
Abstract
Introduction:
The worldwide incidence of fragility fractures is increasing and the greatest burden is borne by the oldest population. Mobile Outreach, an innovative orthopedic-based program providing on-site musculoskeletal care for individuals in nursing care facilities, was implemented as part of our Geriatric Orthopaedic Trauma Program. The objectives of this report are to describe characteristics of patients cared for through Mobile Outreach and to report specific services provided.
Program Description:
Based from a nonprofit, private hospital that serves as the community’s level 1 trauma center and teaching hospital, the Mobile Outreach Program is directed by an orthopedic surgeon with geriatric subspecialization and staffed by a full-time geriatric nurse practitioner. Patients receive care for musculoskeletal concerns and fracture assessments at their nursing care facilities by a Mobile Outreach care provider. Referral for care is from nursing care facilities or as scheduled postoperative follow-up.
Results:
In 2016, the program treated 458 patients (76% female) in the patients’ care settings for a total of 689 visits. The mean age was 81 years (standard deviation = 14; range 25-107). Care of patients included nonoperative fracture care in 100 (22%), postoperative fracture follow-up in 149 (33%), injections for pain management in 184 (40%), and other orthopedic care in 25 (5%). Visits occurred at 88 facilities, mean 7 visits per site (range 1-57).
Conclusions:
Mobile Outreach was implemented to improve postoperative fracture care in the elderly patients. The program also provides on-site nonoperative fracture care and care of frail elderly individuals with chronic musculoskeletal conditions. This report aims to establish the feasibility of a program focused on the provision of appropriate, coordinated care for older fracture patients in their care facility. Level of Evidence: Level V.
Keywords
Introduction
The worldwide incidence of fragility fractures is increasing. 1,2 These injuries are often associated with significant loss of independence and increase in morbidity and mortality. 3 -6 The greatest burden is borne by the oldest population who are not only at greatest risk for fracture but also have the least physiological reserve for recovery.
Approximately 20% to 50% of patients with hip fracture come from nursing homes. 7,8 Ninety percent of patients with hip fracture are discharged from the hospital to postacute care facilities. 9,10 Given the overwhelming number of patients with hip fracture who either temporarily or permanently reside in nursing care facilities, care must be well coordinated throughout the acute and postacute processes. 11,12 In addition, as bundled care reimbursement models are implemented, acute care hospitals and physicians must focus their attention on an integrated acute to postacute model to most efficiently affect fracture recovery. 13
The Mobile Outreach Program is an orthopedic-based program through which on-site musculoskeletal care for individuals in care facilities is provided. Orthopedic services rendered by Mobile Outreach include telephone consultation for initial injury assessment, on-site nonoperative fracture care, joint pain management, postoperative follow-up checks, and coordination of hospital direct-admit processes when injuries and patient circumstances warrant hospital admission and/or surgical treatment. Mobile Outreach is part of a comprehensive elder orthopedic care service, called the “Masters Orthopaedic Program,” which began in 2003 at Regions Hospital in St. Paul, Minnesota. The program is founded upon evidence-based principles for geriatric orthopedic co-management for in-hospital elderly patients with fracture; comprehensive secondary fracture prevention and bone health counseling; and orthopedic service provision at nursing care facilities (Mobile Outreach; Figure 1).
An illustration representing the 3 programmatic foci of the Masters Orthopaedic Program at Regions Hospital, St. Paul, Minnesota. These include an in-hospital geriatric fracture service, an on-site orthopedic clinical service (Mobile Outreach), and a bone health and secondary fracture prevention service. 19
The goal of Mobile Outreach is to provide patient-centered, compassionate care to older individuals who have sustained a fracture or musculoskeletal injury. Given that postoperative, in-clinic visits for elderly patients with fracture may not provide considerable value; transportation for this cohort of patients may be difficult and costly; and most musculoskeletal care can be provided in nursing care facilities (with the assistance of portable X-ray capabilities). 14 Mobile Outreach meets a widely unrecognized and unmet need. The objectives of this report are to detail an innovative care model not previously described in the orthopedic literature, to describe the characteristics of patients who have been cared for through Mobile Outreach from January 1, 2016, through December 31, 2016, and to report specific services provided during this time period.
Program Description
Setting and Target Population
Regions Hospital is nonprofit 527-bed, private hospital in the HealthPartners care network. It is a level 1 trauma center and teaching hospital affiliated with the University of Minnesota. The hospital is located in St. Paul, Minnesota, and is associated with 136 facilities (48 long-term care, 66 assisted living, 10 independent living, and 12 preferred transitional care units) in which HealthPartners Partnering Care Senior Services practitioners provide care. The hospital has an area of operation that includes the 7 counties that surround St. Paul, Minnesota, and also western Wisconsin. It serves an elderly population (65 years and over) of approximately 500 000 within a 50-mile radius.
Patient Engagement
Patients enter the Mobile Outreach care pathway in 1 of 2 ways. First, in-hospital patients with fracture are referred for orthopedic follow-up when they are both discharged to a skilled care facility and identified as vulnerable to challenges with postoperative visits. These challenges include long waits in clinic, consultation when family members might not be present, and the coordination and cost of transportation to and from clinic. Second, existing residents in nursing facilities are referred for musculoskeletal concerns and fracture assessments to Mobile Outreach by their primary care provider.
Program Model and Processes
Based at Regions Hospital, an orthopedic surgeon with geriatric subspecialization directs the program. An in-hospital multidisciplinary team (including representatives from anesthesiology, emergency medicine, hospital medicine, palliative care, perioperative and orthopedic nursing, nutrition, physical therapy, case management, and other medical providers) supports the overall program. In addition to the orthopedic director, resources dedicated to Mobile Outreach at the time of this report included a full-time, dedicated nurse practitioner with geriatric orthopedic specialization.
Mobile Outreach accomplishes its goals of providing the best care possible to frail elderly patients by focusing on 5 components: 24/7 phone consultations with care providers from nursing care facilities On-site (in nursing facility) acute injury visits Procedural visits (cortisone injections for arthritis, splint or cast management for fractures, etc) Postoperative and postfracture treatment visits Facility education and training
Phone consultations
If a geriatrician or primary care nurse practitioner identifies a concern regarding the musculoskeletal health of any patient in a nursing facility, that provider may initiate a call to Mobile Outreach through a dedicated pager. Pager coverage is 24 hours, 7 d/wk. If a resident in a nursing care facility falls, is observed with a musculoskeletal concern such as impaired use of an extremity, or is bearing the stigmata of injury in the form of bruising or swelling, a standard radiograph of the area in question is ordered by the facility staff. Radiographs are obtained on-site through a third-party provider offering portable imaging services. Radiographs are transferred electronically, in an Health Insurance Portability and Accountability Act (HIPAA) compliant manner, to the Mobile Outreach team for review and consultation. When nonoperative intervention is indicated, management is initiated or directed by phone. If operative intervention is required, coordination begins immediately for the direct admission of the patient to Regions Hospital’s orthopedic floor. Emergency department visits, where delays can be long, may thereby be bypassed. 15 Preoperative orders, necessary diagnostic testing, and even scheduling of the operating suite, can occur before the patient arrives at the hospital (Figure 2).

A flow diagram illustrating the communication algorithm utilized by the Mobile Outreach Program.
Acute injury on-site visits
If a care facility resident sustains a musculoskeletal injury or fracture that can be well cared for within that facility (examples include distal radius fracture in a frail patient, minimally displaced proximal humerus fracture, or ankle fracture in a nonambulatory individual), the Mobile Outreach nurse practitioner travels to the facility to provide appropriate definitive care for the injury. Care may include cast, splint, or sling application. Appropriate follow-up and radiographic review can also be undertaken without the patient leaving the care facility. As above, this orthopedic care provision is necessarily supported by the availability of radiographs taken via portable equipment brought to the individual’s room in the nursing facility or assisted living apartment. The potential stress and burden on the patient, afforded by transportation to the hospital or clinic, is thereby eliminated.
Procedural visits
Through the development of collaborative care relationships with primary care providers in many nursing care facilities, the nonemergent orthopedic needs of many nursing residents can also be met through Mobile Outreach. Many care facility residents have degenerative or acute conditions that may require orthopedic attention and intervention. Therefore, the Mobile Outreach nurse practitioner also schedules visits to facilities to provide care, such as cortisone injections for arthritic conditions, on-site splint, brace, or cast management, as well as appropriate osteoporosis or bone health consultation. 16 -18
Postoperative visits
As standard of care, orthopedic surgical patients are seen in clinic at 2, 6, and 12 weeks following their procedures. At these visits, wound checks and rehabilitation evaluations are undertaken. Radiographs are reviewed. The majority of older orthopedic trauma patients treated at Regions Hospital are discharged to a transitional care, skilled nursing, or nursing home facility. Return to clinic for these, often frail, individuals may cause physical, mental, and even financial hardship. Therefore, for those patients unable to easily return to clinic from a postacute care facility, the Mobile Outreach nurse practitioner travels to the care facility to complete postoperative evaluations. Once again, radiographs are preordered and obtained on-site prior to the Mobile Outreach provider visit. This arrangement frees the patient and his or her family from the burden of arranging transportation to the clinic, of waiting to be seen in clinic, and of being transported back to the nursing care facility.
Education and training
Treatment of Mobile Outreach patients within the various nursing care facilities results in an enhanced environment of shared learning and training. The nurse practitioner provides staff training on geriatric orthopedic concerns and best practices through small and large group educational presentations and hands-on skills labs.
Funding and equipment
The Mobile Outreach provider completes both billable and nonbillable encounters. Billable encounters, including E&M visits (CPT 99334-337 and CPT 99348-350), major joint injections (CPT 20610), closed treatment without manipulation (CPT 22XXX-CPT 28XXX), applications of casts and splints (CPT 29XXX), and subsequent care visits (CPT 99307-CPT 310), make up two-thirds of the patient encounters. Post-op follow-up visits (CPT 99024) make up approximately one-third of the Mobile Outreach visits. Although these visits do not generate direct revenues, the benefit of Mobile Outreach extend far beyond the revenue generated by the Mobile Outreach nurse practitioner position and therefore, in our opinion, justify at least some organizational subsidy of such a program.
There are acknowledged inefficiencies when a single provider covers geographically diverse sites, such that the direct revenue generated by the position may not cover the full cost. However, there are many secondary and tertiary cost benefits realized across the organization that far outweigh the gap between position cost and revenue generated. As previously reported, 19 we estimate cost-of-care savings (in 2015 dollars) per encounter as shown in Table 1. Other cost benefits include release of clinic slots for new patients and the utilization of advanced practice providers (APPs or NPs) to offset physician effort. A highlighted financial analysis previously described an annual cost-of-care savings estimate in 2015 of $197 283 for over 300 patients served through 530 encounters. 19
Mobile Outreach Program.
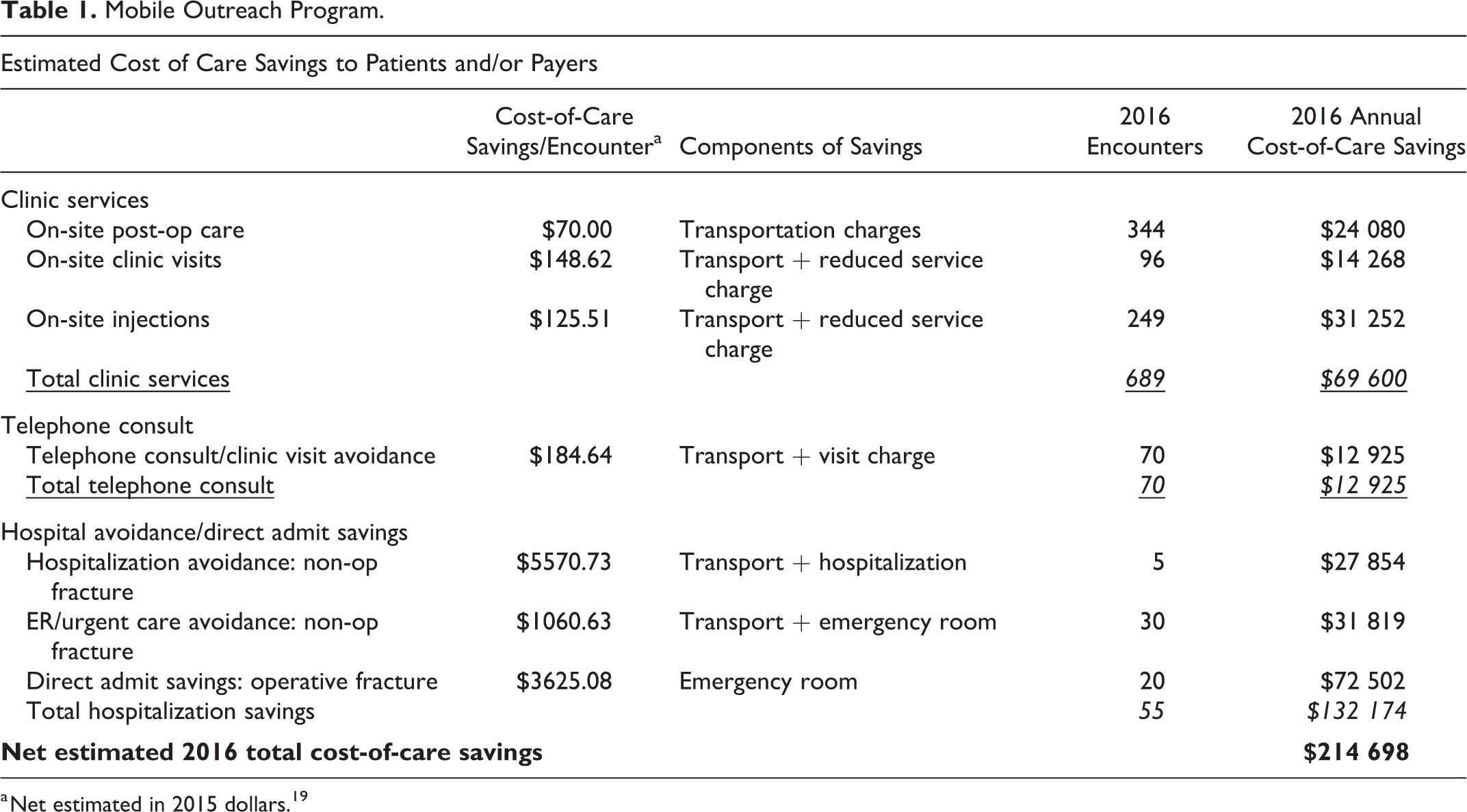
a Net estimated in 2015 dollars. 19
In addition to the financial resources to support such a program, an electronic medical record (EMR) system and access to portable X-rays are cornerstones to a Mobile Outreach Program. Within our program, the Mobile Outreach nurse practitioner utilizes the hospital EMR system (EPIC, Verona, Wisconsin) to input each referral request and to document all clinical encounters. In addition, electronic transfer and digital access through multiple portable radiographic providers allow the Mobile Outreach nurse practitioner to embed into the patient EMR and/or download into picture archiving and communication system (PACS), the X-rays taken at a patient’s residence.
Data Collection and Analysis
A retrospective review of the Mobile Outreach provider and patient records was undertaken for the time period of January 1, 2016, through December 31, 2016. The goals of the review were to determine the number of patient visits and procedures accomplished by a single Mobile Outreach nurse practitioner, the relevant patient demographics, the types of procedures and reasons for patient visits, and the number of facilities (or points of service) visited. Determination was also made whether the visit was the initial encounter with Mobile Outreach or if there were prior encounters for the same patient.
Patient demographics and relevant clinical characteristics were extracted from the EMR by manual review. Analyses and descriptive statistics were accomplished utilizing a simple Excel spreadsheet (Microsoft Inc, Redmond, Washington). The institutional review board was consulted for a determination that this quality reporting initiative did not constitute clinical research and therefore did not require ongoing institutional review board oversight and monitoring.
Results
Between January 1, 2016, and December 31, 2016, the Mobile Outreach program treated 458 patients (76% female) whose point of service was the patient’s care setting (transitional care unit, assisted living, or skilled nursing facility). The mean and median age of patients treated by Mobile Outreach was 81 years and 84 years, respectively (standard deviation = 14 years; range 25-107 years). Thirteen patients (3%), who received Mobile Outreach care were <50 years old. While this cohort would not be considered “geriatric,” their needs (cognitive, medical, physical, and social challenges) were similar to the older population that the Mobile Outreach Program serves. Given these considerations, these patients were also accepted for Mobile Outreach care (Figure 3).
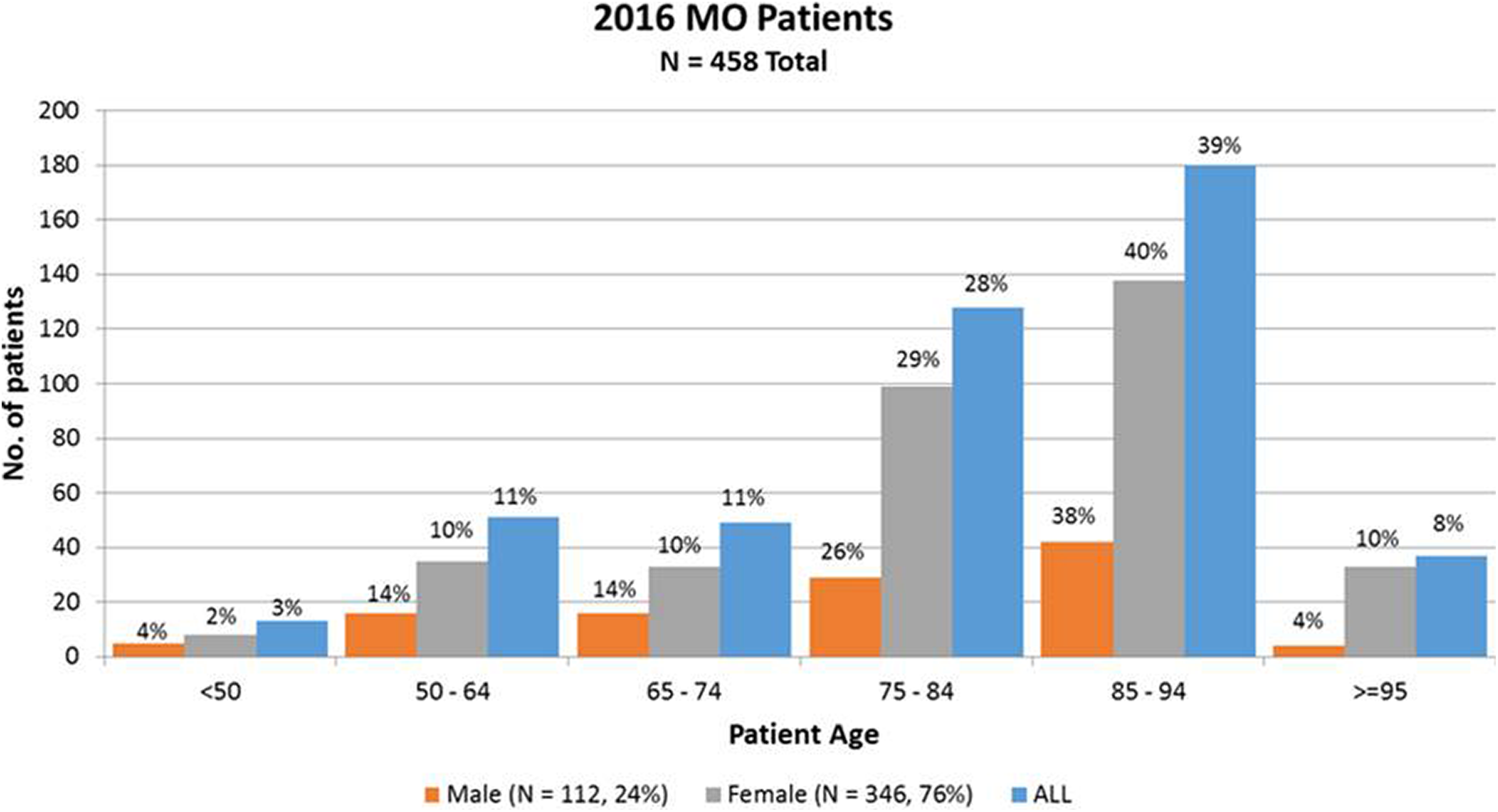
A bar chart illustrating the number of patients in each decade of life treated by the Mobile Outreach Program in 2016. The largest volume of patients fell within 85 to 94 years at the time of care provision. Thirteen (3%) patients, who received Mobile Outreach care were <50 years old and due to receiving trauma care at our institution and having extreme situations of injury, overall morbidity, or personal need, were also accepted for Mobile Outreach care.
The on-site services rendered included first-time visits for nonoperative fracture care in 100 (22%) patients, postoperative fracture follow-up care in 149 (33%) patients, injections for pain management in osteoarthritic conditions in 184 (40%) patients, and other orthopedic injury and postoperative care in 25 (5%) patients. One hundred forty-nine patients (33%) received more than one Mobile Outreach visit in the study period (range 2-7 visits) for a total of 689 care visits completed.
The 689 Mobile Outreach care visits occurred at 88 different care facilities with an average of 7 visits per location (range 1-57 visits per site) and included 6 visits to 4 patient homes. The locations of the various nursing facilities were within a 30-mile radius of the hospital setting where the program is based. Of the 689 visits, 190 (28%) occurred at the “top 5” locations, all having ≥20 visits in 2016 (Figure 4).

A geographical representation of the area of service and Mobile Outreach encounters in the greater St. Paul, Minnesota area. The number of visits to each facility within the 1-year time period of January 1, 2016, through December 31, 2016, are shown.
Of the 458 patients, 161 (79%) receiving care were first-time Mobile Outreach patients during the reviewed 2016 time period. Of these, 149 (33%) of 458 were cared for on 2 or more occasions. The program had previously treated 97 (21%) patients prior to the 2016 study period. Of the 97 patients, 58 (60%) were provided cortisone injections for arthritic joint pain relief, 19 (20%) were seen for nonoperative fracture care and follow-up, 16 (16%) were evaluated for postoperative care (including 1 for total shoulder arthroplasty follow-up), and 4 (4%) were provided care for nonoperative, nonfracture musculoskeletal injuries.
An orthopedic provider from our practice initiated the Mobile Outreach visit in 209 (46%) patients, while the providers at the nursing facility contacted the Mobile Outreach nurse practitioner and requested a consultation in 240 (52%) patients. A Mobile Outreach visit was requested in 9 (2%) patients whose original care was provided for by an outside hospital, but whose follow-up care was requested of the Mobile Outreach program due to patient need or family/patient preferences.
Based upon the type of services rendered by the Mobile Outreach provider, utilizing previously reported estimates for cost-of-care savings to the patient and/or payer, the total net estimated 2016 savings were $214 689 (Table 1). This included $69 600 in transportation savings and reduced service charges (for an APP/NP instead of a physician visit in clinic). Savings for avoided visits altogether, due to telephone consults with geriatrician providers on-site, totaled $12 925. Finally, avoidance of hospital and emergency room fees due to on-site fracture care and direct hospital admission, totaled $132 174. Estimates of transportation savings alone would comprise of $55 580 or 26% of the total $214 689 savings generated in 2016 (Table 1).
Of the 458 patients treated by the Mobile Outreach service in 2016, death occurred in 14% (n = 66) according to the EMR records, at the time of this review.
Discussion
The aging of the population presents considerable challenges for the field of orthopedics. Fragility fracture rates are increasing. 1 Hip fractures, one of the most costly fractures in terms of morbidity and mortality, are expected to double in number in the next 50 years. 20,21 Most studies of elderly patients with fracture have focused attention on advances in perioperative surgical and medical care through integrated geriatric co-management models or fracture liaison services. 7,22,23 These geriatric orthopedic co-management and bone health strategies have been shown to decrease hospital length of stay, decrease surgical complications, improve in-hospital mortality, and facilitate appropriate osteoporosis management. 17,24 Little attention, however, has been focused on the impact of clinical interventions provided outside the hospital setting (and not specifically devoted to bone health), such as during the postacute phase of orthopedic care and beyond. 25 To our knowledge, on-site musculoskeletal care and consult services by geriatric orthopedic providers has not been previously described in any other published model.
An innovative model of orthopedic fracture care called Mobile Outreach has been successfully implemented in our health-care setting. The Mobile Outreach intervention strategy differs from usual orthopedic care and telehealth in orthopedics, 26 in that a geriatric nurse practitioner, also trained in orthopedic care, provides clinical, orthopedic focused care at the patient’s place of residence—nursing home, assisted living, or skilled nursing facility. The preliminary results presented provide evidence of the feasibility and impact that such a program can have in the provision of orthopedic care to the residents of nursing care facilities.
In our urban setting, the Mobile Outreach provider clinic schedule allows for 6 to 8 patient encounters per day. In 2016, through our Mobile Outreach Program, we fielded orthopedic consultation calls from providers at nursing care facilities, saw postoperative patients, facilitated direct admission to the hospital, and accomplished on-site fracture care and joint injections for a total of 458 patients in 689 care visits. Either initial or follow-up fracture care was provided to over 250 patients. One hundred forty-nine of these individuals were postoperative patients. Older patients who had painful musculoskeletal injuries and conditions were spared the disruption of care transition and transport. They could stay in a familiar environment and keep their usual schedule. In other words, in a patient-centered manner, their orthopedic health-care needs were met.
New care models, such as the Mobile Outreach Program, have considerable relevance to orthopedists and especially to those who provide fracture care in elderly patients. The “Triple Aim”—a focus on patient satisfaction, quality of care, and cost—has become a greater focus by health-care organizations, providers, and patients. 17,27 Additionally, although the Center for Medicare and Medicaid Services mandate for the bundled payment of hip fracture care (surgical hip/femur fracture treatment) has been cancelled, efforts to coordinate and decrease the cost of hip fracture care are nearly inevitable. 28 Our report illustrates that the Mobile Outreach Program of orthopedic care for the frail elderly patients at their place of residence is a feasible method of care delivery.
Although, in the primary care field, providing on-site medical care by geriatric nurse practitioners is widely accepted, 29 this approach is novel in the provision of orthopedic care. Also, more recently, Hospital-at-Home (HaH) programs have been trialed for certain limited diagnosis-related groups. 30 -32 Although orthopedic care has not been described specifically, Federman et al reported that HaH bundled in-hospital and postacute care for 19 separate medical conditions resulted in an improvement in clinical outcomes and patient experience. 33
Through the Mobile Outreach program, orthopedic care rendered includes postoperative hip fracture care, which can specifically bring the most appropriate care to this vulnerable patient population. 34 This may reduce postsurgical emergency department visits, readmissions, morbidity, mortality, as well as overall medical care costs. Work is underway to evaluate these potential care process outcomes. This report did not aim to prove the efficacy of the Mobile Outreach service, but instead to provide a foundation to establish its feasibility and to summarize information which may be helpful in the planning of future clinical studies and/or programmatic planning. Further analysis is warranted to appropriately assess the full value of such a program in relationship to improved patient outcomes, cost of care, and patient experience.
Footnotes
Acknowledgments
The authors would like to acknowledge Jeanne Dutkowski, J. Noel, Veronica Carson, David Wright, Donna Marko, and Ryan Larson, without whom this line of service could not have been developed and the report would not be possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.