
Abstract
Introduction
We aimed to describe patient awareness regarding fall prevention and education, perceived causes of falls, and changes in attitude after experiencing a fall through interviews with older Korean patients who experienced falls with resultant hip fractures.
Materials and Methods
We conducted face-to-face semi-structured in-depth interviews with 11 patients who were admitted to Kangbuk Samsung Hospital for hip fractures caused by falls and were referred to the Department of Rehabilitation Medicine for postsurgical rehabilitation between June 2022 and June 2023. The data were analyzed using the phenomenological method developed by Colaizzi.
Results
Before hip fracture, none of the patients had received fall prevention education or perceived its necessity; however, they recognized its necessity retrospectively. Participants described the causes of falls as carelessness, actions taken at the time of the fall, environmental factors, and decreased physical function. Most participants believed that falls could be prevented through personal caution and activity restrictions. Some mentioned fall prevention education, exercise, wearing appropriate shoes, environmental adjustments, and seeking assistance from others as methods of preventing future falls. Most patients reported adopting a safety-seeking attitude after experiencing hip fracture. Many patients had negative thoughts such as guilt or thoughts of death, whereas only a few reported increased interest in education and exercise.
Conclusions
We observed a lack of fall prevention education, misunderstanding regarding the cause of falls, and negative psychological changes after experiencing hip fractures due to falls in older Korean individuals. Recognizing and managing patient perceptions is crucial for effective fall prevention, requiring both healthcare provider awareness and active participation from patients and caregivers.
Introduction
Falls are the most common cause of both fatal and non-fatal injuries among individuals aged ≥65 years. 1 Annually, 27.9% of older adults in the United States, 23.4% in European countries, 18.5% in China, 15.9%–25.1% in Korea, and 26.5% in the world experience falls.2–5 Falls may lead to fractures, head injuries, fear of falling, and other injuries, which eventually result in significant pain, decreased quality of life, and impaired daily functioning, including decreased mobility, increased dependency and medical expenses, and mortality. 6
To prevent falls in the older individuals, current guidelines recommend identifying target patients, stratifying their fall risks using brief screening tools, assessing multifactorial risk factors, and providing individualized interventions.7–9 Fall prevention has been investigated in multiple randomized control studies, analyzed by systematic reviews and meta-analyses, and has shown efficacy reducing fall-related risk factors, rate of falls, fall-related fractures, and fear of falls and increasing fall-related efficacy.10–12
Understanding the gap between research and real-world setting is crucial to optimize fall prevention interventions and reduce falls occurrences. Previously suggested gaps include a low level of knowledge regarding fall prevention among patients 13 , lack of patient education during admission 14 , and inability to recall the education. 14 Fear of falls, which develops in 21-39% of patients who experience falls, may unnecessarily restrict their activity level and cause deconditioning, which is also a barrier to fall prevention. 15
In South Korea, the fall-related mortality in 2022 was 5.3 per 100,000 individuals, which is lower than the Organization for Economic Co-operation and Development average of 9.2 per 100,000 individuals 16 ; however, the rate has increased. Based on our clinical experience, the awareness of falls in South Korea is generally considered low.
Qualitative research is useful for understanding a patient’s thoughts on fall prevention and the gap between the research and real-world setting for fall prevention. Furthermore, this methodology is useful for identifying differences in thoughts based on cultural, economic, and environmental variations among populations. To the best of our knowledge, limited qualitative research has been conducted on falls experienced by Koreans. Therefore, we aimed to describe patient awareness of fall prevention and education, identify barriers to fall prevention, and describe changes in attitudes among patients after experiencing a fall.
Methods
Study Design
This qualitative study used the phenomenological methodology proposed by Colaizzi 17 to qualitatively describe the meaning and essence of the participants’ perceived thoughts after experiencing a fall. The study was reviewed and approved by the Institutional Review Board of Kangbuk Samsung Hospital (IRB no. KBSMC 2023-08-030), and all participants signed a statement of informed consent. The study was reported according to the consolidated criteria for reporting qualitative studies (COREQ) (Supplemental File 1).
Participant Recruitment
The participants were recruited from patients who were admitted to Kangbuk Samsung Hospital, a large tertiary hospital in Seoul, Korea for hip fractures caused by falls and were referred to the Department of Rehabilitation Medicine for post-surgical rehabilitation. The inclusion criteria were individuals (1) aged ≥65 years who had experienced a hip fracture due to a fall, (2) who were community-dwelling before experiencing the hip fracture, and (3) who could understand and answer the study questions. The exclusion criteria were participants who had unstable medical conditions, declined to participate, or had neuropsychiatric disorders that could influence conversations.
From June 2022 to June 2023, we interviewed as many individuals as possible to maintain representativeness. Twenty candidates were identified, nine of whom refused to participate in the interview because of surgical site pain or a desire for rest. At the time of recruitment, we collected data on baseline characteristics, including age, sex, fracture side and site, and fall site.
Risk factors for falls that were present before experiencing the hip fracture were identified through interviews or from medical records. Direct physical function assessments were limited at the time of interview due to post-operative status. Therefore, the risk factors for falls were from previous studies.18,19 The information collected from the participants included previous history of fall, old age, female sex, use of psychoactive medication, decreased physical function, neuropsychiatric conditions, requiring the use of an assistive device before the hip fracture, and decreased visual acuity.
Interview Procedure
We conducted face-to-face, semi-structured, and in-depth interviews. Interviews were conducted once per patient during the consultation for rehabilitation after hip surgery in a comfortable room separate from the inpatient room. The same researcher (H.S.L.) conducted all interviews to ensure consistency. Participants were assured of the anonymity of their interviews prior to the interview, and the interviews were recorded to ensure accurate data collection.
Interview Question Guide.
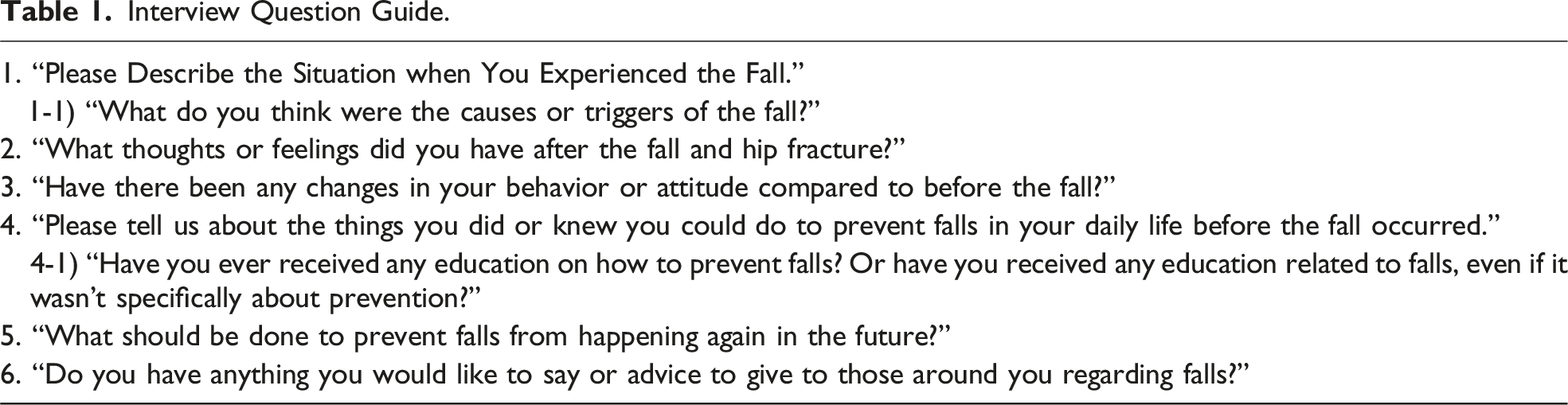
The interviewer attempted to elicit meaningful experiences from the individuals and interpret their narratives by drawing on their knowledge on rehabilitation and falls. The questions were primarily open-ended to allow the participants to freely express their opinions. The interview did not follow the above sequence of questions strictly, to avoid interrupting the participants’ narration. We did not restrict the interview duration; the average duration was approximately 15 mins. Member checking could not be done after analyzing the transcripts because many participants were discharged shortly after their interviews.
Data Analysis
The interview content was transcribed verbatim by the first author (W.H). The transcripts were reviewed by co-researchers to ensure accuracy. After conducting interviews with six participants, the entire research team reviewed the contents and identified themes during a regular team meeting and continued the process until saturation was reached. The data were reviewed every two interviews until saturation. After eleven interviews, no new content emerged, and data acquisition was discontinued.
Considering the Colaizzi’s phenomenological method, we adapted the following sequence of data analysis. First, the two researchers (W.H and K.R.O) listened to the audios and read the transcripts several times to fully understand the flow of each conversation. Second, meaningful statements were identified and listed (W.H and K.R.O). Third, the thoughts and perspectives underlying these statements were extracted (W.H and K.R.O). Fourth, similar thoughts were classified into keywords, then into subthemes, and the main ideas in the subthemes were categorized into themes (W.H and K.R.O). Fifth, thoughts, subthemes, and themes were checked by expert clinicians (K.K, C.S.G, J.B, M.W.P, and C.P) and the whole research team.
Results
Participant Characteristics.

Theme 1: Perceptions on Fall Prevention.
Theme 2: Perceptions on the Causes for Falls.

Theme 3: Changes in Attitude After Experiencing Falls.
Theme 1: Perceptions on Fall Prevention
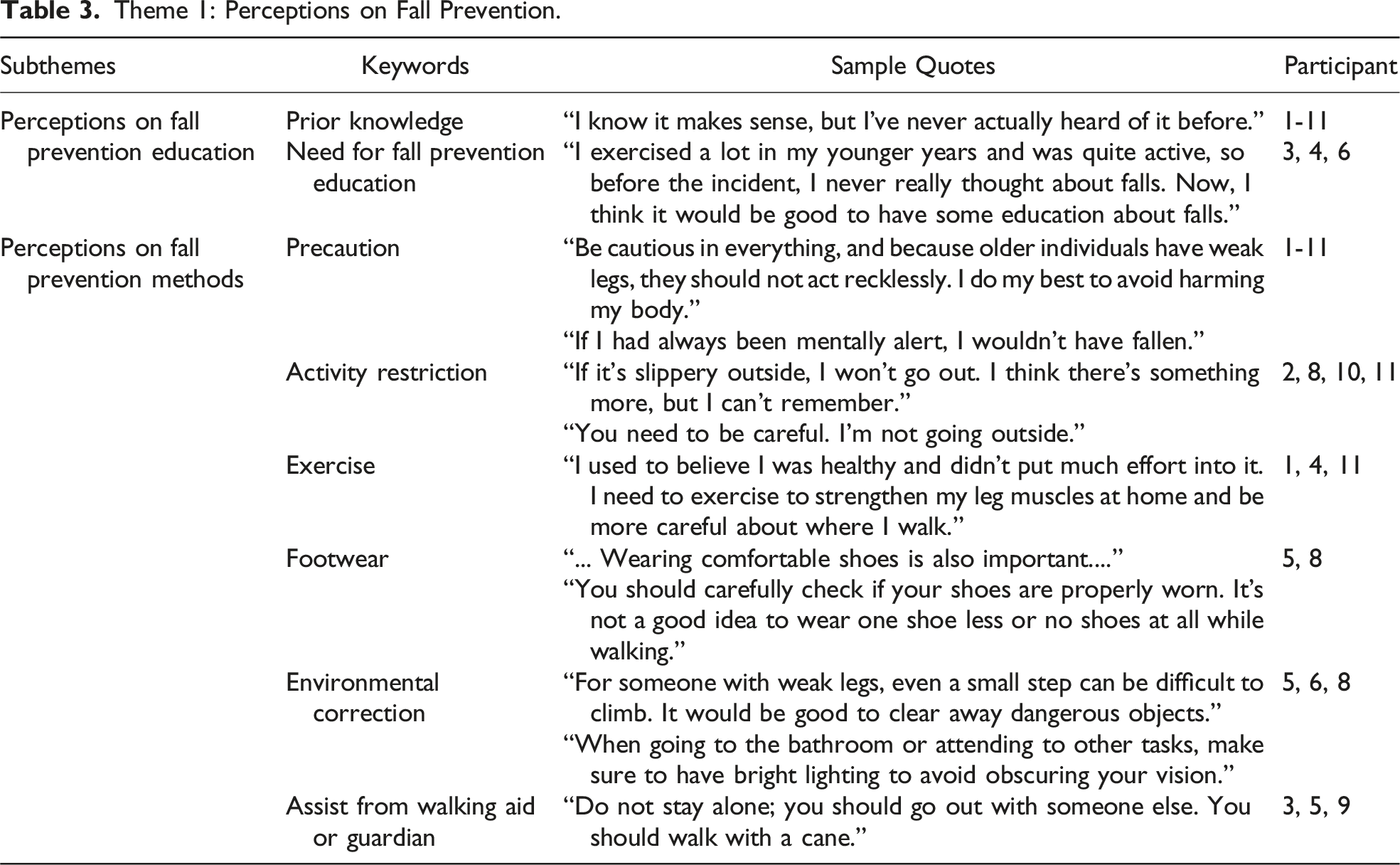
Participants’ responses regarding their perceptions on fall prevention were categorized into two subthemes: perceptions on fall prevention education and on fall prevention methods (Table 3).
Perceptions on Fall Prevention Education
When the participants were asked whether they had received prior information regarding fall prevention, all participants stated that they had not. Participants were unaware of the need for fall prevention education before experiencing falls and retrospectively recognized its importance. (Table 3) “... I didn’t think about falls because I exercised a lot and was active when I was young. I still thought of myself as young. After this incident, I think it would be good to have education about falls. I didn't know how dangerous falls were, and I didn't even suspect that I might get hurt even if I lay down for over an hour. …” (Participant 3, a 74-year-old female) “... I thought I was healthy, so I believed only in that and didn't put in much effort. …” (Participant 4, an 87-year-old female) “... I thought that falls are more for those much older than I am, so I didn’t care. …” (Participant 6, a 69-year-old male)
Perceptions on Fall Prevention Methods
All but one participant perceived falls as preventable events. Participant 4 thought that although it would be good to exercise or take precautions to prevent falls, ultimately, these measures would be insufficient to completely prevent falls. Among those who perceived falls as preventable, several responses were identified regarding their reactions toward fall prevention methods, including precautions, activity restrictions, education, exercise, wearing well-fitting footwear, adjusting their environment, and seeking assistance from walking aids or guardians. (Table 3)
All participants responded to the precautions, emphasizing the need for constant vigilance to prevent falls. Activity restrictions included avoiding slopes, high places, and slippery surfaces. “... I don’t want anyone like me to be here, so I would advise them to be cautious and avoid getting hurt …” (Participant 1, an 81-year-old female) “... I will just move back and forth on level ground. I won’t climb …” (Participant 2, an 81-year-old male)
Education focused on raising awareness on the risk of falls and teaching coping strategies. Three participants mentioned exercise as a fall prevention method, although only one could specifically mention strength training as the type of exercise. Regarding footwear, participants mentioned wearing comfortable and properly fastened shoes. Environmental adjustments involved clearing obstacles that cause tripping or visibility hazards. Three participants suggested the presence of a guardian, whereas one (participant 9) mentioned the use of a walking aid. “... There should always be someone at home. One should not be alone...” (Participant 9, an 84-year-old female)
Theme 2: Perceptions on the Causes of Falls
The participants described various factors as the causes of falls, including their carelessness, actions at the time of the fall, environmental factors, old age, and weakened leg muscles. Six participants pointed their carelessness as the cause of the fall and mentioned instances in which they failed to use assistive devices such as walkers or handrails. They also mentioned situations in which they failed to visually perceive the placement of their feet, resulting in stumbling and falling. Seven participants mentioned environmental factors as a cause of falls including slippery floors, dark areas, and obstacles on the floor. Five participants attributed falls to their actions at the time of the fall, such as climbing to a high place to perform tasks, using both hands while walking (carrying heavy objects using both hands and holding a blanket using one hand while walking), and adopting an unstable posture (placing too much weight on one foot). Three participants primarily attributed their falls to decreased physical functioning. Among them, one cited decreased agility owing to aging, whereas the other two identified decreased lower limb strength owing to inadequate nutrition and underlying medical conditions (Table 4). “...On a rainy day, I climbed onto a chair to repair the academy's window. In the process, I slipped owing to my right leg, which had not been in good condition lately, and fell…” (Participant 3, a 74-year-old female) “... At night, I went to the bathroom without turning on the light. As I was coming out, I tripped over the door threshold and fell…” (Participant 6, a 69-year-old male)
Theme 3: Changes in Attitude After Experiencing a Fall
Most participants exhibited changes in attitudes and behaviors (9/11), whereas the remaining two participants (participant 2, an 81-year-old male; participant 8, a 92-year-old female) reported no changes. For these two, their discussions primarily consisted of thoughts toward their own pain and quick recovery.
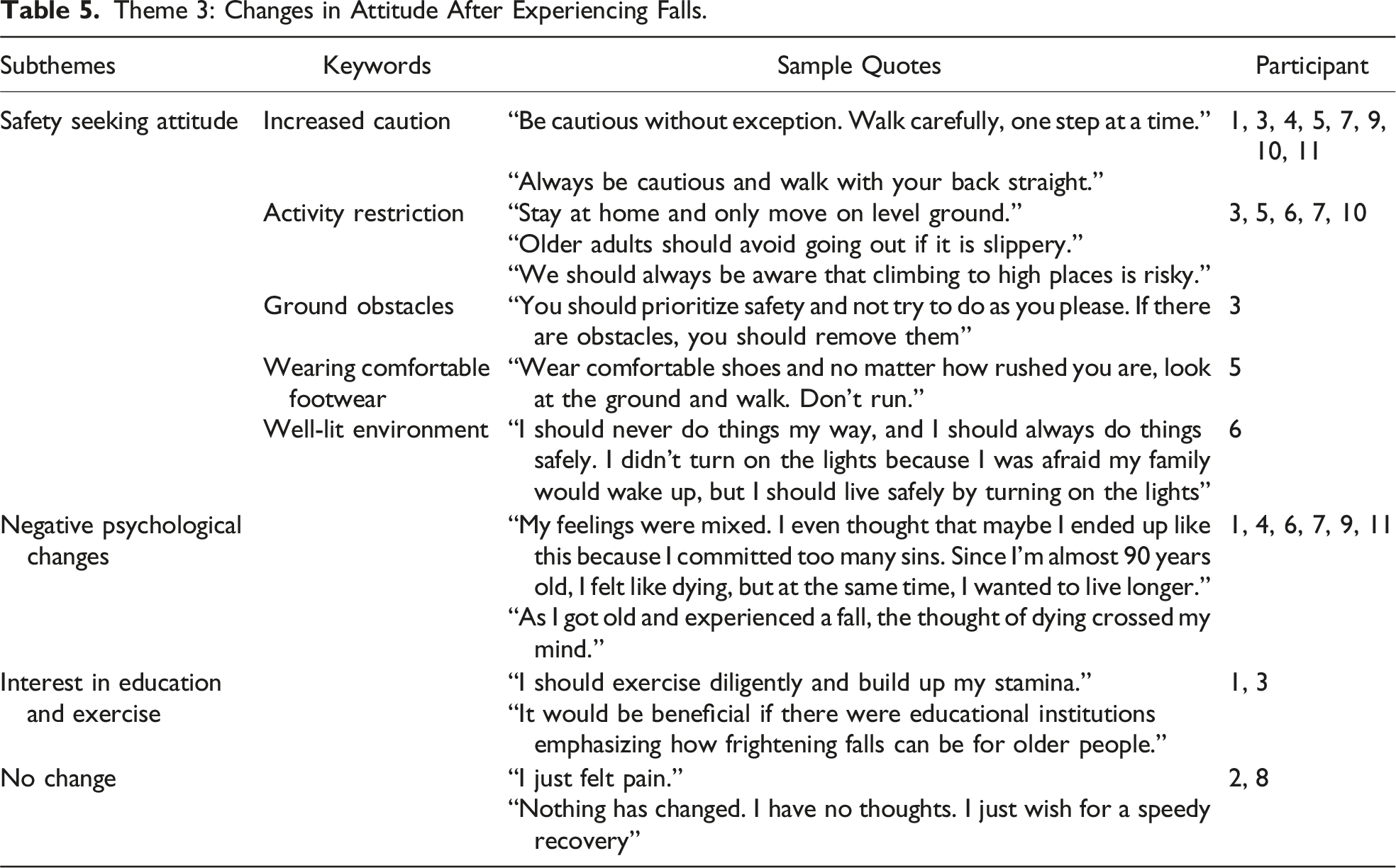
The changes experienced by the participants owing to falls were categorized into three subthemes: activity restriction and safety-seeking attitudes, frustration and reduced self-esteem, and interest in education and exercise. (Table 5)
Safety Seeking Attitudes
Most participants (9/11) expressed a change in attitude after experiencing a fall, emphasizing the need for increased caution to prevent future accidents. Five participants acknowledged the need for activity restriction. This restriction included avoiding slippery surfaces and heights, and three participants recommended avoiding all outdoor activities. One participant emphasized the importance of a well-lit environment, the other stressed the need for caution regarding ground obstacles, and the third highlighted the significance of wearing comfortable footwear. “... Be cautious without exception. Walk carefully, one step at a time…” (Participant 1, an 81-year old female) “... If outside is slippery, older adults should avoid going out....” (Participant 10, an 83-year old female)
Negative Psychological Changes
Six participants experienced feelings of guilt, thoughts of death, and negative perceptions on the situation following their falls and hip fractures. “... My feelings were mixed. I even thought that maybe I ended up like this because I committed too many sins. Since I’m almost 90 years old, I felt like dying, but at the same time, I wanted to live longer...” (Participant 4, an 87-year old female) “... As I got old and experienced a fall, the thought of dying crossed my mind....” (Participant 9, an 84-year old female)
Interest in Education and Exercise
Only two participants demonstrated awareness regarding the importance of exercise and future prevention after their fall. “... It would be beneficial if there were educational institutions emphasizing how frightening falls can be for older people...” (Participant 3, a 74-year-old-female)
Discussion
In this qualitative study, we conducted face-to-face, semi-structured, and in-depth interviews with 11 older Koreans who had experienced a hip fracture owing to a fall to investigate their perceptions regarding fall prevention. Before the hip fracture, none of the participants had received fall prevention education or perceived its necessity; however, they recognized its need retrospectively. The participants described falls to be due to carelessness, actions taken at the time of the fall, environmental factors, and decreased physical function. Most participants believed that falls could be prevented through personal caution and activity restrictions. Some mentioned fall prevention education, exercise, wearing appropriate shoes, environmental adjustments, and seeking assistance from others as methods of preventing future falls. Most patients reported adopting a safety-seeking attitude after their hip fracture. Furthermore, many patients had negative thoughts such as guilt or thoughts of death, whereas only a few reported increased interest in education and exercise.
Notably, none of the participants in this study received fall prevention education before their hip fracture. The participants were community-dwelling older individuals with risk factors for falls who could have received education on fall prevention. Previous studies reported a similar lack of fall prevention education among community-dwelling older individuals. In a qualitative study of 66 older people aged 61-94 years in the UK, almost all participants stated that they had not received any prior communications regarding fall prevention. 23 Similarly, a qualitative study of 30 Chinese older people showed similar lack of fall prevention education and poor acceptance to fall prevention interventions. 24 Lastly, a survey including 2012 people aged over 60 years old in Korea showed that 91.8% of them did not receive any prior fall prevention education. 25 Although fall prevention education is considered crucial in fall prevention, various barriers exist. 26 From a healthcare provider’s perspective, time limitations and competing demands, knowledge and skill deficits, and lack of coordination are the suggested barriers to fall prevention education. 27 From a patient perspective, older individuals reportedly normalize their fall, underestimate fall risk, and take advice as unnecessary, irrelevant, and a threat to their self-identity.23,28–30 Multimedia- and bingo-based education has been studied to enhance the delivery of fall prevention education and has been shown to increase the gain in knowledge.31,32 Efforts to overcome the aforementioned barriers are required to further enhance the delivery of fall prevention education to community-dwelling older individuals.
Although many participants in this study described the primary cause of falls as carelessness, actions at the time of the fall, and environmental factors, only two participants described them to be due to decreased physical function. None of the participants discussed their prescribed medications as the cause of fall. In previous studies, patients were able to identify various causes of falls33,34; however, our study participants primarily attributed factors related to the circumstances at the time of the fall. This could be due to a tendency to normalize their status, to avoid commenting on their physical impairment, or a lack of knowledge regarding falls.
In this study, attitude changes after experiencing falls mostly included seeking of safety and negative thoughts, while education and exercise were also considered to some extent. This was similar to the findings in a previous research, where patients experienced anger, fear, and embarrassment and expressed concerns and anxieties regarding future falls. 35 In another study on in-hospital falls, patients exhibited various reactions such as apathy, self-blame, reluctance to report falls, negative feelings toward nurses, and overestimation of their own abilities. 36 Negative thoughts arising after a fall may be considered normal psychological distress but can potentially lead to depression 37 or be associated with negative health behaviors. 38 Therefore, negative thoughts must be appropriately managed.
For fall prevention, the importance of multimodal interventions encompassing exercise and physical activity, medication, vitamin D intake, and cardiovascular, vestibular, and visual health has been emphasized. 7 Most patients in this study believed that falls could be prevented by addressing various modifiable factors within these domains; however, only few participants responded that they should engage in exercise for fall prevention. Moreover, they were not well informed on the appropriate types of exercise. Balance and functional exercises at least thrice a week for at least 12 weeks are recommended to prevent falls. 7 Another notable aspect of this study is that although many patients were consuming medications with a high fall risk, such as benzodiazepines, Z-drugs, antihypertensives, and diuretics, they lacked knowledge regarding the relationship between these medications and falls. Therefore, patient and caregiver education on fall prevention should include accurate strategies to prevent falls, including the aforementioned perspectives.
To the best of our knowledge, this qualitative study was the first to examine perceived thoughts of older Koreans after a fall with resultant hip fracture, which is one of the most devastating outcomes after falls. However, our study had some limitations. Since the interview was conducted during admission, the participants were in a relatively acute phase after hip fracture surgery. Therefore, further studies should investigate whether attitude changes persist in the long term, how this affects their future risk of falling, and what interventions can be implemented to reduce this risk. Although the data was saturated, another limitation of this study is our small sample size (n = 11) and lack of sample size calculation.
Since the proportion of men was low in this study, it was difficult to observe differences in perceptions of falls between men and women. However, previous studies showed gender differences in the perceptions of falls. A qualitative study involving 27 older adults in USA showed that women approach fall prevention by controlling extrinsic risk factors indoors, while men approach it to reduce risk analytically by employing safety measures for outdoor activities. 39 Another interview study including 40 older adults in England showed that men who perceived themselves as “responsible” and “rational”, expected to reduce their own risk of falling, while women had tendency to blame themselves or others for their falls. 40 Patriarchal values are usually strong in Asian countries, therefore we may expect to observe stronger gender differences. 41
All participants were older individuals residing in urban areas. Previous studies in Korea and China have reported that the rate of falls is higher in rural areas than in urban areas.2,42 This is attributed to factors such as increased outdoor activities among rural-dwelling older individuals, rough or hilly terrain, living alone, functional impairments, and musculoskeletal conditions resulting from rural lifestyles.2,25,43 Therefore, urban and rural-dwelling older individuals may differ in their awareness and attitude changes regarding the causes of falls. Further studies should investigate the differences in awareness and attitude changes after falls between rural and urban areas.
Conclusions
In this study, we elucidated the lack of fall prevention education, misunderstandings related to the cause of falls, and negative psychological changes after experiencing hip fractures due to falls in older Korean individuals. Recognizing and managing patient perceptions are crucial for effective fall prevention, requiring both healthcare provider awareness and active participation from patients and their caregivers.
Supplemental Material
Supplemental Material - Lack of Fall Prevention Education in Patients Experiencing Fall-Related Hip Fracture: A Qualitative Study
Supplemental Material for Lack of Fall Prevention Education in Patients Experiencing Fall-Related Hip Fracture: A Qualitative Study by Wonjae Hwang, Kyung Rok Oh, Min Gyun Kim, Won Bin Kim, Hyun Seung Lee, Sun Gun Chung, Jaewon Beom, Myung Woo Park, Kyung Su Kim, Joonghee Kim, Chul-Hyun Park, and Keewon Kim in Geriatric Orthopaedic Surgery & Rehabilitation.
Footnotes
Acknowledgements
The authors would like to thank all the participants in this study and all experts and hospitals who supported this study.
Author Contributions
Conceptualization and design: All authors (W.H, K.R.O, M.G.K, W.B.K, H.S.L, S.G.C, J.B, M.W.P, K.S.K, J.K, C.P, and K.K). Funding acquisition: K.K. Data acquisition (participant interview): H.S.L. Data analysis: W.H, K.R.O. Original draft: W.H, K.R.O. Revision: W.H, K.R.O, M.G.K, W.B.K. Review, editing, and approval of the final manuscript: All authors (W.H, K.R.O, M.G.K, W.B.K, H.S.L, S.G.C, J.B, M.W.P, K.S.K, J.K, C.P, and K.K).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the This research was supported by a grant from the Patient-Centered Clinical Research Coordinating Center (PACEN) funded by the Ministry of Health & Welfare, Republic of Korea (grant no. HC21C0064).
Ethical Statement
ORCID iDs
Data Availability Statement
The authors confirm that the data supporting the findings of this qualitative study are available within the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.