
Abstract
Objective:
We sought to understand older patients’ perspectives about their fall, fall risk factors, and attitude toward emergency department (ED) fall-prevention interventions.
Methods:
We conducted semistructured interviews between July 2015 and January 2016 of community-dwelling, nondemented patients in the ED, who presented with a fall to an urban, teaching hospital. Interviews were halted once we achieve thematic saturation with the data coded and categorized into themes.
Results:
Of the 63 patients interviewed, patients blamed falls on the environment, accidents, a medical condition, or themselves. Three major themes were generated: (1) patients blamed falls on a multitude of things but never acknowledged a possible multifactorial rationale, (2) patients have variable level of concerns regarding their current fall and future fall risk, and (3) patients demonstrated a range of receptiveness to ED interventions aimed at preventing falls but provided little input as to what those interventions should be.
Conclusions:
Many older patients who fall do not understand their fall risk. However, based on the responses provided, older adults tend to be more receptive to intervention and more concerned about their future fall risk, making the ED an appropriate setting for intervention.
Introduction
In the older adult population (age 65 and older), accidental falls have long been considered a leading cause of preventable injury, functional disability, and mortality by public health experts. 1 Older adults fall frequently; annually, 1 in 3 community-dwelling older adults experience a fall. 2,3 Each year the estimated direct medical cost of fall-related injuries is ∼$31.3 billion. 4 This cost is likely to increase as this population age 5 -7 ; and the total cost is estimated to increase to $67 billion by the year 2020. 8
While the majority of unintentional falls in the older population do not result in significant injury, 9 the resultant overall decline in health, loss of confidence, social isolation, and increased risk of admission to nursing homes are well-documented phenomena. 10 -13 Falls remain the number 1 cause of death due to injury in adults aged 65 and older. 7 Annually, there are more than 27 000 deaths and ∼2.5 million nonfatal injuries from falls in this population. 7 Further, older adult falls serve as a major risk factor for future falls, 14,15 having a compounding effect on morbidity. Studies have found that within 6 months of emergency department (ED) discharge, the fall recurrence rates ranged from 14% to 48%. 10,16,17 Thus, falls in this population are widely considered to be sentinel events.
Current guidelines recommend all older adults to be screened for their risk of falls and those with a balance and/or gait abnormality or those who suffer multiple falls undergo a multifactorial fall evaluation and targeted intervention. 18 A Cochrane meta-analysis showed multifactorial interventions significantly reduced the rates of fall. 19 Geriatric ED guidelines suggest how to evaluate the fall risk factors. 18
Previous qualitative studies of elderly patients’ views on falls and fall-prevention consistently described denial of the personal relevance of fall-prevention interventions and diminished personal risk as barriers to care. 20,21 These studies were conducted in nonclinical settings and notably not in the setting of a recent fall. To date, no studies assessed ED patients’ understanding of their fall and fall risk nor their openness to ED fall interventions. The success of ED fall-prevention programs may depend upon patients’ attitudes regarding therapy, their illness-related insight, and their receptiveness to referral from the ED. In this study, we sought to explore older patients’ understanding of their recent falls, perceptions of future fall risk, and attitudes toward ED falls prevention interventions.
Methods
Study Design
Between July 2015 and January 2016, 2 of the investigators (D.T. and C.T.R.) conducted semistructured, open-ended interviews with older adults in the ED who had recently fallen. The primary aim of these interviews was to elucidate patients’ perceptions of fall that precipitated their ED presentation, future fall risk, and receptiveness to ED interventions aimed at preventing future falls. This study was a part of a larger pilot falls referral program. This study was approved by our institutional review board.
Population and Setting
Patients were identified while receiving care in the ED of an urban, academic level 1 trauma center with 100 000 visits annually. We included community-dwelling patients aged 65 and older. We excluded patients with dementia and patients whom ED clinicians thought were too ill or inappropriate for interviewing. Patients who did not speak English were able to participate via interpreter services.
Patients were recruited and enrolled 7 days per week from 8
Patients were approached for a brief cognitive assessment and dementia screening, utilizing the validated 6-item Cognitive Impairment Test (6CIT). 22 Patients scoring in the normal range (0-7) were consented for the study. Those scoring 8 or more were excluded, given the difficulty of conducting interviews of patients with dementia.
Study Protocol
Interviews were conducted in patient rooms. If patients were not in a room (ie, in a hallway bed or open waiting area), they were taken to private consultation rooms for interview.
The interview tool was developed by the principal investigator (S.W.L.) based on review of the literature and expert opinion on pertinent aspects of patient perception regarding falls (see Table A1). The interview tool was piloted and refined to adequately cover the scope and context of our research question. Two investigators (D.T. and C.T.R.), trained by the senior author (S.W.L.) in interview techniques to minimize interviewer bias, conducted and recorded interviews. The final questionnaire consisted of 3 close-ended questions pertaining to the patients’ fall history and 5 open-ended questions pertaining to their views of their most recent fall.
All interviews were audio recorded and were transcribed verbatim. Periodic reviews of transcripts were performed to evaluate for emerging themes, and interviews were halted when thematic saturation was reached.
Data Analysis
Throughout the data collection period, the transcripts were independently reviewed by 2 of the investigators (S.W.L. and D.T.). At the 7-month mark, interim analysis was conducted, determining the thematic saturation after enrolling a total of 63 patients, at which point enrollment was halted. Two investigators (S.W.L. and D.T.) again reviewed the transcripts to gain better understanding of context, key concepts, and scope. 23 One reviewer (S.W.L.) then created an initial thematic framework by condensing and later paraphrasing data to generate themes informed by previous experience, noted response patterns, and the stated aims of this study. The transcripts were then reread by the 2 reviewers (S.W.L. and D.T.) independently and codes generated inductively in accordance with established qualitative research methods based on grounded theory. 23,24
The 2 reviewers (S.W.L. and D.T.) discussed common concepts and generated a final code list. 23,24 The 2 investigators then coded the transcript independently, 23,25 and a κ score was generated to assess inter-rater agreement between the independently coded transcripts of a subset of interviews. 25 The 2 reviewers (S.W.L. and D.T.) discussed any discrepancies in assigned codes through negotiated consensus. 24 The coded data were then organized into concepts and themes. Demographic data were calculated using Microsoft Excel 2016 (16.0.7329.1051) 32-bit.
Results
Our final sample included 63 participants. Between the 2 reviewers based on the final code list, the κ score was 0.75. Two participants had incomplete interviews. The average age was 79.9 years (standard deviation [SD]: 8.5); there were 46 female and 17 male patients. The mean number of falls in the past year was 2 across the entire sample (see Table 1). Table 1 lists age, gender, English speaking, and the number of falls in the past year. Table 2 lists the themes and subcategories.
Participant Characteristics

Themes and Subcategories

Abbreviation: ED, emergency department.
Theme 1: Patients Blamed Falls on the Environment, on Themselves, on a Freak Accident, or on a Medical Condition but Never Noted a Multifactorial Rationale
During the course of interviews, all patients either blamed their falls on a specific entity, such as “the brick walkways,” on themselves for being “stupid” or “not paying attention,” or on nothing at all, often stating, “…I just fell.” One theme that emerged early on was that patients perceived the environment was at fault for their falls. People blamed things ranging from “uneven sidewalks,” to “black ice,” to a “pile of blankets.” One patient when asked about her current risk factors for falls stated: …so, I was using the walker and I gotta tell you, I ran over a mouse, and I went back like this, and the walker fell, and I fell…If it wasn’t for the mouse, none of this would have happened.
Another prominent subtheme that emerged was self-blame. Many participants either referred to themselves as “stupid,” described “rushing,” or simply “not paying attention.” One patient encompassed all 3 of these principles in a response to questioning, saying, “This one I was really stupid…not to remember that the chair was there, and I should’ve been paying attention. Yeah, and not being in such a hurry.” Another patient responded to a question about what the fall meant to her with “I’m angry with myself because I’m stupid. I don’t look where I’m walking.” Yet another patient attributed her fall to carelessness, even going as far as to actively deny there was anything else contributing to her fall, stating: I think in both instances it was an element of carelessness. I am always in a hurry. I feel better about that, as opposed to a serious problem. I don’t feel as if it is a medical problem, but I just need to be more careful.
Freak accidents were another recurring subtheme. Many patients described the events as things that just happened. People described going “flying” out of nowhere and sensations of being “thrown,” with no clear antecedent event. For instance, 1 patient who fell stated, “I wiggled myself out of the chair, took 2 steps to the phone, turned around, and the next thing you know I’m sailing across the room.” Another man described his fall as, “I was just walking and, wow, it was like somebody threw me.” While several participants alluded to the idea that this fall was just a freak accident, many people plainly described it as such: “I mean, well, it just happened…just a freak accident,” 1 patient said in response to the question of what the fall meant to her. Another man responded to that same question with, “nothing, it was a fluke.”
Some patients demonstrated some understanding of medical conditions as potential fall risks, with many citing strength or balance as important factors, while others tended to blame specific body parts as issues. One patient, for example, cited balance, but like in other cases, she immediately diminishes the relevance to this particular fall: “…you know I have balance issues, so I have to be careful. But I don’t fall because of those.” Another patient who stated that he had no risk factors for falls said this when asked what he would do to prevent future falls: “Be a little more careful that’s all. Vertigo has been awful. I never had good balance.” Overall, 17 (27%) patients mentioned balance as an issue during the interviews, but none of them addressed the issue as part of a group of risks, and only 1 spoke of therapy aimed at improving balance. Weakness, both general and of a specific body part, was also mentioned. One man said, “…my knee that I had surgery [on] is very weak and painful. I don’t think I could ever have a second knee surgery.”
In all, many patients blamed a variation of things, but no patients described multifactorial causes of these falls. Some patients, although few (3 patients), did attribute their falls to “getting old.” For example, 1 patient said: Oh boy, risk factors…well I have, although it doesn’t have anything to do with it, I have positional vertigo…I find that when I get older, that didn’t have anything to do with this particular fall um, but um, I just um, as I get older I am more unsteady.”
Theme 2: Patients Have Variable Emotions About Their Current Fall and Variable Concerns About Future Fall Risk, Ranging From Extremely Concerned to not at All Concerned
Although 37 patients were concerned (extremely, mildly, a little, and somewhat), 26 (41%) patients were either “not concerned” or indifferent. Of those 26 patients, 21 of them were coded as not concerned. Patients who were not concerned frequently had short answers to questions that addressed their level of concern for risk of future falls such as, “no,” “I’m not concerned,” and “not at all.” Only 19 (30%) of 63 patients directly admitted to having risk factors when asked. There were again several patients who listed risk factors, as above, but subsequently denied or diminished their importance or relevance. Further, 40 (63%) of 63 patients denied having or did not know whether they had any risk factors for future falls, with 28 participants denying having any risk factors all together.
Several participants cited mitigating factors, such as baseline activity, as potentially risk reducing factors. For instance, 1 participant when asked about his risk for future falls stated: I am very active, and I workout and stuff. So, I don’t think so. My balance is good. I try and do stuff too fast; I am very abrupt with my movements and turning.” Another participant who stated he had no risk factors later said,…you need to know in what condition the person is in. If a person has rheumatism, these people are in bad shape. You may need to do something for them. As for me, I tripped while I was jogging.”
The majority of patients were concerned to some degree. Some of these participants exhibited low to moderate level of concern, as in, “I’d say I’m a little concerned about falling again. I took a little spill today, and I can tell you this isn’t fun”; or another, who simply replied, “[I’m] moderately concerned.” Others voiced more concern, with many stating they were “extremely concerned” or “very concerned.” One patient, for example, said she was “scared…very concerned, absolutely.” Another said, “[falling] is always in the back of my mind.”
Slightly more than half of the patients described the ways in which they would prevent future falls, given their concern. However, a minority of patients put forth actionable items when asked what they would do to decrease the risk of future falls. The most common theme was to elevate the level of attentiveness. A majority of these responses involved “being more careful,” “paying attention,” or “being more aware,” with 27 (43%) participants offering 1 of these as the primary method of risk reduction. In contrast, 4 (6%) patients mentioned some form of therapy or exercise, and only 7 (11%) patients said they would use stabilizing devices, such as canes, walkers, wheelchairs, or the use of handrails.
Ultimately, there was a wide range of response around questions of concern and risk. Overall, there seemed to be a discrepancy of real and perceived risk. The patients also appeared to rely heavily on paying attention and being careful in efforts to prevent future falls, whereas there seems to be little focus on the use of physical therapy or strengthening exercises. There was also, notably, no mention of medication reviews or comprehensive evaluations.
Theme 3: Patients Demonstrated a Range of Receptiveness to ED Interventions Aimed at Preventing Falls, with Very Little Input as to What Those Interventions Should be
We asked patients 2 questions regarding ED interventions aimed at preventing falls: (1) How would you feel about the ED trying to prevent you from falling in the future? and (2) What would you think should be part of an ED effort to prevent you falling again? Question #1 was added to the original interview tool during the data collection process to more adequately address the scope of our research aims. Answers ranged widely. There were many patients who seemed receptive to the idea of an intervention, but few of them had ideas about what that should entail. For instance, 1 person who was open to ED intervention said: I don’t know what you could do, but I guess if you could do something, that would be great. But, I don’t know what that is.
Although most patients viewed ED intervention positively, with statements ranging from “…why not?” to “I would love that,” still there were some who thought it was unnecessary or had clear trepidation. These answers ranged from outright rejection, for example, “I don’t need that,” to patients saying, “I don’t know how I would feel about that.”
When it came to patient perspectives about what might be part of an ED intervention, there were few who offered intervention ideas. Most participants either stated, “I don’t know,” or they used praise of the ED physicians to the effect that there was nothing left to do. For example, 1 patient responded: Everything’s been perfect I have no complaints. Treated me well, watching my blood pressure which goes up when this happens and I am sure I’ll be taken care of. I can’t complain as far as I know they are doing everything fine. They put me in. I’m here; somebody’s here with me. The doctors have been in. I have no complaints. Do know that you should never put loose carpets and Persians down. I think care should be taken in the shower. I think a great deal of falls are in the shower. We mustn’t trifle with our strength and ability to walk. Tell them…. One of the things that they teach you once you have an operation is how to use your other appendages to do things, to get up…to stay up. You could teach people. You have to be sure to let seniors know is there is no shame. Be sure that people know that as you get older, the first thing to go is your legs. They need to remember that they have to work on their strength. You need to tell people to exercise. You have to teach people to take care of themselves and to exercise because the body is made for exercise…. It’s made to be used.
Discussion
This study is the first to examine the perspectives of older adults (aged 65 and older) who have recently fallen and who were ED patients. We found that older adult ED fall patients lack understanding about their fall risk and have varied perceptions about their future fall risk and desire for ED fall-prevention interventions. Our study provides important insight into patients’ understanding of their personal fall risk profiles and their attitudes toward intervention by ED clinicians.
In our study, we found that patients blamed many different things for their falls, most prominently, self and the environment, but no participants understood the multifactorial nature of older adult fall risk. 26 -29 Some patients did recognize that their advancing age could perhaps be contributing to their fall risk, which is in some ways multifactorial although never made explicit. It is not surprising that patients tended to blame the environment, as a previous study of community-dwelling older adults showed outside environmental factors were perceived to be the only important factors for personal risk of fall. 21 Even ED providers, however, often use inappropriate or vague terminology to describe the etiology of a patient’s fall so it is not surprising that patients have inadequate understanding of their fall risk. This underscores 2 important points: (1) the patient minimizes their fall risk and (2) the clinicians are also unaware of the patient’s fall risk. Together, these issues highlight the need for broad clinician and patient understanding regarding future fall risk and the need for more urgent evaluation. 30
This study also found there was varied level of concern and emotional response in older adults who had recently fallen. In some ways, these findings are consistent with previous studies carried out in nonclinical settings, in that diminished personal risk was frequent. 20,21 Unlike those studies, 20,21 the majority of our patient group was concerned (mildly to extremely) about future falls, irrespective of their perspectives on personal risk; whereas community-dwelling people without a recent fall tended to be less concerned. 20,21 This is an important distinction because the effectiveness of some health behavior interventions may rely on motivational factors, such as concern. 31 Level of concern is a major driver of consciousness raising, which has the potential to make ED visits an important time for teachable opportunities for the older adult faller. 31,32
Lastly, we found that patients varied in terms of receptiveness to ED intervention and what that intervention might entail. Patients in community-based studies rejected interventions, dismissing them as not personally relevant. 20,21 Participants in this study, however, differed from previous studies, in that a majority of participants in the ED viewed the idea of a falls prevention intervention positively. Whereas in the community, this population rejected falls prevention interventions, including advice, viewing fall-prevention advice as potentially patronizing and distressing. 20 The patients in our study who offered potential interventions overwhelmingly recommended advice and counseling. This supports our thought that proximity to a fall and the setting of an ED have the potential to transform the way patients approach falls prevention strategies. Thus, the ED could be an ideal place to intervene, improving the health of this population, 33,34 and reducing health-care costs. 35 For this to be successful, however, patients must have some understanding of their fall risk and be open and willing to participate in such an intervention. This insight could help guide patient–physician conversations directed at counseling or at referral to multidisciplinary teams aiming to prevent future falls.
Limitations
There were many limitations of this study. The external validity may be limited by population characteristics and severity of illness differences among EDs. Our sample was unbalanced with respect to gender, but we interviewed enough patients to reasonably overcome gender differences. Further, like many other qualitative studies, this study utilized a small sample size. Our study inherently lacks application to a sicker population of elderly fallers who have dementia, live in skilled nursing facilities or are otherwise institutionalized. Also, patients who are not demented but have acute changes in mental status will likely be screened out of the study by the 6CIT dementia screening tool, which is reasonable because studies of outpatient falls prevention program efficacy have failed to demonstrate an effect in older adults with dementia. 36 Furthermore, patients could have answered in ways to increase social desirability. 37 Lastly, we did not pose any qualitative questions regarding their level of concern or future fall risk to the ED physician treating these patients; being able to compare these 2 response would have generated insight as to how well patients understood their diagnosis and advice given by their care team.
Conclusion
Patients do not understand the full spectrum of fall risk and often blame themselves for not paying attention, blame the environment, or blame another factor. Although patients’ openness to intervention and their concern for future falls varied, our ED patients were more concerned about fall risk and more interested in fall-prevention interventions initiated in the ED, after a fall, than healthy older adults in the community. This may make the ED an ideal setting for a fall-prevention intervention.
It is clear that many of these patients deny their own multifactorial risk of falls but appear to be more inclined to engage in fall prevention than is otherwise noted in the outpatient literature. 19 Emergency department physicians should talk to patients about their falls and perhaps about some things they could to reduce their risk of future falls. Emergency department interventions aimed at preventing falls in older adults have great potential to make an impact, given the time proximity of falls prevention engagement to the actual fall. While it is natural to use this information to increase patient education on fall risk, EDs should also engage these patients on promotion of activities that enhance fitness, balance, and mobility. 38 This emphasis on improving balance would likely increase confidence in balance rather than provoke anxiety about risk, with potentially beneficial consequence for physical functioning and fall risk. 39
Footnotes
Appendix A
Key Interview Tool Questions.
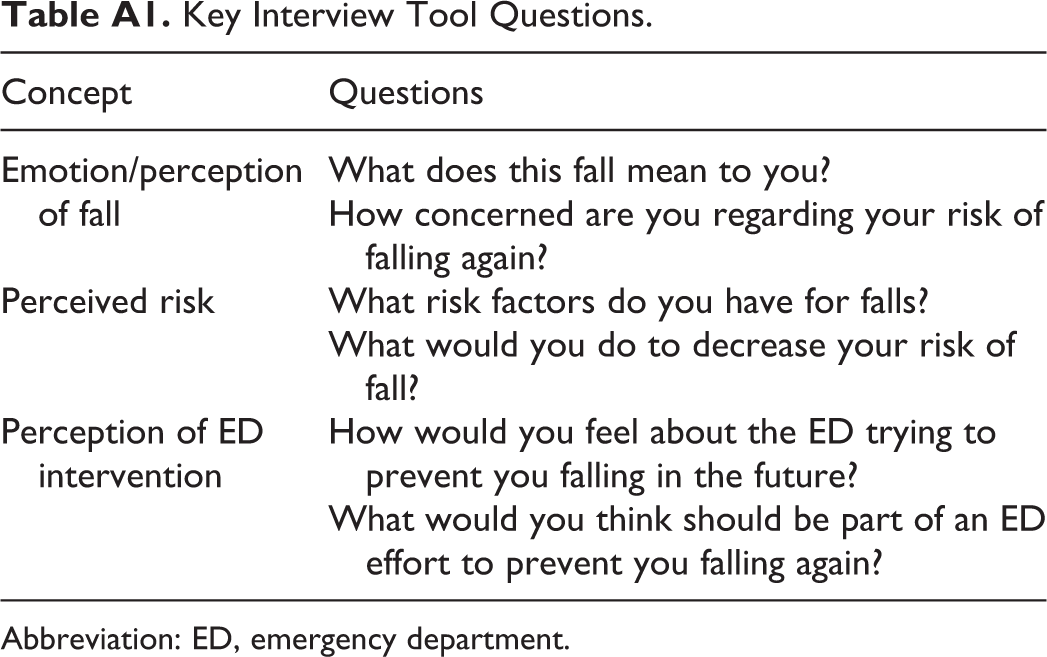
| Concept | Questions |
|---|---|
| Emotion/perception of fall | What does this fall mean to you? |
| How concerned are you regarding your risk of falling again? | |
| Perceived risk | What risk factors do you have for falls? |
| What would you do to decrease your risk of fall? | |
| Perception of ED intervention | How would you feel about the ED trying to prevent you falling in the future? |
| What would you think should be part of an ED effort to prevent you falling again? |
Abbreviation: ED, emergency department.
Authors’ Contribution
K.N.S. and S.W.L. conceived the initial study. S.W.L. undertook the statistical analysis with the help of D.T. Authors K.N.S. and S.W.L. drafted the article, and D.T. and C.T.R. contributed to its revision. K.N.S. takes responsibility for the article as a whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.