
Abstract
Introduction:
Although electrotherapy appears to have particularly interesting applications in the field of postoperative orthopedic rehabilitation, relatively little scientifically based research has been conducted in the area of electrotherapy with regard to safety involving patients with orthopedic implants.
Method:
Three electrotherapy forms were tested, such as high-volt stimulation (HVS), transcutaneous electric nerve stimulation (TENS), and galvanic current (GAL), using a model system containing a metal implant plate to evaluate whether heating in excess of 3°C would occur.
Results:
All changes in temperature for HVS, GAL, and TENS therapeutic electrical currents observed in our model system fall below the predefined 3°C.
Conclusion:
To the best of our knowledge, this is the first experimental based observation that prolonged exposure to a direct electrical current at therapeutic strength does not result in heating of metal titanium plates.
Introduction
Several recent reviews have highlighted the importance of electrotherapy as an effective tool in pain management. 1-5 Conditions associated with geriatric populations in particular chronic pain, 5 low back pain, 2 and osteoarthritis have been shown to be effectively treated by electrotherapy. 1 In addition, the American Physical Therapy Association currently recognizes the utility of electrotherapy for pain management, treatment of neuromuscular dysfunction, inducing tissue repair, resolving acute and chronic edema, increasing peripheral blood flow, and iontophoresis. 6 Iontophoresis is of particular interest to researchers as it is the form of electrotherapy, which uses a unidirectional galvanic current (GAL) to transfer pharmaceutically active ions (electronically charged molecules) across the skin membrane. 7-9 This can be considered a form of needleless injection. Based on the principle of like charges repelling, pharmaceutically active ions being placed under similarly charged anodes or cathodes are repelled with the application of the GAL electrical current. This method is primarily used for the delivery of anti-inflammatory medications. 9 Other popular forms of electrotherapy such as high-volt stimulation (HVS) and transcutaneous electrical nerve stimulation (TENS) are also widely used. The HVS is used for the stimulation of wound healing, edema resolution, and pain relief, whereas TENS is primarily used for pain relief. Some forms of TENS have also been shown to aid in edema resolution. 9
Although electrotherapy, especially iontophoresis, appears to have particularly interesting applications in the field of postoperative orthopedic rehabilitation, relatively little scientifically based research has been conducted with regard to safety involving patients with orthopedic implants. A PubMed search given the keywords such as orthopaedic implant and electrotherapy resulted in only 21 hits, as of August 2015. Although a conference proceeding and a journal article discussed the use of neuromuscular electrical stimulation to reduce the incidence of deep vein thrombosis in postoperative total hip and knee arthroplasty patients, it simply reported metallic implant did not give rise to hypersensitivity judged by patient reports of comfort on a visual analogue scale. 10 Few reports exist relating to the use of electrical currents as a sterilization procedure for both titanium and surgical stainless steel before implantation. However, no data with regard to modeling of the in vivo heating of implants in the presence of therapeutic levels of electrical currents were found. 11,12
General guidelines as to the indications and contraindications with regard to the use of HVS, TENS, and GAL in the presence of orthopedic implants are available from the relatively limited number of physical therapy textbooks, electrotherapy machine manufacturer user manuals, and forums on the Internet that deal with this topic. 7-9,13 Although these sources offer basic information and guidelines for use, they lack citations and appear to be opinion based rather than founded in experimental evidence. It has been reported that conductivity and current path may be much higher for plates located immediately subcutaneously. 12 Data regarding physical properties such as conductivity exist for biological and implant materials. We were, however, unable to find literature that evaluated the heating of implants in in vitro or in vivo systems. The conductivity of titanium, a common implant material, is 1.76 × 106 S/m. Although titanium is a much better conductor than other biological tissues such as bone and muscle (conductivities 1.70-1.72 × 10−1 S/m and 1.50-6.00 × 10−1 S/m, respectively), the overall conductivity when compared to a good conductor such as copper (conductivity 58.5 × 106 S/m) is low. 14-16 One would expect heat storage in vivo to be minimized by transfer and cooling by the circulatory system. A recent report on the effects of low-dose microwave on healing of fractures with titanium alloy internal fixation for an in vivo animal model showed microwave treatment caused no significant heat damage in tissues around implants, and no statistical increase in temperature was observed. 17 Although microwave radiation and the HVS, TENS, and GAL currents are very different, this report highlights the need for further study of electrotherapy in vivo and the need for preliminary research to justify or invalidate current clinical recommendations with regard to use.
The purpose of the following study is to establish whether heating of a model system occurs in the presence of an orthopedic implant. Due to the conductivity of materials used for orthopedic implants and the promising early reports of no microwave therapy associated heating for in vivo models, 17 we propose that heating in the presence of an orthopedic implant using electrotherapy will be minimal. The 3 electrotherapy methods selected, such as HVS, TENS, and GAL, cover the range of safe recommended to potentially dangerous modalities. We were interested in comparing possible differences in heating between classical nonthermal modalities such as HVS and TENS and the unidirectional galvanic current used in GAL. As such, comparisons of relative heating from system to system should provide insight into the relative safety of each form. To the best of our knowledge, the following project is the first reported attempt to evaluate the heating of an orthopedic implant in the presence of HVS, TENS, and GAL electrical currents.
Materials and Methods
Apparatus
A diagram of the model system used is shown in Figure 1. The titanium implant plate, model number AR-2952TT-03 (Arthrex, Germany), was attached with cotton thread to a 1-cm thick cellulose sheet. Three additional sheets were used to secure the implant in the center of the 4 cm × 6 cm × 8 cm cell, and electrodes were placed on the inside of the cell. As the titanium implant plate studied was designed to be used in the foot, this cell size was deemed appropriate. To this, 20 mL of isotonic solution (5% w/vol NaCl) was added. The relatively small solution cell and limited amount of conducting solution were selected to minimize the loss of heat generated in the system. We propose this in vitro system, though simple should mimic the in vivo system as conductivity is similar. Temperatures were measured at given time intervals (0, 5, 10, 15, 20, 30, and 40 minutes) in 5 different positions. The probe positions for temperature collection A, B, C, D, and E are defined as follows—A is the point between the cathode (IONOSON-Jubilee-00654 Plattenelektrode EF50 8 cm × 6 cm; Physiomed, Germany) and the first cellulose sheet in the geometric center of the cathode, B also positioned in the center of the electrode but 1 cm closer to the anode. Points C, D, and E are located 2, 3, and 4 cm closer to the anode (IONOSON-Jubilee-00653 Plattenelektrode EF50 8 cm × 6 cm; Physiomed), respectively. The probe positions vary in distance from the implant at 1 cm intervals, with a temperature probe C being taken directly at the site of metal implant attachment. The temperature was measured with a Thermomax AVAX DT-7 Digital thermometer (measurement range −50°C to +300°C, resolution 0.1°C, precision 1°C, power voltage DC 1.5 V; AVAX, Germany). Precision of the temperature probe was tested and found to agree with manufacturer specifications. To ensure no heating of the conductive material in the thermometer, during temperature measurements, the electrical current was disconnected from the machine at the electrode outlet base of the source used. The current source, a IONOSON Jubilee model number ISJ2-1209708 (Physiomed), was used at various current strengths.

Schematic representation of sample cell containing orthopedic implant.
Selection of Electrotherapy Currents
For a preliminary evaluation of 3 electrotherapy forms, HVS, TENS, and GAL were selected. Test parameters used are summarized in Table 1. The HVS has been reported safe for use in patients with orthopedic implants, as has TENS due to the lack of direct continuous current. There is some concern as to the safety of GAL with orthopedic implants as a direct current used. Fear exists that this direct current focused on a metal implant could result in spot heating due to the storage and transfer of electricity to heat at the metal site in vivo.
Therapeutic Currents Evaluated.
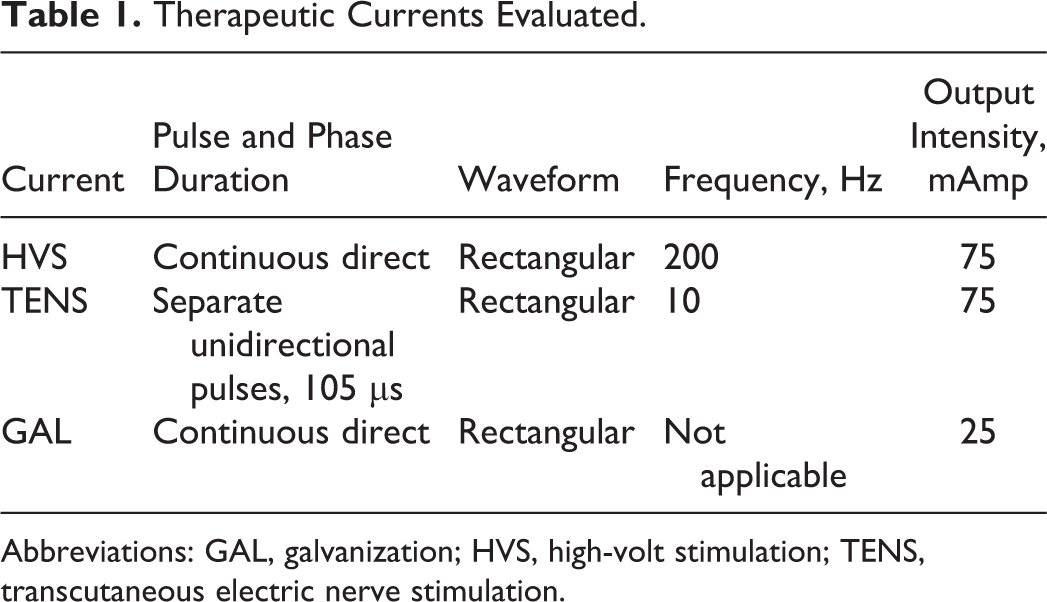
Abbreviations: GAL, galvanization; HVS, high-volt stimulation; TENS, transcutaneous electric nerve stimulation.
Although therapeutic uses of electrical currents, particularly GAL, would differ from individual to individual based on pain tolerance, the currents tested were the maximum output available on these machines. The maximum current density advised for iontophoresis is dependent on electrode size 0.5 mA/cm2. 8 To test potential heating, we used a current density 10 times this maximum and twice as long (40 minutes) as typical 20 minutes therapy times commonly used for iontophoresis. This extreme energy input was used to evaluate the risk of overheating based on the idea that if no heating was seen for these extreme GAL conditions, clinically relevant heating in standard therapeutic conditions would be highly unlikely. A lack of heating using the GAL current in our simple model would suggest that further study with a more complex system should be undertaken and may be indicative that iontophoresis is a viable treatment option for patients with orthopedic implants.
Statistics
Mean and standard deviation (SD) were used to compare and evaluate trends in data observed. Microsoft Excel (version 14.4.0) and the Analyze-it add-in (version 2.21) were used to generate graphs shown. Furthermore, a detection limit was defined as 3°C, which was established using the standard signal to background noise ratio of 3:1. In our case, we can take the “noise” to be defined as the variance inherent to measurement with the thermometer 1°C, and as such say that any temperature increase over 3°C would be defined as a significant increase in temperature. As average human body temperature is 37°C to 38°C and fevers do not typically exceed 41°C, we considered the detection limit of a 3:1 signal-to-noise ratio appropriate for our model system as this would also be the maximum physiological temperature range expected (41°C-38°C = 3°C). 18-20
Results
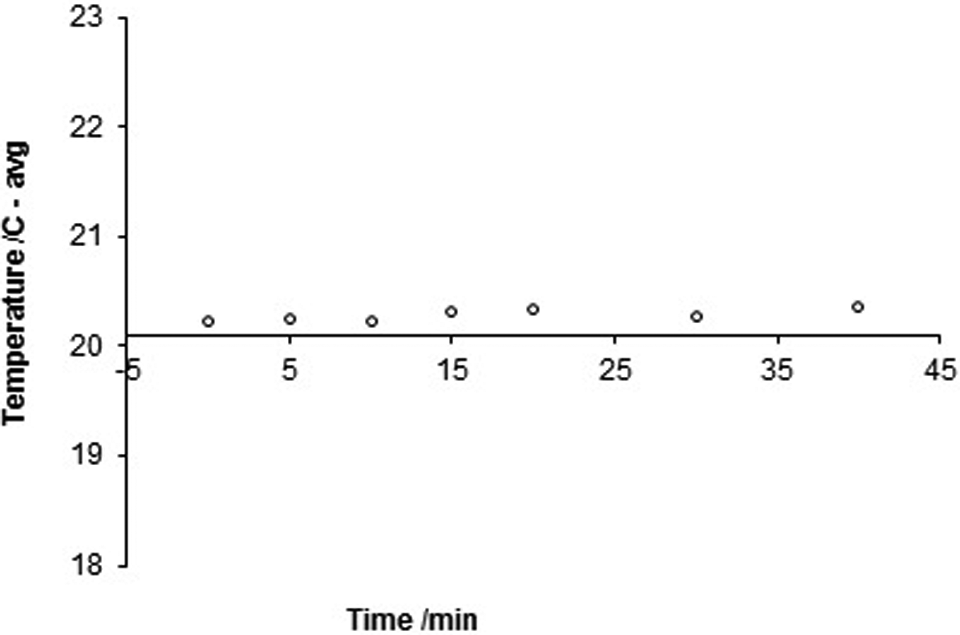
Tables 2 to 4 show the temperatures measured at various time points (0-40 minutes) and probe locations (A-D), as well as the mean temperatures for each time point (avg) and the respective SDs. Graphs of mean temperatures versus time are depicted in Figures 2 to 4. All changes in temperature observed fall below the relevant signal to background noise ratio previously defined. Hence for the system studied, prolonged exposure to any of the 3 electrical currents investigated does not result in heating of the model system studied within the range of sensitivity of the measurement instruments used.
Temperature Measurements From Probe Locations for Given Times With the Sample Cell and Implant System When Using a HVS Electrical Current.
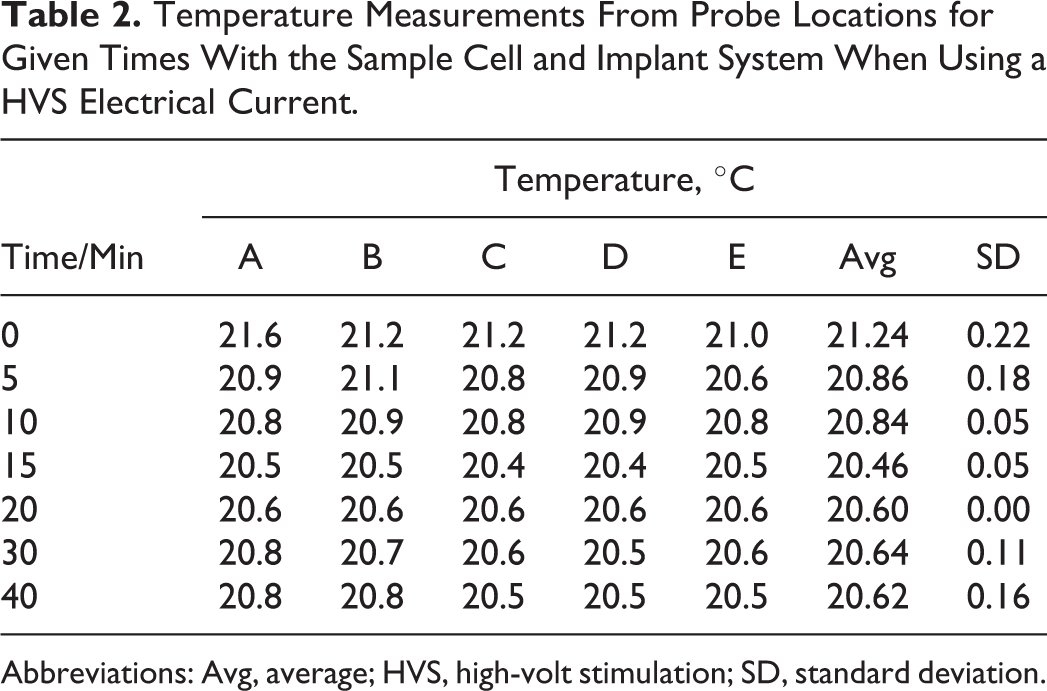
Abbreviations: Avg, average; HVS, high-volt stimulation; SD, standard deviation.
Temperature Measurements From Probe Locations for Given Times With the Sample Cell and Implant System When Using a TENS Electrical Current.

Abbreviations: Avg, average; SD, standard deviation; TENS, transcutaneous electric nerve stimulation.
Temperature Measurements From Probe Locations for Given Times With the Sample Cell and Implant System When Using a GAL Electrical Current.

Abbreviations: Avg, average; GAL, galvanization; SD, standard deviation.

Average temperature versus time for the sample cell and implant system when using a high-volt stimulation (HVS) electrical current.

Average temperature versus time for the sample cell and implant system when using a transcutaneous electric nerve stimulation (TENS) electrical current.
Average temperature versus time for the sample cell and implant system when using a galvanization (GAL) electrical current.
Discussion
Outlook and Clinical Implications
The use of electrotherapy in the field postoperative orthopedic rehabilitation with direct current could be a valuable tool. Iontophoresis and edema resorption are the 2 techniques in modern physiotherapy that could aid greatly in postoperative recovery. The lack of information with regard to the safety of use is surprising. Although there is little published in this area, we feel that the use of electrical currents is particularly attractive as elimination of medications would reduce medication interactions and side effects for pain management and edema reduction. Our preliminary investigations suggest that heating at the implant site is nonexistent. The concerns with regard to use of direct currents are therefore unfounded. Further work should be done with more complex models to confirm these findings.
Limitations
Although these preliminary results are promising, one must not understate the need for further experimentation and optimization of the model system. Particular limitations to the system studied include the sensitivity of temperature measurement and the nonphysiological parameters used in testing. The system was open and not insulated, which could account for the very slight loss of temperature over time (<1°C). Holding the temperature of the in vitro model steady with heating or using a closed system would interfere, most likely falsely minimize the effects of measurement of temperature changes with the presence of an electric current. The use of an electrolytic solution in direct contact with the anode and cathode may provide exaggerated heating as a skin barrier in an in vivo model would be expected to more poorly conduct electricity. Through the use of a simple, cost-effective, easy to reproduce model, we hope to encourage other groups to use our system as a preliminary model and expand and improve upon it further. We also hope our model can be used by groups with enhanced expertise and facilities as a preliminary screening model, before moving on to testing with animal models. Testing in this area should continue, and developments should be made to further optimize the apparatus to more closely mirror actual physiological conditions. In vivo tests with animal models should be considered. One must not directly correlate spot heating in this modified system as a direct representation of an in vivo implant as the body undergoes exchange of fluid within the system in the form of blood flow. Current test conditions do however provide an upper limit of expected heating near an implant in conducting media that provides useful information for efficient selection of electrical therapy for patients with orthopedic implants.
Conclusion
These preliminary investigations concerning the heating of orthopedic implants in a direct therapeutic current suggest that heating about the implant site, for an implant made of titanium, is minimal. The use of electrotherapy in the place of biologically active chemical compounds could reduce possible drug interactions and side effects due to reduced or absent doses of medicines used. Although of interest for all patient groups, this would be particularly useful to geriatric orthopedic patients who may have multiple disease, have compromised organ function, or currently be on medications that could interact with medications given postoperatively to help combat pain and swelling. We hope this preliminary report encourages other health-care professionals to undertake research in this exciting area.
Footnotes
Acknowledgments
Dr Robert Kilger is kindly thanked for supplying our research group with the orthopedic implant tested.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.