
Abstract
Background
There is ongoing debate regarding the optimal management of older adult ankle fractures. The purpose of this study was to describe baseline characteristics and functional outcomes including complications in older adult patients receiving nonoperative treatment for low-energy ankle fracture and compare the outcomes of those with unstable vs stable fracture patterns.
Methods
Patients aged ≥65 from January 2012 to March 2019 that sustained an ankle fracture were identified. Those who had surgical treatment, age <65, high-energy trauma, bilateral ankle fractures, and patients without adequate follow-up (minimum 12 weeks) were excluded. Baseline demographics, injury characteristics, Charlson Comorbidity Index (CCI) score, and functioning regarding ambulatory status, living environment, and assistance personnel in the household were collected for all patients. The primary outcome of interest was retention of baseline ambulation, living environment, and assistance requirements at follow-up (>12 weeks). Pain improvement, radiographic changes, and adverse clinical events were also assessed.
Results
A total of 158 patients were included with an average follow-up timeframe of 41.6 weeks. Eighty-six percent of patients (n = 136) retained their ambulatory status at long-term follow up. Most patients retained the same living environment (n = 145, 91.8%). Thirty-five patients (22.2%) required additional assistance long-term. Approximately 67.1% of the entire cohort retained all three functional metrics. Patients who experienced functional decline were older (77.8 vs 71.6, P < 0.001), had higher CCI (3.2 vs 1.6, P < 0.001), had a diagnosis of dementia or cognitive impairment (36.5% vs 3.8%, P < 0.001), had lower baseline functional status (ambulation, living environment, and assistance required; all P < 0.001), and had an unstable fracture pattern (P = 0.003).
Conclusions
Understanding the functional outcomes of non-operative treatment in geriatric ankle fracture cases can contribute to a shared decision-making among healthcare providers, patients, and families.
Introduction
Within the aging population, older adult ankle fractures are becoming increasingly common. 1 Ankle fractures rank as the third most common orthopedic fracture in older adults, and the number is expected to rise in the future.1-4 Older patients have disproportionately poor outcomes, and their quality of life can suffer as they lose mobility.4-6 Due to the varied physiological conditions observed in the geriatric population, determining the optimal treatment for ankle fractures in this demographic remains a challenge. 7
Physicians consider several factors when discussing between nonoperative treatment and operative intervention for older adult patients. These factors include age, comorbidities, baseline functional status, fracture pattern, and functional goals.4,8-12 Some ankle fractures, even with unstable morphology, are treated conservatively in older adults for various reasons such as medical comorbidities, baseline ambulatory status, and patients’ goal. The primary goal in treating ankle fractures in older adult patients is to restore health-related quality of life and to avoid treatment complications and immobility. 4 Non operative treatment is sometimes chosen for geriatric patients with ankle fracture, however, there is still a limited understanding of the functional outcomes. The primary objective of this study is to examine the functional outcomes of older adult patients with ankle fractures who underwent nonoperative treatment, with a particular emphasis on ambulatory status, living environment, and assistance personnel. Secondary aim includes identifying characteristics associated with unfavorable functional outcomes.
Materials and Methods
This retrospective cohort study was conducted within a United States metropolitan healthcare system. This study was approved by the Health Partners institutional review board in March 2022 prior to data collection. All research was carried out according to the Declaration of Helsinki. Patient consent was not required for this retrospective review. The study included older adult patients (age 65 and older) who sustained a single low-energy ankle fracture and received nonoperative treatment. Patients who underwent surgical treatment within 6 weeks after the injury, were under 65 years of age, experienced high-energy trauma, had bilateral ankle fractures, or lacked at least 12 weeks of follow-up were excluded. Encounters from January 2012 to March 2019 were identified using codes from the 10th edition of the International Classification of Diseases (ICD-10) in three centers. The primary diagnosis of these encounters was an ankle fracture or fracture of the distal tibia or fibula.
Variables Included
Patient demographic, injury type, medical comorbidities, and baseline functional characteristics were collected from the electronic medical record (EMR). Charlson comorbidity index for each patient was calculated using medical history extracted from the EMR as described in previous literature. 13 Based on radiographic findings, fractures were divided by stability of the fracture pattern. Fractures considered stable included isolated avulsion fractures, Weber A fractures, Weber B fractures that did not exhibit syndesmotic or medial space widening on stress or gravity view, and isolated medial or posterior malleolar fractures that involved <25% of the malleolus and had displacement <2 mm that did not exhibit syndesmotic or medial space widening on stress or gravity view. 14 Fractures considered unstable included Weber B which exhibited syndesmotic or medial space widening on Mortise or stress view, Weber C fractures, bimalleolar or bimalleolar-equivalent fractures, trimalleolar fractures, and Maissoneuve fractures.15,16 Fractures that did not fall into either unstable or stable classification or required radiographs for appropriate classification were included in whole-cohort analyses, but excluded for comparative analyses of cohorts.
Functional outcomes (ambulation status, living environment, or assistance requirements) at final follow-up were collected and categorized. Adverse clinical outcomes such as complications, emergency department (ED) visits, admissions/readmissions, subsequent need of operations, and death within 1 year of injury were recorded.
Statistical Analysis
Statistical analysis was performed using Intellectus Statistics (Clearwater, FL). Data were presented using counts and frequencies for categorical variables and means and standard deviations for continuous variables. Factors associated with functional outcomes were compared between patients who retained functional status on all metrics and those who declined functionally for any 1 metric. Characteristics and outcomes of patients with unstable fractures were described and compared to the overall cohort via one-sample t-tests (continuous variables) and one-proportion z-tests, Chi-square tests, or Fisher exact tests (categorical variables). Statistical significance was set at P = 0.05 (two-tailed).
Results
Functional and Clinical Outcomes
Baseline Demographics and Functional Status (N = 158).

Categorical data presented as n (%). Scale data presented as mean ± S. D.
Injury Characteristics and Weight-Bearing (N = 158).

Categorical data presented as n (%). Scale data presented as mean ± S. D.
Outcomes After Nonoperative Ankle Fracture Treatment (n = 158).
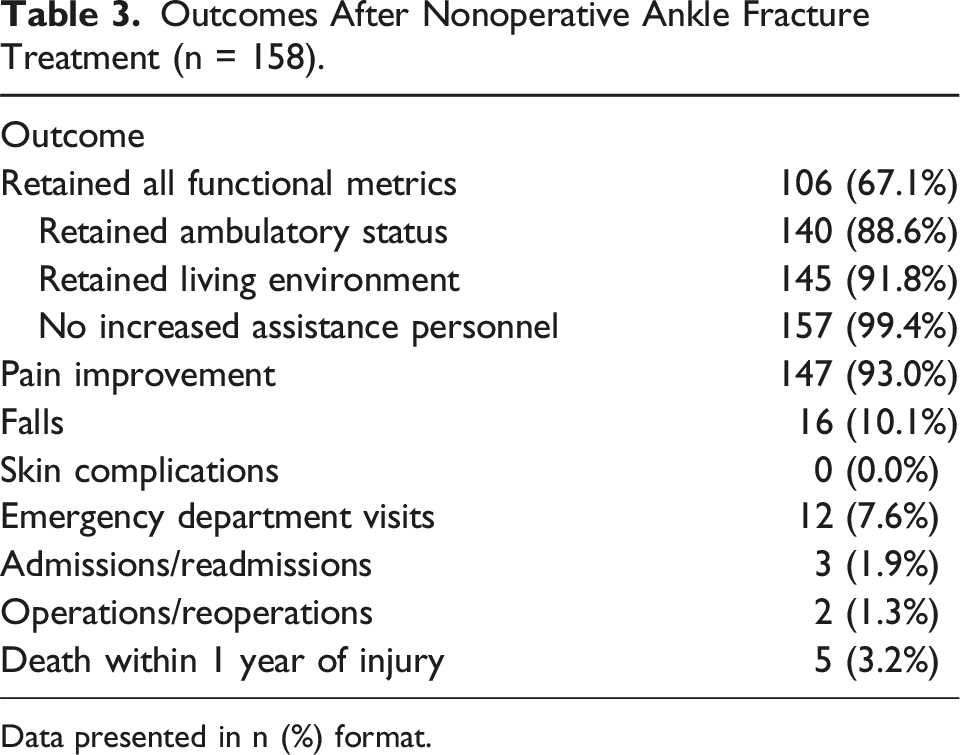
Data presented in n (%) format.

Non-weightbearing initial injury (left) and 12-week follow-up (right) radiographs for patient that underwent nonoperative management of an ankle fracture.
Comparison of Stable and Unstable Fracture Pattern Patients
Baseline Characteristics and Weightbearing Status of Patients With Unstable and Stable Fractures (N = 141).

*One-sample t-tests were conducted for continuous variables. One-proportion z-tests, Chi-square, and Fisher exact tests were conducted for categorical variables as appropriate. Bold text indicates statistical significance. Significance set at P = 0.05.
aDOI = Date of injury.
bNWB = non-weightbearing.
cPWB = partial weightbearing.
dWBAT = weightbearing as tolerated.
Outcomes for Unstable Ankle Fractures After Nonoperative Treatment.

Bolded text indicates statistically significant difference between stable and unstable cohort at that follow‐up timepoint for that specific variable. Significance set at p ≤ 0.05
Discussion
Open reduction and internal fixation (ORIF) normally leads to fair postoperative results in young patients with an ankle fracture and is therefore widely accepted. However, optimal treatment for geriatric patients remains controversial due to the complexity including medical comorbidities, different baseline functional status, and various treatment goals.
Patients’ Characteristics
The present study described the characteristics of patients who underwent non-operative treatment. Factors such as female gender, advanced age, and a high CCI have been reported to associate with a higher likelihood of nonoperative management.18,19 Those who with unstable ankle fracture patterns were less functional regarding ambulation and baseline living environment as well as having higher rates of diagnosed dementia at baseline. However, more than 85% of patients with unstable fracture patterns were independent ambulators or independent with assistive device as baseline, and 69.4% lived independently at home at baseline. It is understandable that patients with unstable fractures who underwent nonoperative treatment were generally less healthy. However, it was surprising that many were still independent ambulators prior to opting for nonoperative management.
Functional Outcomes
Regarding the functional outcomes, the previous studies showed inconsistent results in geriatric patients. Our study demonstrates maintenance of ambulatory status in 89% of patients treated nonoperatively with no significant difference in ambulatory status change between patients with stable and unstable fracture patterns at an average follow-up of 42 weeks. In a study performed by Lorente et al, a group of geriatric patients with Weber B fractures treated nonoperatively were prescribed early weightbearing with functional outcomes up to two years post-injury. Patients assigned to the early weightbearing cohort saw greater improvement in functionality as measured by the Barthel Index and the Short Form 12 questionnaire. 20 Ahearn et al reported operative patients ultimately returned to their baseline mobility measured by the life space assessment (LSA) at 1 year while nonoperative patients did not. 21 Another prospective randomized study of 36 patients with mean 27-month follow-up found higher Olerud scores for ankles undergoing ORIF vs those treated nonoperatively. 22 In contrast, a systematic review and meta-analysis including eight prospective randomized controlled studies provides equal results for conservative and surgical treatment in ankle fractures. 23 One study randomized 84 patients aged ≥65 to either nonoperative or operative management and demonstrated better American Orthopedic Foot and Ankle Score (AOFAS) for patients undergoing nonoperative treatment (91 vs 75, P = 0.001), concluding that consideration should be given to nonoperative treatment for well-reduced ankle fractures. 24
We identified factors associated with higher likelihood of functional decline, including older age, higher CCI score, diagnosis of dementia, lower overall functional baseline, and fracture instability. This result is concordant with previous studies. One of the aforementioned studies found that age ≥80, poor surgical reduction, two or more comorbidities, female sex, and Weber type C fractures were predictors of loss of autonomy after ankle fracture in older adult patients that underwent surgical treatment. 25 Our identification of factors associated with functional decline in nonoperative ankle fracture patients adds valuable insights to clinical decision-making. Patients with these characteristics thus need closer follow-up or a higher degree of care following an ankle fracture.
While fewer patients experienced functional preservation with unstable fractures, it is noteworthy that approximately half of these patients did not experience a functional decline in the measured three metrics after nonoperative treatment. Over 80% of the patients with unstable fractures in the present study retained their ambulatory status and living environment. A recent randomized controlled trial of 620 patients aged ≥60 with unstable ankle fractures revealed equivalent Olerud-Molander Ankle Score (OMAS), Timed Up and Go test mobility, quality of life, pain, ankle motion, and patient satisfaction between operative and nonoperative treatment, although 19% of nonoperative patients received later surgery. 26 Unstable fractures are typically treated operatively but the results of this study in conjunction with prior studies6,26 that evaluated unstable fractures specifically suggest that nonoperative treatment for these types of fractures is an option for selected patients.
Mortality
It is previously reported that non-operative patients have a higher mortality compared to operative patients after an ankle fracture. Koval et al. reported on mortality and complications for 33,704 older adult patients, revealing higher mortality rates in nonoperative patients and higher rehospitalization rates in operative patients. 18 Bariteau et al. reported 22% of one-year mortality among geriatric ankle fracture patients with a nonoperative treatment. 8 The one-year mortality of the present study was 3.2%, which was much lower compared to other studies. The reason is unclear but could be the result of a healthier population, advances in medical treatment and support, or the exclusion of high-energy injuries among others. Nonetheless, the 1-year mortality rate of less than 4% suggested that nonoperative management was not associated with an immediate risk of death.
Strengths and Limitations
One limitation was the inability to determine the impact of early fracture displacement on the management and outcomes of ankle fractures. The study's methodology may have excluded the patients who initially underwent nonoperative treatment but later required operative fixation within 6 weeks due to fracture displacement. An additional limitation is the lack of prospective power analysis for sample size calculation. The primary objective of the study was to describe the functional outcomes for nonoperative treatment, thus excluding early surgical interventions. Furthermore, the study's focus on nonoperative patients aged 65 or older in a specific metropolitan area in the United States limits its generalizability to a broader population. Despite these limitations, the study was able to provide a comprehensive description of the characteristics and functional outcomes of older patients who underwent non-operative treatment after low-energy ankle fractures. This information is valuable to patients, their families, and healthcare providers seeking insights into the management of such fractures.
Conclusion
Due to the varied physiological conditions observed in the geriatric population, determining the optimal treatment for ankle fractures in this demographic remains a challenge. Understanding the functional outcomes of non-operative treatment in geriatric ankle fracture cases can contribute to informed decision-making among healthcare providers, patients, and families.
Footnotes
Author Contributions
RMK contributed to data collection, analysis and validation, manuscript composition and final manuscript revision. FAH contributed to study conceptualization, data collection, analysis and validation, manuscript composition, and final manuscript revision approval. BRA contributed to study conceptualization, data collection, manuscript composition and final revision approval. AS, JA, and LQ contributed to study conceptualization, data collection and analysis, manuscript editing and final revision approval. JAS contributed to study conceptualization, data curation and validation, manuscript editing, and final manuscript revision approval. NO contributed to study conceptualization, data validation, manuscript composition, manuscript final revision and supervision.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Switzer is committee member for AAOS and AOA. She is also on the editorial board for GOS&R, and a committee member for IGFS. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.