
Abstract
Introduction:
Introduction: Adequate calcium and vitamin D from diet and supplementation is recommended for elderly hip fracture patients. Using data from the multinational hip fracture arthroplasty trial (HEALTH), we determined the proportion of patients who consistently took vitamin D and calcium and which characteristics/prescribing practices were associated with consistency of supplement use.
Methods:
HEALTH is a multicenter randomized trial of elderly hip fracture patients treated with hemi-arthroplasty and total hip arthroplasty. Patients were categorized as consistent users, inconsistent users, or nonusers of calcium and vitamin D. We used multinomial regression to determine the characteristics associated with calcium and vitamin D use.
Results:
603 HEALTH participants were included in the analysis. 34.7% of patients never took vitamin D within 12 months after surgery, 26.2% took vitamin D inconsistently, and 39.1% took vitamin D consistently. 36.0% of patients never took calcium within 12 months after surgery, 28.4% took calcium inconsistently, and 35.7% took calcium consistently. There was great variation in prescribed/recommended doses. Compared to nonusers, consistent users of the supplements were more likely to be female, North American, prescribed/recommended vitamin D and/or calcium postoperatively, and presented to a facility with comprehensive fragility fracture protocols.
Conclusions:
A low proportion of elderly hip fracture patients are consistently taking vitamin D and calcium, which may contribute to poorer bone health. Surgeons should be educated to prescribe/ recommend vitamin D and calcium, institutions should develop comprehensive fragility fracture protocols and patient education strategies to ensure that patients with osteoporosis receive bone health management beyond fracture care.
Introduction
The refracture rate in patients with hip fragility fractures is very high, with up to 14% of patients sustaining a second fragility fracture. 1 Vitamin D and calcium supplementation are frequently advised in elderly populations, especially relating to prevention of, and after, hip fractures and to reduce the very high rate of refractures in this population. 2,3 Vitamin D and calcium supplementation have been shown to have positive effects including increasing 25(OH)D serum levels, 4 improving bone mineral density, 5,6 and reducing the risk of falls. 7,8 Additionally, studies have shown that calcium and vitamin D supplementation is a cost-effective method of preventing future fragility fractures in patients who have sustained a hip fracture. 9,10
The current Osteoporosis Canada clinical practice guidelines recommend routine vitamin D supplementation with 800 to 1000 IU daily for healthy adults older than 50 years, although up to 2000 IU per day may be necessary for higher risk adults. 2 Additionally, the Canadian guidelines state that calcium intake from diet and supplements should be 1200 mg daily. Guidelines in the United States and United Kingdom are similar, recommending at least 1000 mg of calcium and 800 IU of vitamin D. 3,11 Despite these guidelines, a recent survey of orthopedic surgeons in Canada and the United States found a lack of consensus on prescribing practices for calcium and vitamin D in fracture patients, as well as a large variability in dosing regimens. 12
Adherence to calcium and vitamin D supplementation has been shown to vary greatly in previous studies, from 20% to over 60%. 13 -15 As with other pharmacological therapies, treatment adherence is likely to have an important influence on the efficacy of calcium and vitamin D supplementation. For example, studies in highly controlled populations with high compliance have shown benefits of calcium and vitamin D supplementation, whereas studies in community settings with less strict controls on adherence show fewer benefits. 16,17 An analysis of elderly patients with femoral neck fractures treated with internal fixation found that over half of patients (54.3%) were either not taking or not consistently taking vitamin D following their fracture. 18
The ongoing multicenter HEALTH trial 19 (randomized controlled trial in elderly femoral neck fracture patients comparing hemi-arthroplasty and total hip arthroplasty) provides a unique opportunity to determine whether elderly hip fracture patients are consistently taking vitamin D and calcium supplements following a hip fracture treated with joint replacement in a clinical trial. It also provides an opportunity to explore factors associated with the consistent use of vitamin D and calcium supplementation. Using data from this trial, the objectives of the current study are (1) to determine the proportion of patients who consistently take vitamin D and/or calcium following arthroplasty, (2) to describe which doses of vitamin D and calcium are frequently used among patients enrolled in HEALTH, and (3) to determine which baseline characteristics and management/prescribing practices were associated with consistency of vitamin D and calcium use.
Methods
Health Study Overview
The HEALTH trial (NCT00556842) is a multicenter randomized controlled trial that compares hemi-arthroplasty versus total hip arthroplasty in patients older than 50 years with displaced femoral neck fractures. Sixty-one clinical sites in 10 countries in North America, Europe, and Australia are participating in the HEALTH trial. The primary objective of the HEALTH trial was to determine the rates of unplanned secondary procedures within 2 years in individuals with displaced femoral neck fractures treated with hemi-arthroplasty versus total hip arthroplasty. Secondary objectives include comparing health-related quality of life and health outcome measures, mortality, and hip-related complications in the 2 treatment groups. Patients were assessed clinically at 1 and 10 weeks and 6, 9, 12, 18, and 24 months postsurgery. This trial is coordinated by the Centre for Evidenced-Based Orthopaedics (McMaster University) and has been approved by the Hamilton Integrated Research Ethics Board (#06-151), as well as all participating clinical sites’ research ethics boards/institutional review boards.
Vitamin D and Calcium Supplementation Substudy
All patients enrolled in HEALTH were asked whether they take vitamin D and calcium supplementation, and the dose of each, at the study follow-up visits. To be included in this substudy, patients had to attend at least 3 of the 5 study follow-up visits within 12 months and had to have reached at least the 12-month study follow-up visit. Based on their reported frequency of vitamin D and calcium supplementation in the first 12 months of follow-up, patients were categorized as either consistent users (positive report at 4-5/5 visits), inconsistent users (positive report at 1-3/5 visits), or nonusers (positive report at 0/5 visits) of vitamin D and/or calcium.
Vitamin D and Calcium Supplementation Prescribing Practices at Clinical Sites
At the first postoperative visit, the HEALTH trial protocol recommended that surgeons prescribe 1000 IU of vitamin D and 600 mg of calcium and that surgeons initiate investigation and treatment of osteoporosis as recommended by a local osteoporosis expert/consultant. Clinical sites had different standards of care for prescribing vitamin D and calcium, which were acceptable to the HEALTH protocol. To learn more about these practices, principal investigators and research coordinators at participating clinical sites were asked to describe if and how vitamin D and calcium were prescribed or recommended in elderly arthroplasty patients at their hospital/clinic, for example, whether there is a standardized protocol for managing fragility fractures at their site.
Data Analysis
Patient characteristics were summarized using descriptive statistics. Categorical baseline variables were summarized as counts and percentages. Continuous baseline data were summarized as means and standard deviations. The doses of vitamin D and calcium used were summarized using the median, interquartile range, and mode. Prescription/recommendation practices were also summarized using descriptive statistics as described above.
Multinomial logistic regression models were used to determine whether the following independent variables were associated with consistency of vitamin D and calcium supplementation: (1) age, (2) sex, (3) location of hospital (North America vs Europe and Australia), (4) a prescription or recommendation to take vitamin D and/or calcium upon hospital discharge, and (5) management practices (comprehensive pathway/protocol vs some protocol vs no standard protocol/unknown practices). Odds ratios (ORs) with 95% confidence intervals (CIs) were reported to compare nonusers, inconsistent users, and consistent users for both calcium and vitamin D. Statistical significance was determined at α = .05. All statistical analyses were performed using SPSS version 24.
Results
Patient Demographics
Of the 824 HEALTH participants who had reached their 12-month visit, 603 were included in this analysis. We excluded data from the 100 patients who had died prior to their 12-month visit and the 121 participants who did not have at least 3 postoperative visits. The mean age of the study participants was 78.6 years (standard deviation: 8.8), and most participants were female (73.1%). The majority of patients were enrolled at clinical sites in North America (244, 40.5%) and Europe (325, 53.9%; Table 1).
Patient Demographics.

Abbreviation: SD, standard deviation. ASA, American Society of Anethesiologists.
Vitamin D and Calcium Supplementation
Two-hundred nine (34.7%) patients reported never taking vitamin D within the first 12 months after surgery, 158 (26.2%) reported taking vitamin D inconsistently, and 236 (39.1%) reported taking vitamin D consistently (Table 2). Two hundred seventeen (36.0%) patients reported never taking calcium within the first 12 months after surgery, 171 (28.4%) reported taking calcium inconsistently, and 215 (35.7%) reported taking calcium consistently (Table 2). Vitamin D and calcium use consistency was highly correlated (Spearman ρ: .861; P < .001). There were 197 (32.7%) participants who consistently used both calcium and vitamin D and 194 (32.2%) participants who consistently did not use calcium nor vitamin D.
Consistency of Vitamin D and Calcium Use.

Vitamin D and Calcium Doses
Of the patients who took vitamin D at 1 visit or more, 24 different doses of vitamin D (21 daily and 3 weekly) were identified. The most common doses of vitamin D included 1000 IU (464/1147 visits), 800 IU (409/1147 visits), and 2000 IU (104/1147 visits). The median daily dose taken was 1000 IU (Q1-Q3: 800-1000 IU; Table 3). The lowest daily dose taken was 200 IU and the highest daily dose taken was 8000 IU. Some patients received a weekly dose as opposed to daily. The lowest weekly dose taken was 5000 IU (∼714 IU daily) and the highest weekly dose taken was 50 000 IU (∼7140 IU daily; Table 3).
Commonly Prescribed Vitamin D and Calcium Doses.
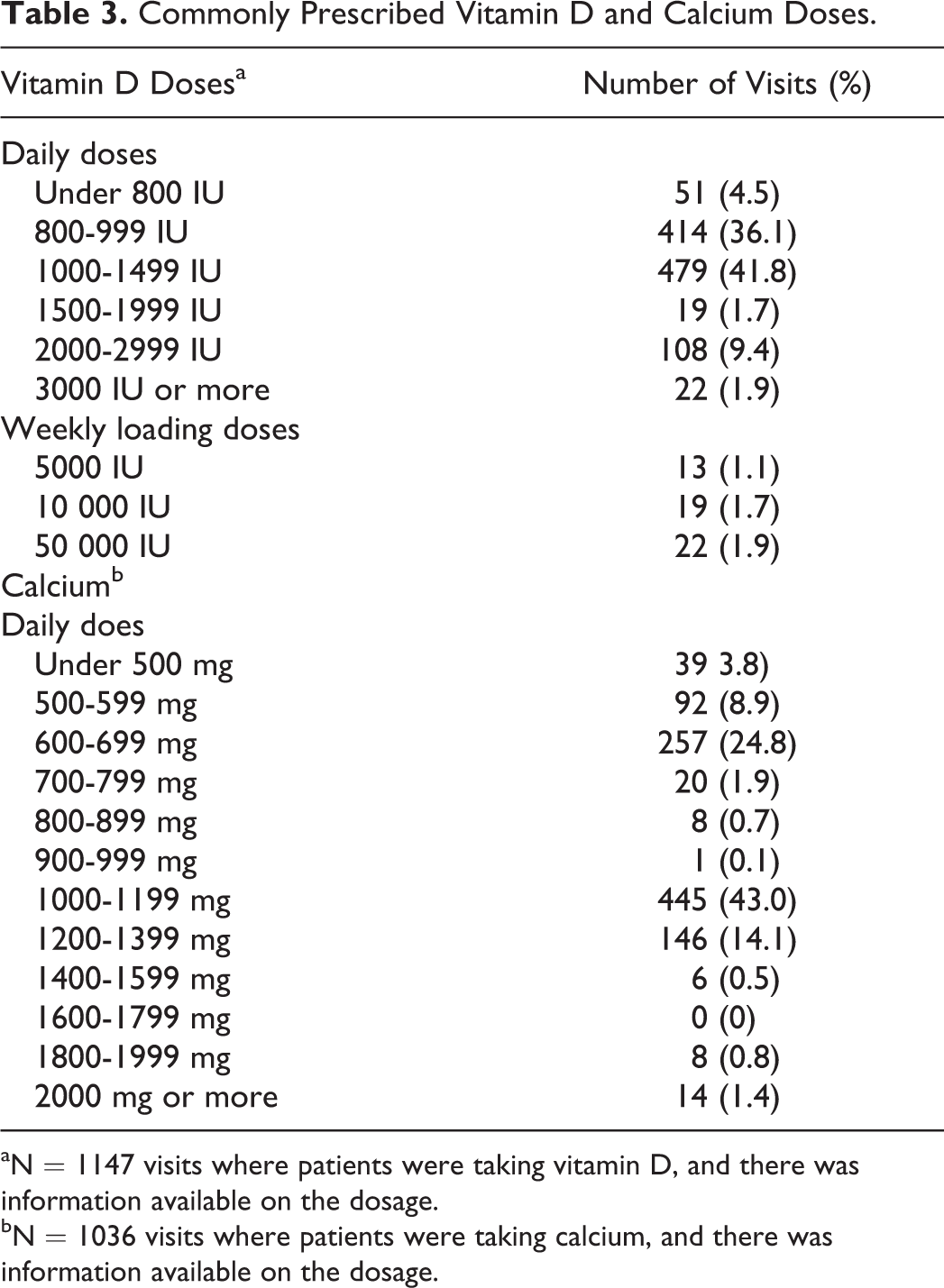
aN = 1147 visits where patients were taking vitamin D, and there was information available on the dosage.
bN = 1036 visits where patients were taking calcium, and there was information available on the dosage.
Of the patients who took calcium at 1 visit or more, 26 different doses of calcium were identified. The most common doses of calcium included 1000 mg (445/1036 visits) and 600 mg (246/1036 visits; Table 3). The median daily dose taken was 1000 mg (Q1-Q3: 600-1000 mg). The lowest dose taken was 100 mg and the highest dose taken was 3800 mg (Table 3).
Vitamin D and Calcium Prescribing and Management Patterns
Twelve (22.6%) sites reported having a comprehensive care pathway or protocol to follow for each patient presenting to hospital with a fragility fracture. Comprehensive pathways, such as Fracture Liaison Services, 20 included prescribing/recommending calcium and vitamin D to each patient as well as a plan of referral and/or investigation and patient education. Two of these sites (34 included patients) are Fracture Liaison Services. Twelve (22.6%) sites reported having a noncomprehensive protocol to follow for patients with fragility fracture. These noncomprehensive strategies included only prescribing/recommending calcium and vitamin D or only referring patients with fragility fracture to a specialist or following a protocol inconsistently or on a case-by-case basis. Twenty-nine (54.7%) sites reported that they do not follow a standardized protocol or their fragility fracture management procedure is unknown (Table 4). Vitamin D was prescribed/recommended to 456 fragility fracture patients (456/603, 75.6%) at the postoperative visit, while calcium was prescribed/recommended to 435 fragility fracture patients (435/603, 72.1%) at the postoperative visit (Table 1).
Clinical Site Characteristics.

Factors Associated With Consistency of Vitamin D and Calcium Supplementation
Compared to nonusers, consistent users of vitamin D were more likely to be from North America (OR: 20.232; 95% CI: 10.894-37.728), to be prescribed or recommended vitamin D postoperatively (OR: 5.938; 95% CI: 3.325-10.605), and to be treated at a site with a management protocol for fragility fractures (OR: 11.117 for comprehensive protocols and OR: 4.054 for noncomprehensive protocols compared to no/unknown protocol). Compared to nonusers, inconsistent users of vitamin D were more likely to be from North America (OR: 17.752; 95% CI: 9.410-33.490), to be prescribed or recommended vitamin D postoperatively (OR: 3.269; 95% CI: 1.844-5.794), and to be treated at a site with a management protocol for fragility fractures (OR: 8.286 for comprehensive protocols and OR: 2.975 for noncomprehensive protocols compared to no/unknown protocol). Age and sex were not associated with consistency of vitamin D use (Table 5).
Factors Associated With Inconsistent Use of Vitamin D and Consistent Use of Vitamin D Versus No Use of Vitamin D.

Abbreviation: CI, confidence interval.
We identified a similar trend for calcium use. Compared to nonusers, consistent users of calcium were more likely to be female (OR: 1.815; 95% CI: 1.058-3.114), from North America (OR: 13.156; 95% CI: 7.409-23.361), and to be prescribed or recommended calcium postoperatively (OR: 4.788; 95% CI: 2.775-8.263). Compared to nonusers, inconsistent users of calcium were more likely to be from North America (OR: 13.778; 95% CI: 7.706-24.638), to be prescribed or recommended calcium postoperatively (OR: 2.705; 95% CI: 1.600-4.574), and to be treated at a site with a management protocol for fragility fractures (OR: 8.819 for comprehensive protocols and OR: 3.259 for noncomprehensive protocols compared to no/unknown protocol). Age was not associated with consistency of calcium use (Table 6).
Factors Associated With Inconsistent Use of Calcium and Consistent Use of Calcium Versus No Use of Calcium.

Abbreviation: CI, confidence interval.
Osteoporosis Medications
Forty-four (7.3%) patients were taking bisphosphonates and 20 (3.3%) patients were taking other medications to treat osteoporosis at baseline. At the first study follow-up visit after surgery, 43 (7.1%) patients were taking bisphosphonates and 14 (2.3%) were taking other medications to manage osteoporosis. Of patients who were taking bisphosphonates or another medication to manage at baseline, approximately half were consistent users of calcium (32/64; 50%) and vitamin D (34/64; 53%).
Discussion
Despite evidence that vitamin D and calcium intake are beneficial for the prevention of refracture in patients who have fragility fractures, our study found that more than one-third of elderly hip fracture patients treated with arthroplasty did not take vitamin D or calcium within the first 12 months after their fracture. An additional one quarter took vitamin D and calcium inconsistently. Patients treated in North America, prescribed calcium and/or vitamin D postoperatively, and who were treated at clinical sites with a comprehensive fragility fracture management protocol were significantly more likely to consistently take calcium and/or vitamin D after hip arthroplasty. Female patients were also more likely to take calcium than males, but not vitamin D. The dosing regimens of both calcium and vitamin D are highly varied, showing a lack of consensus on the optimal dose. A slightly higher proportion of patients taking medications to manage osteoporosis were consistent users compared to patients not on bisphosphonates or osteoporosis medications.
These results are relatively consistent with a recent study on vitamin D supplementation among elderly patients undergoing internal fixation for a hip fracture, 18 although the internal fixation study found a slightly higher rate of consistent vitamin D use (46%) than our study. The similar study in internal fixation of hip fractures 18 also found that patients in North America are more likely to take vitamin D consistently, which is also congruent with our findings. The results of the current study show that there is large variability in dosing regimens of calcium and vitamin D. This is similar to a recent survey of American and Canadian orthopedic surgeons which found that 65% orthopedic surgeons routinely prescribe vitamin D to their fragility fracture patients. 12 In our study, nearly three quarters of patients were prescribed calcium and vitamin D while in hospital, but fewer patients reported taking calcium and vitamin D at study follow-up visits. A 1-year supply of calcium and vitamin D tablets ranges from CAD$20 to CAD$60 depending on brand name and daily dose, making it a very inexpensive medication. This study highlights an issue with compliance of even simple, inexpensive, and widely available medications, which should be taken into consideration when treating elderly orthopedic patients. We also found a very low rate of prescription (10.6% at baseline and 9.5% at the first study follow-up) of bisphosphonates and other osteoporosis medications in this population of fragility fracture patients. It is unknown why the rate of prescription of these medications was so low in this population, but it may point to a gap in care in geriatric orthopedics that should be addressed in future research. There is an opportunity to improve both the rate of prescription/recommendation and supplement adherence to ensure that patients with osteoporosis are getting the care that is needed to manage their osteoporosis and to prevent future fragility fractures.
It should be noted that, for patients who have high dietary calcium intake, supplementation is not required. In fact, it is more desirable for patients to obtain their calcium through diet than through supplementation. 21,22 However, relatively few hip fracture patients have adequate dietary calcium intake and therefore need supplementation. Health Canada reports that elderly men older than 70 years are getting 69% less calcium than the current recommendation and elderly women are getting 63% less calcium than recommended. 23 Clinical practice guidelines, hospital protocols, and educational programs for prevention of fragility fractures should reflect this.
Physicians should monitor patients who are taking vitamin D and/or calcium for possible side effects. Specifically, patients taking high doses of vitamin D should be carefully monitored for falls, 24,25 hypercalcemia, hypercalciuria, 26 and gastrointestinal distress. 10 Additionally, patients taking calcium may be at an increased risk of renal calculi, kidney stones, and negative cardiovascular effects, especially if they have cardiovascular, gastrointestinal, and kidney conditions. 27
This study is strengthened by the inclusion of a large number of participants from diverse clinical sites in 7 countries. Additionally, the prospective nature of the study allowed us to capture data with little risk of recall bias. Limitations of this study include possible underestimation of the loading doses of vitamin D taken as we did not specifically ask clinical sites to record loading doses. Additionally, clinical sites had to rely on self-reported use of calcium and vitamin D, which may be an overestimate or underestimate of actual calcium and vitamin D intake. We did not ask sites to specify whether the vitamin D was vitamin D2 or D3, so that information is unknown. Additionally, we did not record whether patients’ vitamin D levels were being monitored or whether they were referred for any additional management of osteoporosis. Monitoring can have an effect on compliance levels.
Despite well-developed guidelines, a low proportion of elderly hip fracture patients are consistently taking vitamin D and calcium, which may be contributing to poorer bone health and a missed opportunity to reduce the high refracture rate in this cohort. The inconsistency in patient use of calcium and vitamin D found in this study highlights a need for additional high-quality studies to establish a consensus on the ideal dosing regimen for vitamin D and calcium. In addition, patient education strategies along with surgeon educational initiatives and resources are needed to ensure that hip fracture patients receive bone health management beyond fracture care. Our study shows that hip fracture patients, who are the group at highest risk of future hip and other fragility fractures, frequently do not receive sufficient vitamin D and calcium. These patients and their treatment teams should be specifically targeted in future strategies for interventions aimed at fracture prevention.
Footnotes
Appendix A
Steering Committee: Mohit Bhandari (Chair), P. J. Devereaux, Thomas A. Einhorn, Lehana Thabane, Emil H. Schemitsch, Ken Koval, Frede Frihagen, Rudolph W. Poolman, Kevin Tetsworth, Ernesto Guerra-Farfán, Stephen D. Walter, Gordon H. Guyatt. Global Methods Centre: Mohit Bhandari, Sheila Sprague, Kim Madden, Paula McKay, Kerry Tai, Taryn Scott, Marilyn Swinton, Diane Heels-Ansdell, Lisa Buckingham, Aravin Duraikannan (McMaster University). US Methods Centre: Thomas A. Einhorn (principal investigator); Heather Silva (research coordination; Boston University Medical Center). Thomas A. Einhorn, Pankajkumar Patel (New York University). Netherlands Methods Centre: Ydo V. Kleinlugtenbelt, Ellie B. M. Landman (Deventer Ziekenhuis; Definitive). Martin J. Heetveld, Rudolf W. Poolman, Esther M. M. Van Lieshout, Paul T. P. W. Burgers (Erasmus Medical Centre, Rotterdam; Pilot). United Kingdom Methods Centre: Amar Rangan (The James Cook University Hospital, South Tees Hospitals NHS Foundation Trust, University of Oxford, University of York), Birgit Hanusch, Lucksy Kottam (The James Cook University Hospital, South Tees Hospitals NHS Foundation Trust). Central Adjudication Committee: Mohit Bhandari (Chair), Robert D. Zura, Victoria Avram, Ajay Manjoo, Dale Williams. Data Safety Monitoring Board (CIHR): John Antoniou (Chair), Tim Ramsay, Earl R. Bogoch, Andrew Trenholm. Data Safety Monitoring Board (NIH): Stephen Lyman (Chair), Madhu Mazumdar, Kevin J. Bozic, Mark Luborsky, Stuart Goodman, Susan Muray, Benjamin K. Potter.
Authors’ Note
Trial registration: NCT00556842. The funding sources had no role in design or conduct of the study; the collection, management, analysis, or interpretation of the data; or the preparation, review, or approval of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research grants were received from the following: Canadian Institutes of Health Research (PI: M. Bhandari, Co-PI: G. H. Guyatt and P. J. Devereaux), National Institutes of Health (PI: T. A. Einhorn), ZorgOnderzoek Nederland-medische wetensehappen (ZonMw) (PI: E. M. M. van Lieshout), Sophies Minde Foundation for Orthopaedic Research (PI: L. Nordsletten and F. Frihagen), and McMaster Surgical Associates (PI: M. Bhandari). Dr Bhandari was also funded, in part, by a Canada Research Chair in Musculoskeletal Trauma which is unrelated to the present study (McMaster University, Hamilton, Ontario, Canada).