
Abstract
Background:
Subsidence of cementless femoral stems in hemiarthroplasty (HA) and increased fracture rates are ongoing concerns of orthopedic surgeons when treating fractures in very old patients. Additionally, bone cement implantation syndrome may result in perioperative cardiac or pulmonary complications, especially in older patients, leading to morbidity and mortality. This study was performed to analyze possible subsidence and intraoperative fractures in a cohort of very old patients treated with cementless stems.
Methods:
We retrospectively analyzed a consecutive cohort of patients aged ≥90 years with femoral neck fractures treated by uncemented HA and an anterior minimally invasive approach. Immediate full-weight bearing was allowed postoperatively. Pelvic radiographs were examined for subsidence immediately postoperatively and 6 weeks later.
Results:
We treated 109 patients (74% women; mean age, 93 years; range, 90-102 years) by HA from January 2010 to March 2016. The 30-day mortality rate was 16%, and the morbidity rate was 47%. There were 11 (12%) intraoperative fractures: 8 (Vancouver B2) had to be addressed immediately during the primary operation, while 3 (1 Vancouver B1 and 2 Vancouver AG) were treated conservatively. One periprosthetic femoral fracture (Vancouver B1) was documented during follow-up. In 17 patients, subsidence of >2.0 mm (median, 3.9 mm; range, 2.5-9.0 mm) was documented.
Conclusion:
Early subsidence was low in this very old cohort treated with an uncemented stem and not showing a periprosthetic fracture. The risk of intraoperative periprosthetic fractures was high. The use of uncemented implants in osteoporotic bone continues to be an intervention with high risk and should only be performed by experienced surgeons.
Level of Evidence:
Level III, Therapeutic study.
Keywords
Introduction
Femoral neck fractures are common injuries in elderly patients and occur at a mean age of 81 years. 1 Svedbom et al reported that the incidence of hip fractures in Switzerland was 17 to 35 per 100 000 person-years among people aged 50 to 54 years and 2937 to 1394 per 100 000 person-years among those aged ≥85 years. An estimated 13 834 traumatic hip fractures occurred in Switzerland in 2010. 2 As the population ages, the incidence of these fractures is expected to increase to almost 3 million worldwide per year by 2025. 3 Patients at the extreme of old age with femoral neck fractures represent a challenging subgroup. Because of their higher numbers of comorbidities, they are thought to have poorer outcomes and a higher risk of systemic and local complications. Although the necessity of operative treatment by hemiarthroplasty (HA) or total hip arthroplasty for displaced femoral neck fractures is well established, whether the prosthesis should be cemented remains controversial. 4,5 Some retrospective studies have supported the use of a cemented prosthesis for the treatment of femoral neck fractures in elderly patients, the claimed advantages being minimal thigh pain, better mobility, 6,7 and a lower frequency of prosthetic dislocation. 8,9 Other studies favoring uncemented prostheses have revealed a shorter operative time, less blood loss, 10,11 and a lower or similar perioperative mortality rate. 12 –16 However, the use of cement leads to a longer duration of surgery, 6,17 complicated revision surgery, 18 and possible bone cement implantation syndrome (BCIS). 19 Up to 28% of patients develop BCIS, which is known to be responsible for intraoperative cardiac or pulmonary complications especially in the elderly. The BCIS is graded from 1 to 3 by increasing severity and is characterized by an increase in hypoxia and hypotension that leads to cardiovascular collapse requiring cardiopulmonary resuscitation in grade 3. 19 Grade 3 BCIS is associated with a high perioperative mortality rate of up to 88% and is responsible for intraoperative death during cementing in 0.11% of patients. 20
Early discharge, relatively fast functional recovery, and independence in activities of daily living are important goals of joint recovery programs. In elderly patients, these goals can be reached more easily if immediate postoperative unrestricted weight bearing can be allowed after arthroplasty. 21 Therefore, it is important that patients with uncemented stems can also undergo immediate unrestricted weight bearing. Early migration of prostheses is known to predict later loosening and implant failure. 22,23 Van der Voort et al 24 defined the threshold for acceptable migration as 0.15 mm in 2 years. Their revision rate was <5% at 10 years, while stems exceeding 0.15 mm of subsidence had revision rates of >5%.
After having obtained very convincing results using uncemented implants, including immediate full weight bearing, we now use this standard for all patients independent of their age or comorbidities. The purpose of this study was to determine whether early subsidence occurs when using uncemented femoral stems in a population of very old patients. We also analyzed intraoperative and perioperative fractures and complications that occurred while using uncemented stems in this high-risk population.
Patients and Methods
Study Design
This retrospective analysis was conducted in our department of geriatric traumatology and orthopedic surgery. From January 2010 to March 2016, all patients aged ≥90 years with a femoral neck fracture (Garden type II-IV) 25 treated with HA were considered for inclusion. After confirming the proximal femoral fracture by conventional radiography, uncemented monopolar arthroplasty was planned. The preoperative exclusion criterion was a Dorr type C proximal femur 26 (Figure 1), for which the use of a cemented femoral stem was planned. Two patients with recent trauma had already undergone osteosynthesis at the proximal femur and were therefore excluded. No further exclusion criteria concerning additional diagnoses, medications, or medical history were applied. The institutional review board and the local ethical committee approved the study protocol, BASEC-Nr. 2016-00577.

A, Example of a Dorr type C proximal femur. B, Primary cemented hemiarthroplasty.
Surgical Procedure
After initializing either spinal or general anesthesia and positioning the patient on a special extension operating table, the surgeon used the modified Hueter approach 27 (anterior minimally invasive surgery approach). All patients were treated with a titanium–niobium standard Quadra-H stem (Medacta International, Castel San Pietro, Switzerland) with hydroxyapatite coating. Preoperative planning using an orthopedic measuring program (MediCAD; Hectec, Altfraunhofen, Germany) was conducted by the surgeon. Following implantation, the operation site was flushed and the joint reduced. In case of intraoperative periprosthetic fracture, the cerclages (wire/band) in the calcar region were performed using the same minimal invasive approach. A drainage tube was placed and the soft tissue and skin were closed.
Postoperative Treatment
All patients were mobilized and allowed full weight bearing on postoperative day 1. This was performed under the instruction of the physiotherapist. To prevent deep vein thrombosis, therapy with enoxaparin was initialized postoperatively and continued for 6 weeks. An anteroposterior plain radiograph of the pelvis was taken after the first postoperative mobilization of the patient. This radiograph indicated the baseline postoperative stem position. The patients left the hospital after receiving full instructions from the physiotherapist for continued exercises at home.
Follow-Up Routine
Six weeks after implantation, a radiological and clinical follow-up was performed to repeat the anteroposterior pelvic plain radiograph. Additionally, all patients were interviewed concerning postoperative complications after discharge. Thirty-day and 1-year morbidity were documented using medical reports at the time of discharge and follow-up. Information on 30-day and 1-year mortality was obtained from the local register of deaths.
Outcome Measures
Radiological measurements were performed by 3 independent observers and orthopedic surgeons (M.K., Y.F., and M.D.), none of whom were involved in any of the surgical interventions. At the time of the measurements, the observers were blinded to the patients’ history and identity. Measurements were performed immediately postoperatively and 6 weeks later using the same technique. Due to the lack of radiostereometry or other specific software, the observers used an established measuring method 28 known to show high interobserver reliability. 29 We used the measuring method established by Bieger et al, 28 in which 3 different distances were measured and compared between the initial and follow-up anteroposterior plain radiographs of the pelvis: greater trochanter to shoulder of prosthesis (A), shoulder of prosthesis to most medial point of lesser trochanter (B), and greater trochanter to most medial point of lesser trochanter (C; Figures 2 and 3). Relevant migration of the femoral stem was assumed if there was a >2-mm difference between the measured distances without a variation in distance C.
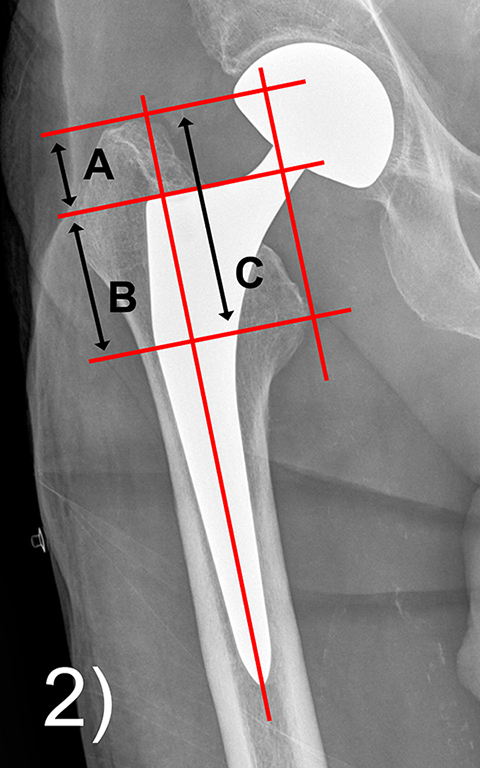
Anteroposterior plain radiograph of a right hip showing the measured distances.
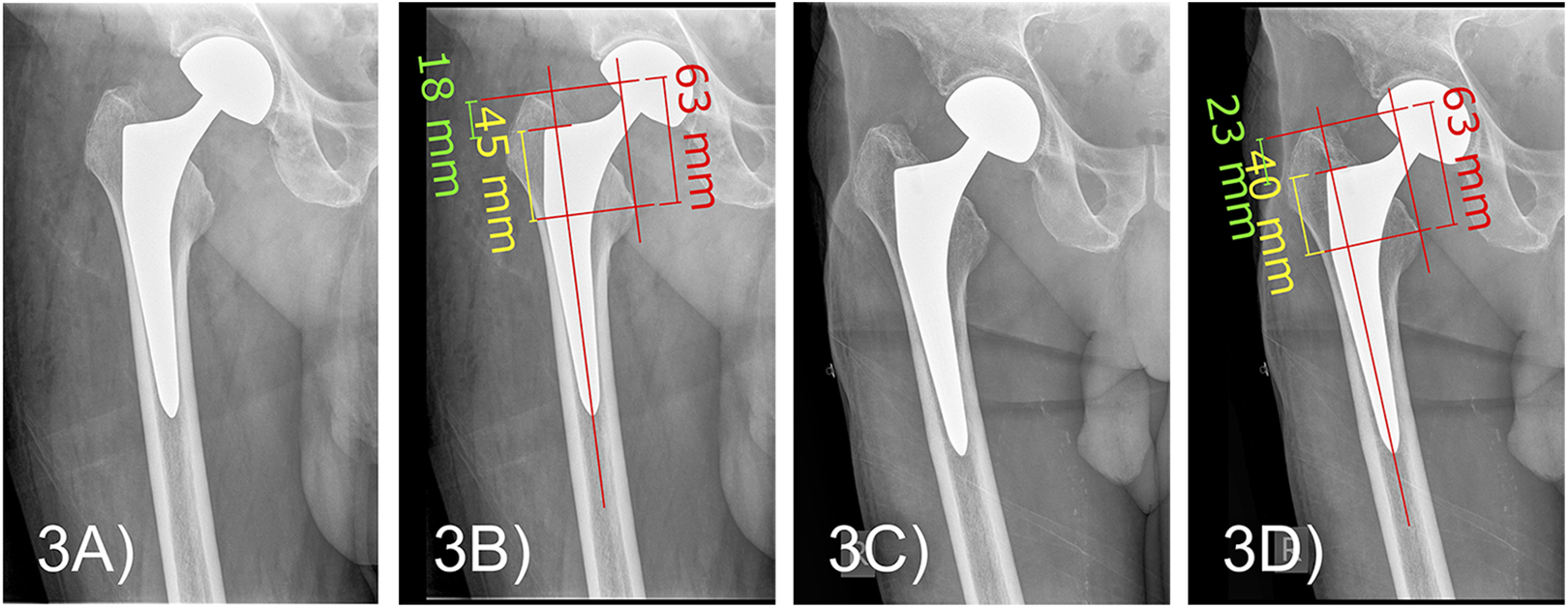
Example of measured distances with relevant migration (B, 18/45 mm vs D, 23/40 mm) without a change in distance C (greater trochanter to most medial point of lesser trochanter, 63 mm). A, After the operation. C, During follow-up.
Both the initial and follow-up radiographs were measured by all 3 observers. If the calculated sum of A + B differed by >2 mm from the measured distance C, a second measurement was performed to either prove or disprove the measurement result. The results of the 3 observers were compared, and the mean and standard deviation were used in cases of discrepancies. Pearson’s correlation coefficient r was calculated to demonstrate the relationships among the measurements of each investigator.
Bieger et al 28 defined a possible subsidence of <5 mm as minimal, 5 to 10 mm as moderate, and >10 mm as massive. Intraoperative iatrogenic fractures were recorded and classified according to the Vancouver classification for periprosthetic femoral fractures. 30 Intraoperative fluoroscopy was not routinely used for the procedures. However, if an intraoperative fracture was evident or suspected, fluoroscopy was used to assist decision-making regarding its treatment (eg, single or multiple wire cerclage of fractures of the proximal shaft, conversion to cemented HA in combination with cerclage). Local and systemic complications during the time of hospitalization were recorded. We therefore carefully documented hematomas, wound healing problems, infections, and all perioperative fractures. Any cardiovascular, pulmonary, neurological, or renal complication or failure was recorded as an early morbidity.
Retrospective radiological measurement concerning the femoral Dorr type classification 26 in the individuals showing an intraoperative fracture was done by using the anteroposterior radiographs of the pelvis at the time of fracture. Due to rotational error of the acutely injured leg, the measurements were obtained from the contralateral femur presuming the same degree of the systemic osteoporosis.
Statistical Analysis
Data were analyzed using SPSS (version 21.0; IBM Corp, Armonk, New York). Pearson’s correlation coefficient r was calculated to demonstrate the relationships among the measurements of the 3 investigators. An elevated coefficient (r > 0.7) indicated a high correlation.
Results
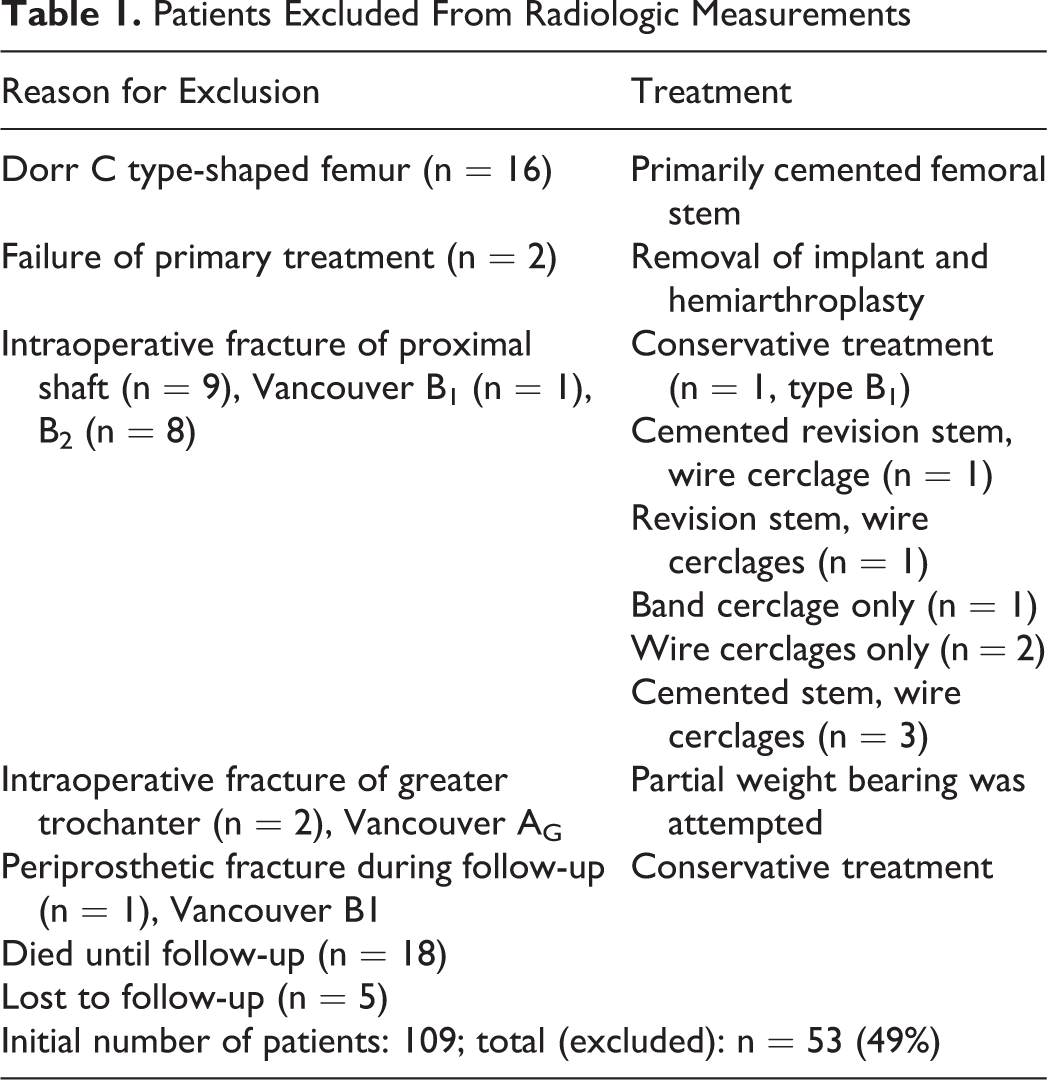
In total, 109 patients aged ≥90 years (81 women [74%]) underwent HA for femoral neck fractures. Sixteen (15%) patients were treated with a cemented femoral stem due to a Dorr type C proximal femur. Secondary HA was performed in 2 patients after failed osteosynthesis in another hospital (Table 1). One intraoperative death occurred among the 16 patients with cemented stems because of the development of a higher grade of BCIS.
Patients Excluded From Radiologic Measurements
There were 11 (12%) intraoperative fractures (Vancouver type AG, n = 2; B1, n = 1; B2, n = 8). While all type B2 fractures were addressed by revision during the same operation (Figure 4A and B), the 1 type B1 fracture was treated conservatively. Two patients had a fracture of the greater trochanter (Vancouver type AG) that resulted in a temporary weight-bearing restriction (Figure 4C). None of these patients were considered for further evaluation due to lack of comparability for radiological measurements. Two of 8 patients showing an intraoperative periprosthetic fracture which was addressed by a change in operative procedure showed a Dorr C type femur. Another 2 individuals with a fracture showed a Dorr B type shaft which was close to being type Dorr C. An initially clearly misjudged and unfortunate example of the chronological history of a Dorr C type femur with a femoral neck fracture is shown in Figure 5A–D. After an intraoperative fracture, which was found early postoperatively, a cemented revision stem combined with a wire cerclage had to be performed during revision surgery. In summary, there was 1 type Dorr A, 5 type Dorr B, and 2 type Dorr C configured femoral shafts in the cohort with intraoperative fractures.

A, An intraoperative fracture addressed with band cerclage only. B, A fracture addressed with cerclage and cement. C, A fracture of the greater trochanter.

A, Dislocated femoral neck fracture of the right femur with type Dorr C configuration. B, Initial postoperative situation after implantation of an uncemented hemiarthroplasty. C, Dislocated periprosthetic fracture of the calcar during hospitalization. D, Revision with cemented femoral revision stem and wire cerclage.
At the time of follow-up, 18 (17%) patients had already died before further examination. Many of these very old patients were not available for further postoperative radiographies caused by several reasons including medical, logistical, or personal reasons. After introducing this study, there were contacted trying to invite them for further follow-up examinations. At this point, unfortunately, they were already deceased, not knowing the cause of death. Five (5%) patients were lost to follow-up because of unknown contact details or relocation (Table 1). There was 1 periprosthetic fracture (Vancouver type B2; Figure 6) that was detected during radiological follow-up. The patient recalled no other trauma and demonstrated pain-free, boundless mobility.

Periprosthetic fracture (Vancouver type B2) detected during radiological follow-up and without clinical implications.
Overall, 53 (49%) patients in this cohort were excluded for the radiological measurements (Figure 7). In total, 56 (51%) patients with a mean age of 92.7 years (range, 90-102 years; 45 females [80%]) were followed up by radiological measurements. The median follow-up time until first radiological examination concerning possible subsidence was 42 days. The duration of hospitalization was 11.6 days, and most patients underwent spinal anesthesia (n = 60, 55%).
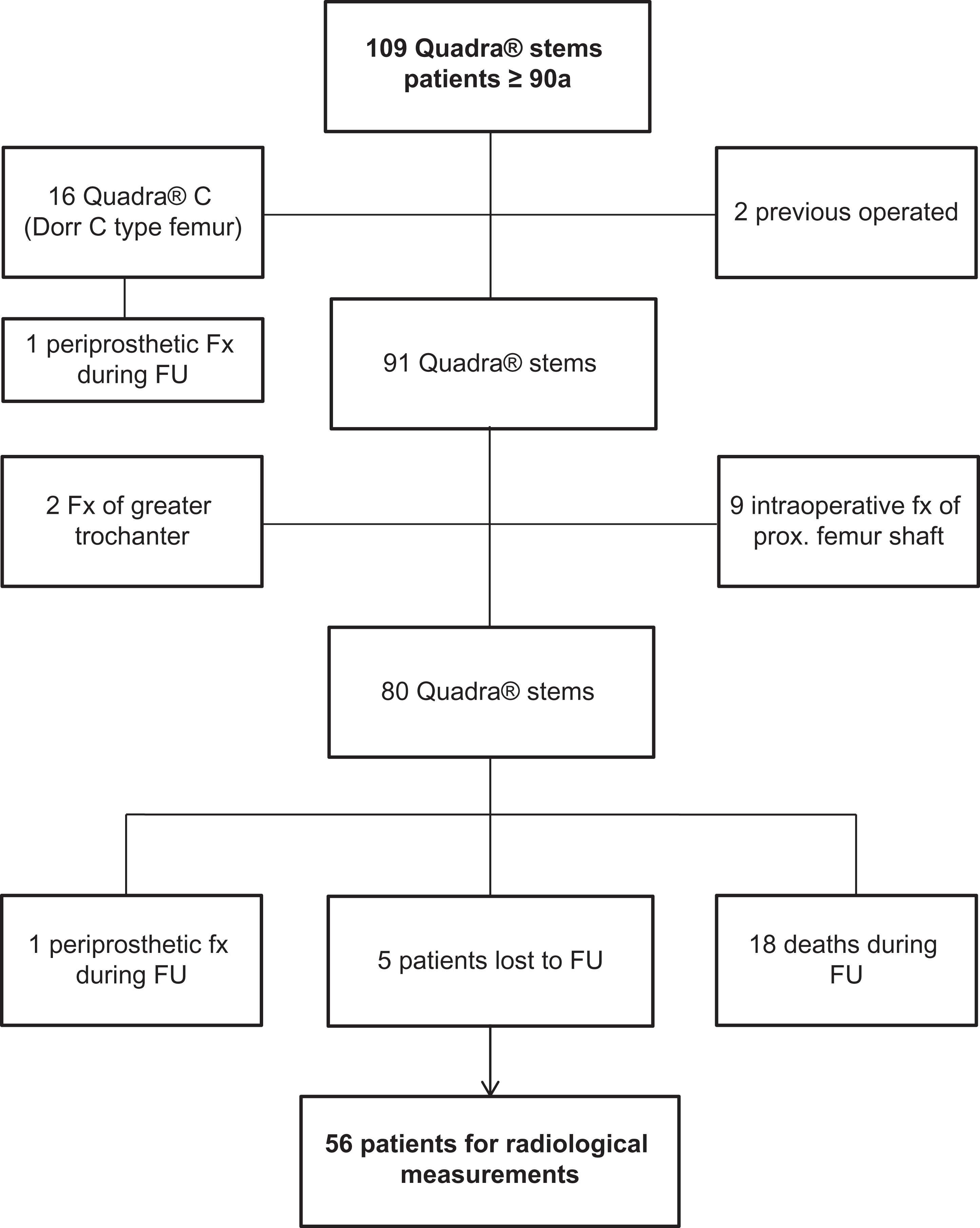
Flowchart: Synopsis of the Study.
Only 1 patient (94-year-old woman with severe cognitive impairment) died of meningitis within the first 30 days postoperatively; the meningitis might have been associated with an infectious local wound situation. The 1-year mortality rate for the final cohort was 23% (n = 18).
Examination of the medical reports of the final cohort (n = 56) revealed a 30-day morbidity rate of 27% (n = 15; Table 2). Two patients required a second intervention during hospitalization for evacuation of a hematoma. After the revision, both wounds healed uneventfully.
Early Morbidities.

With respect to potential radiological subsidence in the uncemented femoral stem, 39 (70%) patients showed no subsidence. Seventeen of 56 (30%) patients showed migration of >2 mm, leading to an average early migration of 3.9 mm (range, 2.5-9.0 mm; standard deviation, 2 mm) in those 17 patients. Only 2 (4%) patients showed subsidence of ≥5 mm (moderate), and none demonstrated a migration of >9 mm (massive) at the time of follow-up. Distal stem migration was confined to the first 6 postoperative weeks.
Interobserver reliability was evaluated by Pearson correlation coefficient r, which was 0.744, indicating good correlation. 31 All subsidence stabilized, and we documented no measurable subsidence from 6 weeks to 2 years among all 14 patients who were available for an additional follow-up examination 2 years postoperatively.
Discussion
Our results showed a very low rate of subsidence (≤5 mm, 5%; >9 mm, 0%) in those patients not showing a periprosthetic fracture, despite the old age of the patients and high likelihood of the presence of osteoporotic bone. These data are in accordance with other studies that demonstrated subsidence in up to 17% of their cohort, although the subsidence was <4 mm (range, 1-3 mm) in all patients. 32,33 Naudi et al 34 reported subsidence of >5 mm in 6.4% of their cohort of young patients with a mean age of 57 years (range, 28-77 years). Therefore, we cannot conclude that age, and probably bone quality, is an arbitrary argument for possible subsidence. On the other hand, the use of cemented stems is not a warranty against subsidence. Siepen et al 35 showed subsidence of >1.0 mm (range, 1.0-3.1 mm) in 11% of their cemented stems. Patients showing an intra- or postoperative periprosthetic fracture (12%) were excluded for further radiological measurement of subsidence. Nevertheless, all those patients presented a major degree of sinking of the femoral shaft over time of radiological follow-up.
In our study group, all but 2 patients were mobilized the first day after the operation with no weight-bearing restrictions. Olsen et al 21 found no difference in subsidence between partial versus unrestricted weight bearing after hip arthroplasty with an uncemented stem.
A leg length discrepancy of <1 cm is not usually recognized by the patient 36 ; therefore, possible subsidence should not be a counterargument against the use of cementless stems. In terms of the radiological measurement of subsidence, radiostereometry is still the most accurate modality with which to quantify movement of the prosthesis. 22 However, it is rarely used because of its need for in vivo markers and high cost. Newer software systems have an accuracy of 0.8 to 1.5 mm but are costly and require highly standardized anteroposterior views of the pelvis. 37,38 Despite these newer methods, most clinicians still rely on plain anteroposterior and axial radiographs of the hip. Although which anatomical landmarks should be used to assess migration of hip prostheses remains unclear, 28 the proposed landmarks may provide a practical solution. It is described that a change of rotation of the examined leg of 10° can lead to an inaccuracy of 0.37 mm in the radiological measurement. 39,40
Although no detailed radiological measurement of the Dorr classification was done prior to the surgical intervention, those patients showing a “stove pipe” morphology 26 of the femur neck were considered for cemented treatment due to higher risk for an intraoperative fracture. Despite applying this method to decrease the perioperative fracture rate, the treated cohort still developed a high rate of periprosthetic fractures. The decision to use a cemented prosthesis in femurs which showed a Dorr C type configuration must be considered as a small selection bias of our cohort. Retrospective review of the radiographs of those patients showing an intraoperative fracture leading to a change in operative procedure concerning the Dorr classification 26 pointed out that there were individuals with higher risk for complications. Two type Dorr C and 2 type Dorr B being close to Dorr C were initially addressed with uncemented implants and then developed intraoperative fractures. Taken this into account, the additional time for measuring the Dorr configuration prior to the initial surgical procedure could have decreased the rate of intraoperative rate of complications due to using a cemented implant.
One patient with a primarily cemented stem developed a higher grade of BCIS that led to a lethal intraoperative cardiopulmonary complication. We believe that BCIS can be prevented by avoiding the use of bone cement, especially in very old patients. 20
In times of diagnosis-related groups, the costs might also be an arbitrary factor in favor of using one implant or the other. With respect to the calculated cost of each implant, the cemented stem is half the price of the uncemented stem. However, after adding the prices for the bone cement, cement gun, vacuum pump, jet lavage instruments, saline solution, and diaphyseal plug, the prices of the 2 stems are almost identical. The price difference of the stem is approximately US$700 in favor of the uncemented implant. By adding the cement gun, bone cement, plug for the shaft, saline solution for lavage, and jet lavage instruments, the total difference is merely 11% of the total cost of the HA. However, the additional operation time when using cement (approximately 15 minutes 6 ) is not taken into account in this calculation. An increased rate of surgical site infection is generally associated with an increased operation time for hip and knee arthroplasty. 41,42 Unless using antibiotic-free cement, there seems to be no distinct risk of higher infection rates caused by the cement itself. 43
Considering the benefits of uncemented implants, the high number of 11 (12%) intraoperative fractures in the present study can partially be understood knowing from the literature different factors can lead to an increased rate of these complications. In their randomized clinical trials, Foster et al 44 reported an intraoperative fracture rate of 7.0% and 7.5%, respectively, in patients treated with uncemented stems and rates of 0.0% and 0.9% in those treated with cemented stems. The use of uncemented implants is well known to be associated with a higher incidence of intraoperative fracture complications than is the use of cemented implants. 18,45 In particular, in a teaching hospital, the learning curve for uncemented implants is known to be more difficult and a longer period of time is required to lower the complication rate. 46 Although we did not perform a randomized trial, the chance of developing a decreased rate of fractures by using cemented implants is likely. Chammout et al 47 recently published a single-blinded randomized controlled trial including only 69 patients, in which total hip arthroplasty was performed for the treatment of displaced femoral neck fractures. The study was stopped early because the number of hip-related complications was substantially higher in the uncemented group. Four intraoperative periprosthetic fractures were counted in the uncemented group of 34 patients. Another randomized controlled study performed by Inngul et al 48 revealed 9 intraoperative periprosthetic fractures and 4 greater trochanter fractures in 74 patients. The authors of both studies advised against using uncemented stems. Both studies treated patients clearly younger than in our cohort (73 and 81 years vs 93 years, respectively). In a study of BCIS, Olsen et al 20 found that the odds ratio for 30-day mortality after cemented HA was 2.21 for patients aged >85 years and 2.85 for patients with an American Society of Anesthesiologists class of >II. It is the responsibility of the surgeon to individually deliberate whether to use a cemented or uncemented implant for nonagenarians. Two settings should be considered: on one hand, preventing a periprosthetic fracture with taking on the risk of a BCIS by choosing a cemented shaft, and on the other hand, reducing the risk of cardiopulmonary complications by selecting an uncemented HA and therefore accepting the possible threat of a periprosthetic fracture.
The stem (Quadra H) used in our cohort was not initially designed for the anterior minimally invasive approach, which might also be a reason for an increased rate of intraoperative fractures. Yu et al 49 demonstrated an intraoperative periprosthetic fracture rate of 11% versus 0% when using a conventional versus short stem, respectively, in hip arthroplasty. Dietrich et al 50 also described lower complication rate with shorter stems while using the direct anterior minimally invasive approach. Almost all orthopedic companies offer shorter implants that are easier to handle and supposedly associated with a lower complication rate. In a recent study, Meneghini et al 51 pointed out that the introduction and implementation of the direct anterior approach represents a higher risk for early femoral failure. Advantages of this approach reported over the last years consisting of earlier rehabilitation, 52 less blood loss, or time under anesthesia seem also to be debatable. Even though we cannot prove results due to the lack of data, our experience cannot verify this. A high percentage of surgical interventions were performed or assisted by experienced surgeons who are well trained in this technique. In terms of recovery of this very old cohort, almost 100% of the treated patients were mobilized on the first postoperative day with full weight bearing. Zhao et al found functional advantages in early recovery after using the direct anterior approach compared to the posterolateral approach. 52
Limitations
This study had certain limitations. Eighteen (17%) patients deceased already early, while 5 (5%) were lost to follow-up and unavailable for follow-up examinations. We considered this to have been caused by the very old age and numerous comorbidities of this cohort. Two other studies showed mortality rates of 22% and 30% during 6- and 24-month follow-ups in cohorts of older patients with fractures (median age of 85 years). 10,18 Additionally, Petruccelli et al 36 reported a >35% complication rate in a cohort of patients aged >89 years treated by elective hip or knee arthroplasty. Because of the lack of radiographs taken prior to the first instance of weight bearing, we are unable to objectively determine whether subsidence of the femoral stem occurred between the end of the implantation procedure and the first postoperative mobilization of the patient. Ström et al 53 observed no migration from the end of surgery to the end of the first postoperative week. Interventions with intraoperative periprosthetic fractures leading to either application of a cerclage or conservative treatment of the surgical complications were not included in the radiological measurement of subsidence. This must also be mentioned as a limitation of this study. Our radiological control examination took place already 6 weeks after the operation. We supported to do so because of the very old age of our cohort and its limited life expectancy. In the recent literature, subsidence seems to be a process that occurs only during the first few weeks postoperatively. 6,21,32,34,53 We again emphasize that we did not compare 2 cohorts. Although information on the intraoperative fracture rate showing lesser osseous complications for cemented prosthesis is available, 42 we cannot scientifically prove that fewer intraoperative fractures would have occurred with a cemented implant in our very old cohort. Looking at recent literature and taking into account our patients all show rather osteoporotic bone, it is very likely that cemented prosthesis reduces the risk of periprosthetic fractures. To our best knowledge, no comparable study exists using cemented implants in a cohort of nonagenarians. We do not know the bone mineral density of the fractured femurs, which were possibly osteoporotic. We did not analyze whether each patient’s comorbidities had an impact on either subsidence or the fracture rate. This study only emphasized the objective measurement of early migration of the femoral component after HA implantation without intra- or postoperative periprosthetic fractures. In order to gain exact anteroposterior radiographs of the hip, we used the local standard positioning. Due to the possible rotational error of the radiographic anatomical landmarks used for measuring the subsidence, there is a possible limitation for measurement precision. 39 No clinical scores or functional outcomes were observed. Therefore, we cannot determine whether subsidence influenced those factors.
Conclusion
This retrospective observation of a very old cohort with displaced femoral neck fractures treated with uncemented HA and a minimally invasive anterior approach has shown that the concerns about migration of the femoral stem are unsubstantiated. Our study revealed negligible radiological subsidence for those patients not showing intra- or postoperative fractures. In most cases, the subsidence did not lead to subjective limitations for the patients. Taking into consideration that uncemented implants show an increased rate of intraoperative fractures of osteoporotic bone, this operation should only be performed by experienced surgeons, who in case of complications are able to address those. Implantation of cemented HA might be protective of periprosthetic fractures and should therefore be considered liberally. The use of standard length femoral shafts being accompanied by higher complication rate when applying the minimal invasive approach could also be reconsidered. In addition, further effort to define the femoral configuration concerning the Dorr classification prior to surgical treatment to avoid intraoperative complications should be conducted.
By definition, this type of operative treatment significantly increases the ability to prevent BCIS. Early and late mortality should accordingly decrease, leading to higher satisfaction for both the patient and surgeon. Furthermore, the longer operation time associated with the cementing procedure and the slight difference in expenses for the operation materials are economic objectives that must be considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.