are as follows: (1) randomized controlled trial (RCT), (2) reporting hip fracture outcomes, (3) intervention included ONS, and (4) outcomes reported included complication rates or mortality or feasibility and were relevant.
After initial screening of titles and abstracts, any articles not relevant (not regarding hip fractures/ONS/complication data) were excluded. Remaining articles were analyzed full text and decided if they were relevant to the review.
Results
A total of 307 articles were screened for inclusion/exclusion based upon titles and abstract (see Figure 1). Thirty-seven articles were identified for full-text review. The final 12 articles fulfilled the inclusion criteria, forming the basis of this systematic review. Key themes from each article are discussed in turn.
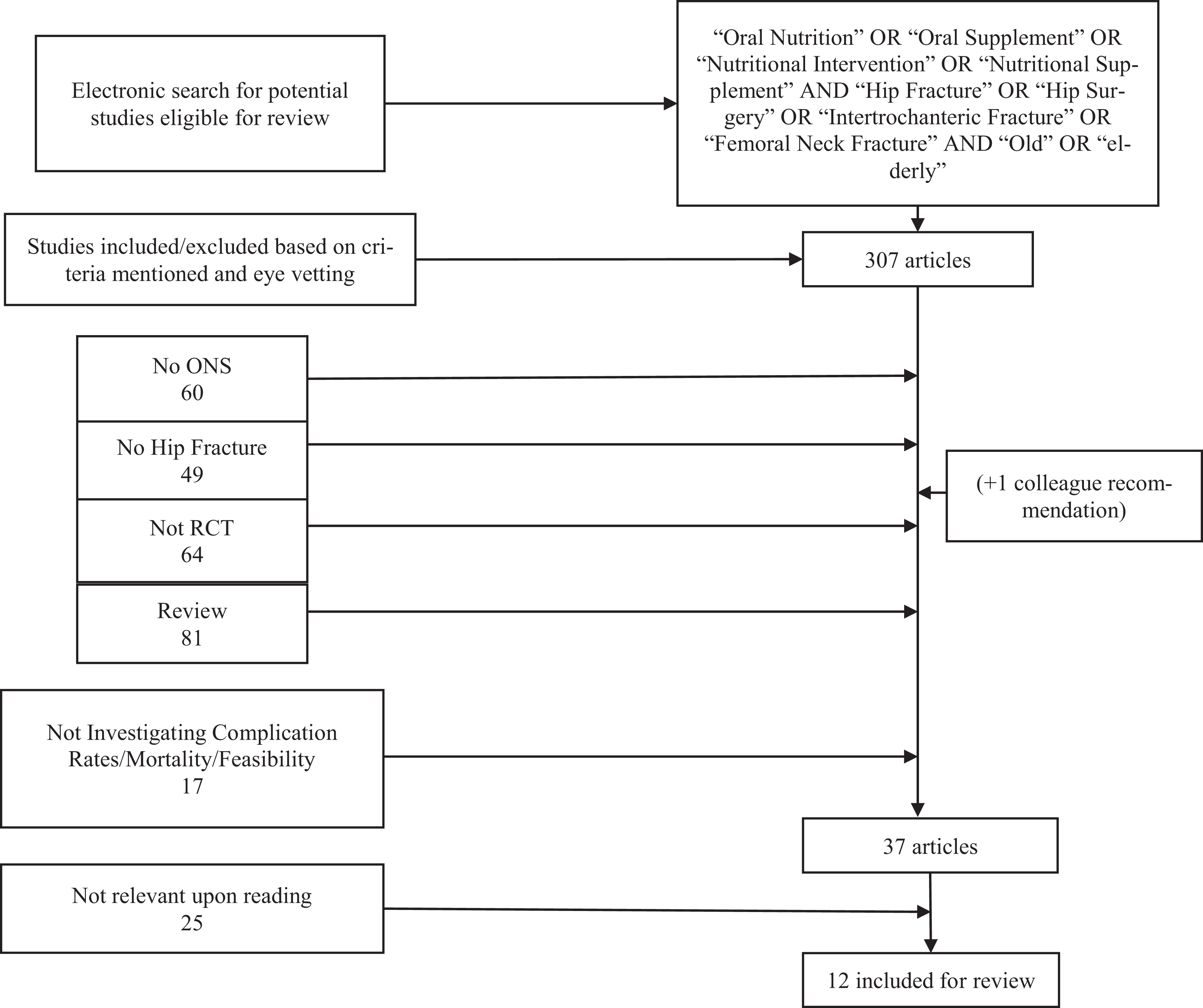
How papers were included/excluded from the review.
Preoperative Starvation for Hip Fracture Patients
Patients are kept “nil by mouth” to prevent aspiration during induction of anesthesia. One variable directly associated with eventual surgical outcome is insulin resistance (IR). Surgery and trauma lead to an increase in IR due to preoperative fasting. 11
With the “triple hit” of trauma, surgery, and presurgery fasting, patients enter a catabolic state resulting in reliance on glycogen and fat stores from the liver, leading to IR affecting the uptake of glucose into cells. 12 Patients who are undernourished do not have the adequate stores of glycogen or fat to deal with the trauma of surgery, leading to greater physiological upset of IR, lasting up to 3 weeks. 13,14 This puts patients at a greater risk of complications, leading to a state of hyperglycemia.
Preoperative starvation time should be kept as short as possible. The American Society of Anesthetists suggest preoperative fasting times of 6 hours for food and 2 hours for clear liquids.
However, evidence shows times are often longer in practice, 15 increasing thirst, anxiety, hunger, and IR risk before surgery. Additionally, multiple studies have shown prolonged fasting times are a risk factor for delirium in elderly patients. 16,17 Delirium is shown to be an independent risk factor for increased mortality and complications after major surgery, 18 with trend showing functional decline between 1 and 12 months after surgery. 19
Oral nutritional supplemental interventions before surgery can shift the body’s metabolic state toward anabolism through inducing CHO storing, in turn reducing starvation-induced IR. 12 A Cochrane review showed preoperative CHO loading can decrease length of stay in hospital up to 1 day compared to a fasting group. 20 Additionally, CHO ONS administered 2 to 4 hours preoperatively reduces postoperative IR state. 21
Supplementation in Hip Fracture
Of the 12 articles found regarding ONS in hip fractures, 10 articles reported the effect of the supplements after surgery. Only 2 studies implemented any nutrition intervention on admission or before surgery: Breedveld-Peters et al 22 and Botella-Carretero et al. 23 One meta-analysis by Liu et al was selected for review, 24 including 6 articles found during our literature search.
Preoperative Nutrition
Botella-Carretero et al 23 performed an RCT comparing oral supplementation with a nonintervention control group in adults aged ≥65 years. Strict exclusion criteria were applied to moderately to severely malnourished patients (as hospital guidelines provided ONS for these individuals), significant comorbidity (such as renal, liver, or respiratory failure), or any supplementation for the previous 3 months.
The study reported outcomes of 60 patients, a 30-patient control arm, and a 30-person intervention group who received Fortimel (Nutricia, Trowbridge, Wiltshire, UK) 200 mL drinks. Each drink provided 20 g of protein and 200 kcal. The intervention group received 40 g of protein from 2 drinks and 400 kcal daily starting from admission and continued after surgery.
The study found a larger decrease in serum albumin levels for the control group versus the intervention group (P < .001). Additionally, they found worse postoperative recovery when compared to the intervention group (P = .002) relating to speed of return to baseline for serum albumin, prealbumin, and retinol-binding globulin, measured before surgery, 48 hours postsurgery, 1 week after surgery, and at hospital discharge. Lower serum albumin is a known predictor for postsurgical complications, 25 with higher rates of complications and length of hospital stay for patients in states of hypoalbuminemia. 26
Postsurgical recovery was poorer in the control group. The authors noted a nonsignificant tendency for more postoperative complications in the control group (40% of patients in the control group had complications vs 20% in the ONS group). Furthermore, postoperative stay in hospital was similar between the groups, and postoperative mobilization was attained at similar times between the 2 groups. Total hospital stay was similar. Botella-Carretero et al 23 concluded patients with greater protein intake had better outcomes when the multivariate analysis of data was performed.
Feasibility of ONS Supplementation
Breedveld-Peters et al performed an open-label RCT investigating the feasibility of ONS and dietetic advice as an intervention in patients aged ≥55 years.
As part of the intervention, all patients were advised to consume 2 bottles of ONS daily between meals. The supplement was milk-based (Cubitan) by Nutricia Advanced Medical Nutrition (Trowbridge, Wiltshire, UK). The macronutrient breakdown of the drink was similar (500 kcal and 40 g of protein per 2 bottles) to the supplement used by Botella-Carretero et al. 23 The control group received the usual nutritional care provided by the hospital—that is, dietetic care or ONS was only provided on demand of the doctor in charge.
Of the 73 intervention group patients, 4 died during the study and 3 withdrew. The 66 remaining had a mean age of 76 years (range: 55-92 years) and consisted of 49 (74%) women and 17 (26%) men.
Of the 66 patients who completed the study, 55 (83%) received all 10 dietician contacts and 58 patients (88%) took the ONS for the recommended period. The authors concluded nutritional intervention in elderly hip fracture patients is feasible based on the parameters listed within the study.
Both groups of authors agreed there is a lack of research in the area of nutritional intervention. High-quality prospective randomized trials are needed to provide evidence of ONS impact, feasibility, and its effect on important surgical outcomes, such as mortality and postoperative complications.
Duncan et al 27 undertook an open prospective RCT of 318 patients in order to investigate the use of dietetic assistants in the outcome of hip fractures. The primary outcome was assessing postoperative mortality in the acute trauma unit with secondary measures of postoperative mortality at 4 months post fracture, length of stay, and nutritional status. They reported 2 part-time dietetic assistants working interchangeably to ensure the trauma unit had cover 7 days a week cost £13 000 annually. This study included patients with cognitive impairment unlike Breedveld-Peters et al, 22 highlighting the affordability of nutritional care.
Benefits of Perioperative Nutrition
Liu et al 24 performed a meta-analysis assessing whether perioperative ONS would be beneficial for rehabilitation of elderly patients after hip surgery. Inclusion criteria for the meta-analysis were RCTs with patients ≥65 years of age, who had hip fractures, and who received intervention using ONS. The 10 RCTs involving 986 patients were included.
The main outcomes for the meta-analysis were total protein measurement, complications, change in serum albumin levels, and mortality. Liu et al 24 found there was a statistically significant increase in total protein levels in patients who had received ONS.
Tidermark et al, 28 Neumann et al, 29 Espaulella et al, 30 Delmi et al, 31 and Botella-Carretero et al 23,32 evaluated effect of ONS on complications. Overall, the analysis was of the outcomes of 463 patients consisting of 220 ONS patients and 243 control patients. Liu et al 24 used a composite outcome measure categorizing complications into wound infection, respiratory infection, and urinary tract infections.
Three studies (Botella-Carretero et al, 23 Delmi et al, 31 and Neumann et al 29 ) reporting the outcomes of 199 patients (102 control vs 97 ONS) reported the ONS group had a lower rate of wound infection compared to the control group (1 event vs 10), and there was no evidence of heterogeneity in the trials (I 2 = 0%, P = .83).
For respiratory infection, pooled results from 3 studies (Botella-Carretero et al 32 , Delmi et al, 31 and Neumann et al 29 ) involving 200 patients (100 ONS vs 100 control) showed there was a significant statistical lower baseline length of hospitalization in the ONS group according to the 3 studies. There was a higher rate of respiratory infections within the control group versus the ONS group (10 events vs 2), with no statistical significance of heterogeneity (I 2 = 21%, P = .28).
For the occurrence of urinary tract infections, pooled results from 3 studies (Botella-Carretero et al, 32 Delmi et al, 31 and Neumann et al 29 ) involving 200 patients showed there was significant differences in favor of ONS between the 2 groups both on baseline and on hospitalization time, with no evidence for heterogeneity between the studies (I 2 = 0%, P = .90).
Results for the serum albumin change were pooled results from 3 studies (Bruce et al, 33 Neumann et al, 29 and Tidermark et al 28 ) with a total of 172 patients. The change in serum albumin did not have any statistically significant difference between the ONS and control; however, heterogeneity in the patient populations was found to be large and statistically significant between these studies, potentially invalidating the meta-analysis (I 2 = 97%, P < .00001).
Results for mortality came from 5 studies (Bruce et al,
33
Delmi et al,
31
Espaulella et al,
30
Neumann et al,
29
and Tidermark et al
28
Liu et al 24 is the largest scale research regarding hip fracture nutrition and supplementation, providing large numbers of participants for conclusions to be drawn upon, making the data more reliable. There are limited numbers of articles regarding nutrition, most of which are small scale (<100 participants). Furthermore, data about quantity, compositions, and timing of nutritional supplements were not reported consistently in any of the reported studies.
Houwing et al 34 performed a double-blind, placebo-controlled randomized trial assessing the effect of nutritional supplementation on the prevention of pressure ulcers. The study included 103 hip fracture patients, 51 of which received 400 mL of daily supplement adding 500 kcal and 40 g of protein to their daily diet, along with a mixture of zinc, arginine, and antioxidants. This was compared to a 51-person control group who received a non-caloric-based water placebo. The stages of pressure ulcers were monitored for 28 days, daily until discharge.
The study found incidence of pressure ulcer did not differ between the intervention and placebo groups (55% vs 59%, respectively). There was instead a trend of later onset of pressure ulcers within the supplemented group versus the control.
These results reflect the study by Liu et al, 24 showing complication rates are considerably lower in supplemented groups compared to the control groups. Houwing et al 34 concluded nutritional supplementation may be more effective if initiated earlier.
Eneroth et al 35 performed an RCT to determine whether combinations of intravenous and oral supplementation during the first 10 days of hospitalization decreased fracture-related complications. Enroth et al 35 randomized 80 patients into either the intervention group or the control group. The control group received regular hospital food, while the intervention group received the hospital food plus 1000 mL Vitrimix (Kabi Pharmacia AB, Stockholm, Sweden) for 3 days followed by Fortimel 2 × 200 mL daily. Vitrimix is a 1 kcal/mL mixture containing amino acids, sodium, potassium, magnesium, calcium, and chloride. The Fortimel energy content is 100 kcal/100 mL, including 10 g of protein, 10.3 g of CHO, and 2.1 g of fat.
Results showed that combined oral and parenteral supplementation increased the daily nutritional intake of the intervention group to near-optimum levels (nutrition levels based on basal demand of 25 kcal/kg body weight/day and fluid levels based on 30 mL/kg body weight/day). Daily, the control group received only 54% of their optimal nutritional intake and 64% of optimal fluid intake, supporting evidence that hip fracture patients suffer from malnutrition. 36 -38
Patients within the intervention group had fewer postoperative complications at 10−30 days postoperatively and 4 months. Overall 15% of patients in the intervention group had 1 or more complications versus 70% in the control arm.
Similar results were found in the study by Duncan et al, 27 where results showed patients being supported by dietetic assistants received on average 349 kcal/24 hour greater than the control nursed group that showed an average of 756 kcal/24 hour. This result was statistically significant (P < .001) and clinically relevant. Both the nursed and the dietetic assistant group received nutritional supplementation along with the hospitals hip fracture care guidelines; however, it was found the patients cared for by the dietetic assistants consumed 286 kcal/24 hour significantly more (P < .001) of their nutritional supplementation than the 123 kcal/24 hour of patients receiving the standard care.
Discussion
Perioperative supplementation for hip fracture patients has clear benefits. While current studies have shown it may have no effect on mortality, ONS is shown to reduce complications and increase optimal nutritional status within the elderly individuals as reported by Liu et al 24 and Eneroth et al. 35
Additionally both Liu et al 24 and Botella-Carretero et al 23 agree supplementation results in a statistically significant increase in serum protein which can improve operative outcomes.
There have been other articles regarding preoperative nutrition, suggesting it is more beneficial than a purely postoperative approach in gastrointestinal surgery and obese, diabetic, and geriatric patients. 39,40 From the IR stand point, it would be beneficial to keep patients in a CHO- and calorie-loaded state in order to reduce the hyperglycemic and catabolic effect of surgery. Further trials reporting the effects of preoperative ONS are needed. Not only would the preoperative nutrition potentially affect surgical outcomes, but it would also reduce patients’ hunger, thirst, and anxious.
There is a further evidence gap relating to hip fracture patients with cognitive impairment. Three studies (Eneroth et al, 35 Breedveld-Peters et al, 22 and Espaulella et al 30 ) excluded patients with dementia or other cognitive issues due to the assumption of decreased compliance with the ONS regimen. This makes generalizing results from these studies difficult, especially as patients with cognitive impairment carry the highest risk of being poorly nourished. Up to 42% of patients with severe cognitive impairment being malnourished. 41 This indicates potential for research projects to investigate how ONS could be used in populations of dementia/delirium patients before surgery.
A recent Cochrane review by Avenell et al 42 looked at 41 RCTs (3881 participants) evaluating nutritional intervention in hip fracture. Evaluation of all the research concluded data were of very low-to-low quality due to high risks of bias and limitation of definitions regarding complications. The review followed up by stating due to the small number of participants and insufficient ascertainment of important outcomes, the data from nutritional studies in hip fractures were imprecise. The reviewers proposed further RCTs to focus on oral multinutrient supplementation. Furthermore, information on nutritional status and supplements should be widely collected in audits in order to investigate the relationship of nutritional status with outcome. This study had a greater number of RCTs as it searched more databases and included nutritional interventions such as parenteral and enteral, whereas we specifically chose ONS as the primary type of nutrition (Eneroth et al used parenteral supplementation along with ONS).
From Breedveld-Peters et al, 22 the feasibility and adherence rates to perioperative ONS were shown to be high, although patients with dementia were excluded. Prices per unit of drink in the United Kingdom range from £1.50 to £2 per unit of ONS according to St George’s Healthcare guidance. 43
With the potential to reduce complications, long term it may be cost-effective for the National Health Service to introduce preoperative and postoperative into standard practice. Within the NICE guidelines, there is no information relating to oral nutritional supplementation in hip fractures. 44 The omission of nutrition guidance from hip fracture–specific guidelines is surprising, given the population at risk.
Conclusion
There is plentiful evidence supporting ONS use in a perioperative environment. It is relatively cheap, associated with reduction in many complication types, returns elderly patients to a more nourished state, and has high rates of adherence when studied. However, there is a clear lack of research around preoperative nutrition. High-quality RCTs are required to investigate outcomes on postoperative complications. In particular, there needs to be an assessment of outcomes and especially those relating to thirst and patient comfort. There should be further trials that investigate oral nutritional supplementation in those with cognitive impairment as sometimes this population is excluded from trials.
For the future, there is potential for preoperative supplementation to be started globally to this population on admission, or earlier in the prehospital phase of care, in order to return elderly patients to a more optimum nutritional state and reduce the chance of complications in concordance with NICE’s nutrition support in adults guide. 45
Footnotes
Author’s Note
William Eardley is also affiliated with Clinical Trials Unit, Department of Health Sciences, University of York, United Kingdom.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.