
Abstract
Introduction:
Older patients with hip fracture have a 20% to 30% mortality rate in the year after surgery. Nonoperative care has higher 1-year mortality rates and is generally only pursued in those with an extraordinarily high surgical risk. As the population ages, more patients with hip fracture may fall into this category. The orthopedic surgeon is typically the main consultant responsible for deciding between surgery and conservative management, and the reasoning behind one decision over the other is often poorly understood. We undertook a review to determine decision-making tools for surgery in high-risk patients with hip fracture.
Materials and Methods:
A review was conducted using PubMed to determine articles published using the terms palliative care, conservative care, nonoperative, hip fracture, orthopedic procedures, fracture fixation, and surgery. Our search resulted in 13 articles to review. These were further screened to determine tools for use in surgical decision-making.
Results:
Several potential decision-making tools were found in our search. The potential tools to identify patients who would benefit from nonoperative treatment included the Palliative Performance Scale for severe dementia, the Lawton Instrumental Activities of Daily Living and Katz Activities of Daily Living scales for prefracture immobility, a combination of clinical signs and laboratory tests to determine risk of imminent death, and the Charlson Comorbidity Score for additional serious comorbidities. No tools have been prospectively tested in a clinical setting.
Discussion:
Evaluation of each patient using a variety of decision making tools should help the orthopedic surgeon determine which patients would be better suited to non-operative management. After determining the benefit of non-operative care, they must effectively allow the fracture to heal while ameliorating pain. Palliative care physicians can fulfill this role by providing support and symptom relief.
Conclusions:
Surgical decision-making for hip fracture repair in the elderly patients is not straight forward. Several tools may be helpful to the surgeon in determining who may be better suited for nonoperative care or a palliative care referral. Prospective data do not exist in these decision-making tools.
Introduction
As the population ages, the number of hip fractures that must be managed are expected to rise by 11.9%. As the numbers increase so will time spent in the hospital, mortality rates, and costs of care. 1 Hip fractures are treated mostly by surgical repair, with only about 10% treated nonoperatively. 2 Regardless of the method of treatment, the goal of hip fracture repair is to return the patient to their prefracture functional abilities. However, individuals who have had a hip fracture have significantly higher mortality rates than those without fracture, and within the fracture sustaining group, there are subsets of patients who are even at greater risk of mortality. 3 This vulnerable group of patients is less likely to regain functionality and has high risks and low rewards associated with surgery.
Nonoperative management may be more beneficial to these patients, ensuring quality of life remains closer to a prefracture level. Additionally, nonoperative management may decrease costs associated with direct surgical intervention or postoperative complications. 4 However, nonoperative management of hip fractures has its own set of complications. Nonoperative treatment requires a longer time frame than surgical management but can be as effective when treating patients with fractures and pain. 5,6
Making the decision to pursue nonoperative care is not an easy task. There is always the need to weigh the patients’ surgical mortality risk versus the chance of regaining function and reducing pain. This article seeks to understand some of the variables that should be considered in when deciding on surgical treatment of hip fractures and on the need for palliative care consultation.
Materials and Methods
A literature search was conducted using Medline through PubMed to look for all relevant articles discussing the use of nonoperative management when compared to surgery in patients with hip fracture between 1985 and 2016. Search terms included: palliative care, conservative care, non-operative, hip fracture, orthopedic procedures, fracture fixation, and surgery (see Figure 1 for search strategy). The search returned 374 articles and was narrowed using English language and aged 65+ years as limits, leaving 142 articles. Articles were hand searched for relevance to hip fractures in the elderly patients, patient postoperative outcomes, pre- and postoperative mortality risks, and the role of different medical specialties in the treatment of fractures. Articles were first screened by title and abstract and then by full text. Specific terminology included in hand searching were nonoperative hip fracture, conservative management of hip fracture, nonoperative management of hip fracture, differences in mortality conservative versus operative, and care planning. Exclusion criteria included articles primarily covering surgical management, fractures in areas other than the hip, or fractures in the pediatric or adult populations. Articles were also excluded if surgical fixation was provided before palliative care, an amputation was performed, or in cases of malignancy.
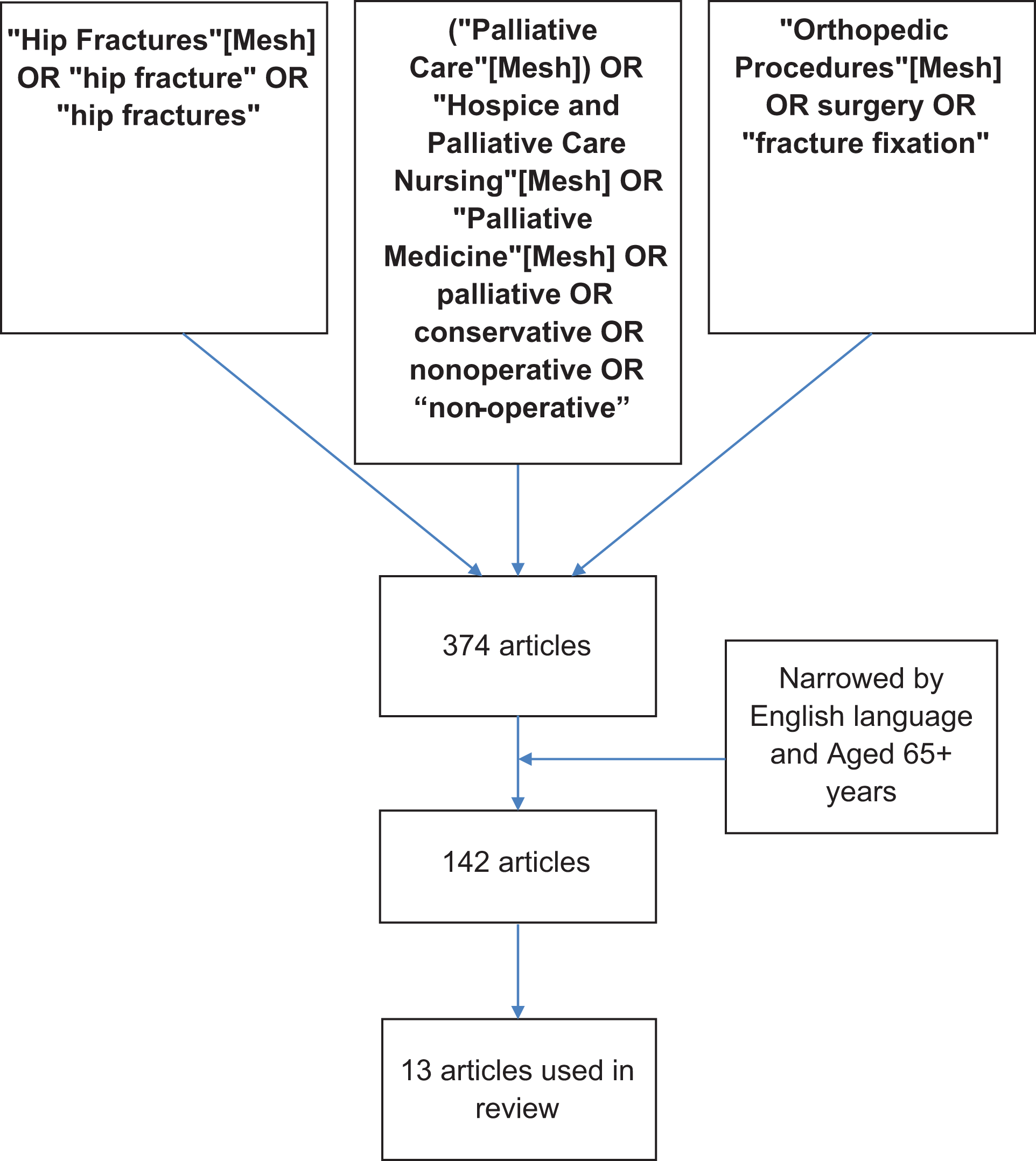
Article search strategy.
Results
Our search found 13 articles that dealt with decision-making for nonoperative treatment (Table 1). A review of the articles discussing nonoperative treatment of hip fractures found that patients with severe dementia, prefracture immobility, those who are imminently dying, and those with serious comorbidities such as severe heart failure, pulmonary, or kidney disease are most likely to benefit from nonoperative care. 7 Patients treated with nonoperative care had no significant difference in the 1-year mortality rate compared to those undergoing surgery. Review of articles discussing palliative care in a surgical setting found that certain criteria can be useful in determining which patients would benefit from early consultation with palliative care. In the specific setting of hip fracture among the frail and elderly patients, it was found that early palliation can lead to better quality of life as well as superior management of their numerous comorbidities. The articles used several tools to potentially identify patients who would benefit from nonoperative treatment. These are based on dementia, preoperative function, and signs of imminent death.
Summary of Articles Discussing Nonoperative Care.

Abbreviations: N/A, not available; ASA, American Society of Anesthesiologists.
Dementia
Dementia is seen in 6.4% of the elderly population, but the prevalence among the elderly patients who sustain hip fractures is typically greater, between 18.7% and 47.2%. 8,9 Patients with dementia often present challenges for physicians, particularly surgeons, due to the unique progression of the disease and the postsurgical risks it presents. These risks include increased risk of further cognitive impairment, drug–drug interactions, anesthetic complications, development of delirium, and loss of ambulatory ability. 10 Multiple studies have shown that cognitive decline after surgery is more frequently seen in elderly patients who already exhibit some form of cognitive impairment. 11,12 In patients with severe dementia, the fact that the risk of anesthesia negatively impacts their cognitive function is appreciable. Prefracture cognitive impairment is also a substantial risk factor for the development of delirium, while late-stage muscle contractures can make surgery more complicated. 13,14 Evidence has shown that surgical intervention increases the risk of altered mental status, so the surgeon should determine which patients are at high risk of further decline and manage their fractures accordingly. 15
Dementia is measured by several scales of varying levels of length, most of which can act as a prognostic indicator of 6-month mortality. 16 These include the Mini Mental Score (MMSE), the clinical dementia rating (CDR), and the Reisburg Functional Assessment Staging (FAST) Scale among others. Am MMSE score of 0 to 10, a CDR rating of 3, or a FAST score of 7 correlate with severe dementia. Over 50% of patients with this severity level of dementia die within 6 months. 17
Prefracture Ambulation
The prefracture ambulatory ability of a patient should be taken into account when considering operative versus nonoperative treatment. Prefracture functionality can be calculated using the Instrumental Activities of Daily Living (IADL) and Activities of Daily Living (ADL) scales. These scales provide a detailed picture of a patient’s mobility prior to fracture by asking questions about activities such as bathing, feeding, and dressing oneself (ADL) or about activities such as using the telephone, shopping, housekeeping, and being responsible for taking medications (IADL). Both scales take into account the amount of independence a patient has in doing these activities. Lower scores are associated with greater functional ability. 18 In many cases, hip fracture management focuses on returning patients to their previous functional abilities. Although surgical management can also be used for pain relief and symptomatic management, a patient who is immobile prior to surgery is unlikely to regain any functional abilities after surgery. Therefore, it is important to weigh the benefits of surgery on pain and regained functionality against the risks prior to making a decision. Patients with lower prefracture scores on these scales were shown to be 18 times more likely to fail to regain basic mobility during hospitalization, while patients who were nonambulatory or housebound had worse postoperative outcomes. 19 -21
The prefracture ambulatory ability of a patient can be used by the orthopedic surgeon as an indirect measurement of the benefit of any surgical intervention. A mobility score, in combination with good clinical judgement, could determine which patients would have improved function after surgery. Surgery introduces postoperative risks that are otherwise unlikely to occur, such as infection and the need for repeated surgery, so that in patients with low mobility scores, nonoperative treatment and careful pain management can be used to decrease these risks while ensuring the patient’s quality of life remains consistent. 22
Imminent Death
Many patients who present with a hip fracture fall while in a nursing home or hospice care. 23 Of those patients, it can be expected that a number of them are either in the preactive or in active stages of dying. In these patients, it is important to consider whether surgery would benefit them at all.
There are observable signs that can be associated with imminent death (Table 2). Marked decreases in consciousness, Cheyne-Stokes breathing, decreased performance status, apnea, and decreased urinary output are used to predict that the patient will die within the next 3 days. 24,25 Additionally, Loekito et al found that abnormal test results for urea, pH, white cell counts, creatinine, albumin, total bicarbonate, and bilirubin measures are also useful in predicting imminent death. 26 Values on these tests outside the normal range, coupled with clinical observations, can be used to accurately predict patients who are likely to be undergoing imminent death. Recognizing patients with hip fracture who are imminently dying is important for the orthopedic surgeon. Surgery has the potential to exacerbate the disease process in these patients, and nonoperative treatment should be chosen in these circumstances.
Signs of Imminent Death.

Surgical Risk and Palliative Care Decision-Making
Scores have been developed to determine surgical risk after hip fracture. The Nottingham Hip Fracture Score was initially developed to stratify risk and has been subsequently modified to better include the effects of cognition. 27 Further modifications have led to the Almelo Hip Fracture Score (AHFS), which has been used to place patients at low, medium, or high risk for mortality. Factors included in the AHFS are age, gender, hemoglobin, cognitive frailty, institutional living, comorbidities, malignancy, Parker Mobility score, and American Society of Anesthesiologists score. 28
The Palliative Performance Scale (PPS) is used to estimate the burden of disease an individual possesses based on categories such as ambulation, activity level, self-care ability, nutritional intake, and consciousness. It has specific guidelines to follow in order to calculate the PPS level, and the distinctions may be easier to separate out. The PPS has been used to determine mortality in older patients with polytrauma. A score of <80 had significant correlation with mortality and poor outcomes. 29 However, it has not been used in a prospective study to promote automatic palliative care consultation in these high-risk patients. The PPS provides the orthopedic surgeon with a potential score to estimate the risk of further mental decline in a patient prior to surgery.
Discussion
Hip fractures occur in elderly patients with high mortality who may be at the end of life. It is important for orthopedic surgeons to recognize patients who would benefit from nonoperative treatment. Recognizing these patients leads to a personalized approach and hopefully appropriate selection of patients who will not benefit from operative care. Although nonoperative treatment has its own risks, evaluation of each patient using a variety of decision-making tools should help the orthopedic surgeon determine which patients would be better suited to nonoperative management. Our review of the literature has shown that no prospectively validated score has been used in surgical or palliative care decision-making in the population with hip fracture. Several different types of scoring systems may be helpful. These tools include measurements of dementia, preoperative ambulation, and signs of imminent death. Patients with FAST stage 7 dementia are both nonresponsive and at higher risk during surgery; they may not benefit from surgical intervention. Patients with very poor levels of preoperative function may also be better suited to nonoperative care. The use of specific scores to evaluate patients with hip fracture, such as the AHFS or the PPS, may be very useful to the clinician to help evaluate patients at extremely high risk of surgery. It may also allow patients and their families to be more involved in the decision-making process and to help them set reasonable expectations and goals of care. Prospective study of these scores to help in decision-making is needed. The use of hip fracture co-management may help with the implementation of routine referral to palliative care in appropriate patients.
Once a patient is determined to benefit from nonoperative care, the challenge becomes effective allowing the fracture to heal while ameliorating pain. Techniques such as bed rest and early mobilization are effective strategies for nonoperative treatment, but they are often associated with a longer and more painful recovery, indicating the need for close follow-up to ensure the patient is treated appropriately. 2 Palliative care physicians are in a unique position to reduce suffering associated with nonoperative management of hip fractures, as they are specially trained to provide symptom relief, whether it is physical or emotional. 30,31
The primary goal of palliative care is to work with the patient through each step of their disease in order to prevent suffering, manage pain, provide relief of symptoms, coordinate planning of care, and provide direct communication with the patient and the family. 32 Their involvement in the care of hip fractures is a reasonable consideration, because much like severe end-stage disease, fragility fractures of the hip can pose a high risk to quality of life. Palliative physicians work regularly to manage end-stage disease and have significant experience with serious comorbidities and dementia. 30 As such, they are able to address functional and cognitive disabilities that elderly patients often have prior to their fracture or following treatment. 33
Palliative care is often used to provide support for patients and families both during the decision-making process and after the role of the surgeon has been fulfilled. Palliative care physicians can explain the outcomes that can be expected with each treatment and help patients choose the most advantageous treatment option based on their goals of care. Currently, there are no guidelines in place for the orthopedic surgeon to follow concerning when to decide on nonoperative care and call palliative medicine. However, a good place to start is for the orthopedic surgeon to be able to recognize the patients who would benefit more from nonoperative management then surgical. Once these patients are identified, the surgeon can consider whether involving palliative care physicians is the right choice.
Conclusions
As the incidence of hip fracture increases due to increases in the very old patient population, it is important to consider areas in which care can be improved. Nonoperative treatment may be optimal for patients who are unlikely to benefit from surgery. In nonoperative cases, involving a palliative care doctor can provide a more comprehensive treatment plan, leading to better patient care. By looking at factors such as cognitive status, various measures of prefracture ambulation, and especially signs of imminent death upon a patients’ admission to the hospital, it may be possible to better identify at-risk patients early and significantly improve our selection of which patients potentially receive nonoperative care. Prospective use of the AFHS or the PPS may provide us with more information to make better informed decisions about the use of operative or palliative care for the very ill patients with hip fracture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.