
Abstract
Radicular lumbar pain is a widespread condition characterized by nerve dysfunction. Many treatments have been proposed over time for its management, ranging from surgery to conservative approaches. The combined application of multiple transcutaneous electrotherapies may be a valid approach for the condition; however, the evidence supporting it is currently weak, as most proposed application protocols are often lacking in detail and replicability. A case series of seven patients (mean age 65 ± 9 years) was conducted to observe their response to a specific non-invasive multimodal transcutaneous electrotherapy protocol, monitored through pain and perceived disability rating scales and postural assessments. Patients showed a general improvement in the monitored parameters, particularly the painful component of the condition. The proposed protocol appears effective and merits further, more in-depth studies, while it continues to be successfully applied in the management of patients with radicular lumbar pain.
Keywords
Introduction
Radicular lumbar pain (RLP) is a widespread musculoskeletal condition, which is estimated to be affecting from 13% to 40% of the population globally. 1 It is characterized by neuropathic pain caused by a pathology of the sensory lumbar nerve roots, resulting in symptoms like sensory disturbance, paresthesia, and motor deficit. 1 RLP appears to be a consequence of morphological variations of the tissues and anatomical structures crossed by the nerve roots emerging from the lumbar spine, 1 as in the case of herniated discs, lumbar spinal stenosis, and other non-skeletal causes like infections or neoplasms. 1
The diagnosis is typically based on clinical tests, pain mapping, and instrumental investigations such as computed tomography and magnetic resonance imaging. 2 The management of RLP is multidisciplinary, based on a conservative approach consisting of exercise, education, local applications, and pharmacological therapy 2 ; invasive and surgical approaches should be limited to cases where conservative therapy fails. 2 However, treatment guidelines for RLP are heterogeneous and often unable to draw definitive conclusions, especially on instrumental therapies, such as electrotherapy, phototherapy, and thermotherapy. 2
Electrotherapies would appear to be a potentially valid approach for nervous disorders.3,4 Some reviews have highlighted how peripheral nerve stimulation would appear to be useful for musculoskeletal and neuropathic pathologies, albeit with conflicting levels of evidence and multiple methodological limitations.3,4 Percutaneous and transcutaneous peripheral applications of electrical nerve stimulators appear to prove useful as a non-invasive approach to various pathologies.3,5
Although transcutaneous nerve stimulation appears to have healing and regenerative effects on nervous structures, 6 determining the best administration method between percutaneous and transcutaneous for this type of treatment (and with which current parameters) remains challenging. 7 However, the non-invasive nature of transcutaneous neuromodulation and microcurrents therapy suggests further investigation of these approaches, to fully disclose their clinical relevance, especially when combined.7,8 In fact, it has been highlighted how different types of current can produce different types of therapeutic effects at the level of nervous tissue, such as proliferation of Schwann cells and macrophages, inhibition of inflammatory factors, increase of regenerative factors, and reversal of the genesis of neuropathic processes. 9
In general, various forms of electrotherapy, such as transcutaneous electrical nerve stimulation, interferential currents, microcurrents, and peripheral neuromodulation, have proven to be effective analgesic tools in pain contexts, such as musculoskeletal, neuropathic, and oncological pain. However, to date, the correct application methodology of these techniques and the possible combination of multiple types of currents still represent a limitation in this area of research.10–13 Therefore, the objective of this study is to explore the therapeutic potential of an innovative approach combining transcutaneous neuromodulation and microcurrent therapy in the management of RLP. This study aims to detail the application method as much as possible, thus laying the foundation for a rational and repeatable operating method that could expand and evolve the emerging research field of combined electrotherapies in rehabilitation, while also defining the basic short-term safety profile of this new therapeutic application.
Materials and methods
This study is a case series carried out at the Center for Physiotherapy, Rehabilitation and Re-Education (Ce.Fi.R.R.) venue “G. d’Annunzio” University of Chieti-Pescara, Italy, from June to September of 2024. All applied procedures comply with the Italian safety regulations and the protocol is not an experimental practice. The study lines with the applicable ethical principles of the Declaration of Helsinki. Written informed consent was collected from participants. Due to all previous considerations and the lack of specific national laws stating the need for the submission of retrospective and/or non-pharmacological observational studies to an ethics committee, 14 external ethical approval was not required. However, to ensure high ethical and procedural standards for studies conducted inside the institution, the Ce.Fi.R.R. relies on the ISO 9001:2015 accreditation for the implementation of observational clinical studies in the rehabilitation field (ACCREDIA Certificate No. IT15/0304). The study was conducted in accordance with the applicable CARE EQUATOR Network reporting guidelines.
We observed seven patients affected by moderate intensity RLP during the period of the study. Patients were diagnosed with RLP at the study site by specialists in rehabilitation medicine, anesthesiology, or rheumatology. The diagnosis was based on the presence of moderate lumbar pain (numeric pain rating scale (NPRS) ⩾3), irradiated on at least one of the two limbs, according to the appropriate pain mapping criteria, in combination with positivity to tests performed by physicians (Wasserman test, Lasegue test, muscle palpation, grazing for the investigation of superficial sensitivity). 2 To be referred to the standard non-invasive multimodal transcutaneous electrotherapy (N-IMTE) treatment, patients had to not present typical contraindications for treatment with electrotherapies, such as cancer, pregnancy, electronic implants, epilepsy, infections, serious vascular and cardiac diseases, and severe neurological impairments. Additionally, subjects with a suspected potential allergy to the conductive glue of electrodes for transcutaneous electrical applications were not considered suitable for the application of N-IMTE.
Since the patients studied were not using NSAIDs Nonsteroidal Anti-Inflammatory Drugs (NSAIDs), steroids, or opioids to control pain at the time of admission, they continued to avoid pharmacological treatment for the entire duration of the study, considering that they were under medical monitoring, and they should have started the N-IMTE treatment.
Recruited patients were indicated by the evaluating physicians to undergo between 5 and 10 applications of N-IMTE, lasting approximately 30–45 min, within a 2-month period. The individual number of sessions was determined based on the availability of each patient to reach the study center for the treatment prescribed.
The non-invasive assessment of patients was performed using reliable and quickly applicable evaluation tools:
NPRS: 10-point monodimensional self-administered scale for the assessment of perceived general pain. 15
Brief pain inventory (BPI): multidimensional self-administered scale to evaluate intensity (four items) and interference (seven items) of the pain experienced. 16
Oswestry disability index (ODI): 10-section self-administered questionnaire aimed at assessing disabilities in subjects suffering from low back pain. 17
Right-to-left foot load difference (LOAD Δ%) and postural biometric index (PBI): respectively, plantar load values and postural quality score detected using a computerized stabilometric platform (Diasu Health Technologies, Rome, Italy).18,19
Assessments were performed immediately before the start of the first session and after the end of the last session. For operational reasons, all assessment tools were administered by the same therapist who performed the treatment. However, all the assessment scales used had standard written instructions and were self-administered by the patient, while the stabilometric-postural assessment was a standardized instrumental assessment. Therefore, the intervention of the therapist-evaluator in the assessments was limited to handing the scales to the patient and initiating the digital capturing of the stabilometric-postural setting, making his influence on the data collection essentially nonexistent, despite the lack of any actual blinding regarding the identity of patients and/or the nature of the treatment received by them. Furthermore, the collected data, once anonymized, were analyzed by a person other than the therapist-evaluator, to avoid any potential interference in the data curation process.
The N-IMTE protocol was performed using the PONOS device (AD Swiss MedTech SA, Gravesano, Switzerland; donated to the study site on a non-profit basis by: a circle S.p.A., San Pietro in Casale, Italy). Patients were all treated by the same therapist, under standard conditions.
N-IMTE consists of the application of a neuromodulation current (damped biphasic sinusoidal waveform, variable repetition interval, and adjustable intensity in mA) set according to the individual perception threshold of the patient (i.e., tingling sensation under the applicator and eventual electrical discharge all along the target nerve) combined with the static application of microcurrents (positive square waveform, variable frequencies, and adjustable intensity in µA). The neuromodulation mode of the device has an impedentiometric feedback tool which registers the local electrical impedance (expressed in Ω) each time the current reaches the lowest and highest stimulation frequencies within the set reference range.
The anatomical sites of application of neuromodulation are shown in Figure 1. The phases of neuromodulation treatment are described in Table 1 and the application areas are shown in Figure 1. During the first session, as a strategy to accommodate the patient to the N-IMTE, the treatment was preferably concentrated near the sides of the spine. In subsequent sessions, the application was instead concentrated peripherally, especially along the limb(s) most affected by the RLP symptoms.

Visual representation of the anatomical application sites of N-IMTE. Specifically, the image shows an example of RLP application with irradiation along the left lower limb.
N-IMTE neuromodulation phases.

N-IMTE: non-invasive multimodal transcutaneous electrotherapy.
Definition and therapeutic target as indicated by the manufacturer.
Phase 1 application was focused on the four points where the electrical impedance was highest and unbalanced between the two frequencies, according to the device feedback. Phase 2 application was focused on the four points of greatest pressure pain manually identified by the therapist. Phase 3 application was focused on the four points of greatest symptomatic irradiation along the nerve pathway. For all the three phases, when the impedance value was reduced and equalized between 30 and 120 Hz on a treated area, the applicator was moved to the subsequent point.
Starting from the second session, simultaneously with the interactive neuromodulation, microcurrents were applied by placing four total PG473W 45 × 80 mm electrodes (FIAB SpA, Vicchio, Italy) on the body of the patients as follows: one on the spine level immediately above the dysfunctional one (channel 1 positive pole), one on the terminal area of RLP irradiation, typically under the foot (channel 1, negative pole), and one on each side of the spine at the spinal level affected by the pathology (channel 2, positive pole on the side opposite to the RLP irradiation and negative pole on the side of RLP irradiation). The anatomical sites of application of neuromodulation are shown in Figure 1. The microcurrents protocol is described in Table 2.
N-IMTE microcurrents protocol.
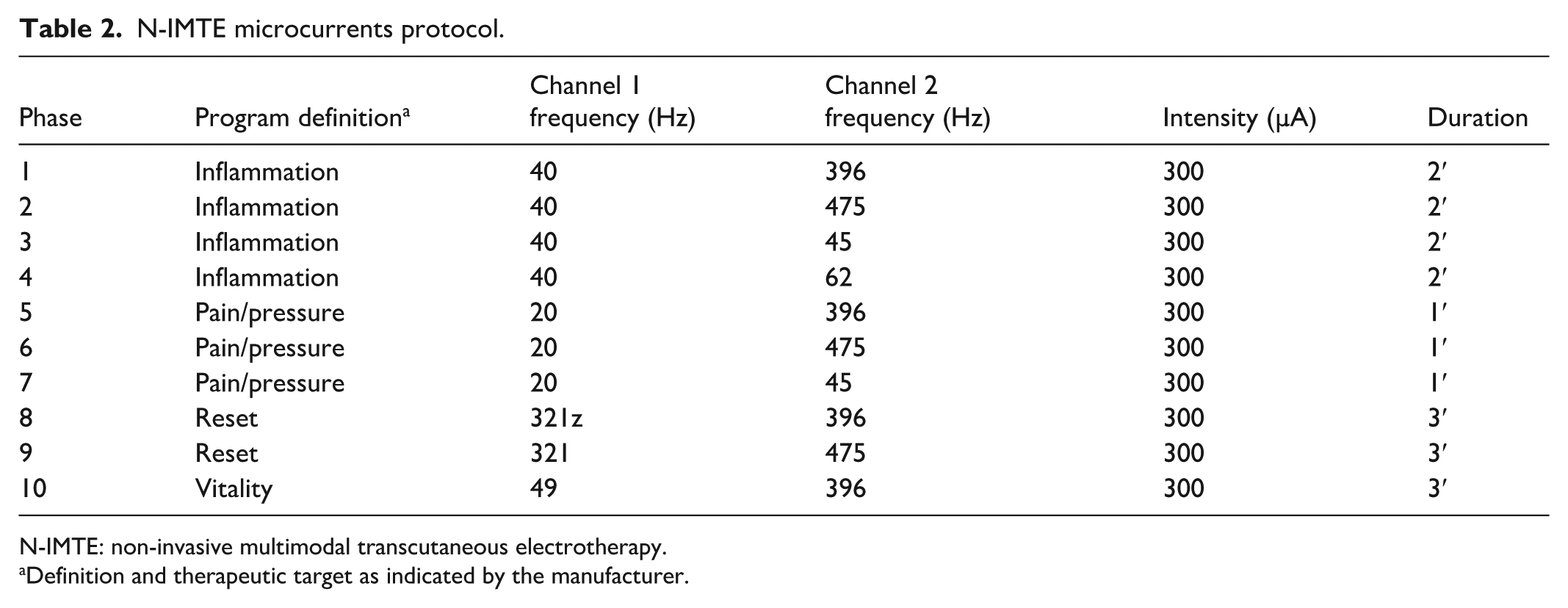
N-IMTE: non-invasive multimodal transcutaneous electrotherapy.
Definition and therapeutic target as indicated by the manufacturer.
The microcurrent protocol lasted 20 min in total. In case of bilateral RLP, the microcurrent application was repeated twice, once for each side of the lower body.
Statistical analysis was performed through the Statistics Kingdom online calculator (www.statskingdom.com). The distribution of the datasets was tested through the Shapiro–Wilk test, according to which BPI (intensity), BPI (interference), LOAD Δ%, and PBI data were normally distributed, while NPRS and ODI were not. Therefore, the analysis of the pre-post variations of the variables was carried out through the paired t–test for normally distributed datasets and through the Wilcoxon-signed rank test for non-normally distributed datasets. A value of p < 0.05 was set to determine statistical significance of the variations. The effect size (d/r) was also determined.
Results
Characteristics of the seven cases observed are indicated in Table 3. All patients reported having attempted NSAIDs use, with little or no success, to manage their moderate RLP prior to attending the study center.
Characteristics of the observed cases.

RLP: radicular lumbar pain; NPRS: numeric pain rating scale.
We observed significant improvements for all the evaluation scales (NPRS = −84.8%; BPI (intensity) = −53.9%; BPI (interference) = −49.2%; ODI = −54.4%; Table 4). However, the values regarding the postural arrangement underwent only slight non-significant improvements (LOAD Δ% = −31.8%; PBI = −13.6%; Table 4).
Values of the parameters observed for each patient at times T0 and T1 and statistical analysis of the variations.

NPRS: numeric pain rating scale; BPI: brief pain inventory; ODI: Oswestry disability index; PBI: postural biometric index; SD: standard deviation.
Means and standard deviations rounded to one decimal place, p-values and effect size values rounded to two decimal places.
All patients studied completed the planned treatment sessions, without reporting, in the form of an oral or written complaint, adverse events and without the need to make changes to the evaluation and treatment protocols. Furthermore, no significant negative skin reactions were observed at the treatment application sites, apart from a very modest redness, probably of hyperemic nature, which disappeared within a few minutes after the end of the sessions and was not associated with pain, burning, itching, or other unpleasant sensations on the part of the patient.
Discussion
Our study highlights how the N-IMTE is associated with significant improvements in pain and disability associated with RLP. However, no significant effects were highlighted on the postural quality of patients, even though this aspect has undertaken a trend of slight improvement. Furthermore, it should be highlighted that no observed case was associated with adverse reactions attributable to the treatment.
It is believed that conservative therapeutic approaches for radiculopathies must necessarily be evidence-based to guarantee results equal to or better than those of the surgical approach. 20 To define the validity of electrotherapies, it is necessary to study approaches characterized by a well-defined, adequately described and replicable methodology, also considering the technological advances in electromedical equipment. 21 The possibility of combining multiple non-invasive physical-instrumental approaches could exploit new and improved methods for rehabilitation, with a view to converging therapeutic approaches into specific multimodal devices.5,22
Developments in bioengineering have highlighted how electrical/electromagnetic neuromodulations appear to be powerful tools for controlling nervous pathologies. 23 Electrical/electromagnetic neuromodulation may promote neural regeneration and healing by controlling signaling in the nervous system: it is in fact capable of exciting, inhibiting, or regulating neuronal and neural network activities to improve motor function and the perpetuation of painful stimuli.23,24 Electrical/electromagnetic neuromodulation techniques appear to be effective in normalizing peripheral nervous activity by inhibiting aberrant descending reflexes, thus improving altered pain perception and motor function. 24 These neuroregulatory mechanisms could explain the effects obtained in our case series. In particular, it is possible that the positive effects we observed in relation to RLP are due to a summation of the therapeutic effects characteristic of the individual electrotherapy techniques applied. Transcutaneous neuromodulation techniques are characterized by an analgesic effect primarily due to the recruitment of Aβ sensory fibers, which act as a gate control on spinal segments when applied at the metameric level, accompanied by an effect on the descending inhibitory control pathways when applied to painful areas. 25 Furthermore, neuromodulation techniques also appear to affect the release and reabsorption of substances involved in pain modulation, such as substance P, glutamate, calcitonin gene-related peptide, norepinephrine, serotonin, gamma-aminobutyric acid, and endorphins. 26 Microcurrents, on the other hand, appear to act mainly through the modulation of inflammation associated with painful states, modifying the levels of cytokines interleukin-1, interleukin-6, tumor necrosis factor, and cortisol. 27 These anti-inflammatory effects are combined with tissue regenerative effects due to the ability of microcurrents to increase Adenosine Triphosphate (ATP) concentrations, protein synthesis, membrane transport, and peripheral blood circulation.28,29
To date, electrotherapies are far from enjoying a high level of recommendation, increasing the need for in-depth research on targeted and adequately detailed techniques, such as the proposed N-IMTE approach. 30 This is even more true considering that the combined applications of multiple forms of electrostimulation and physical energies, such as the observed protocol, could rationally offer more advantages than applications of single currents. 5 For example, some studies observed combined central and peripheral neuromodulation techniques. 31 Furthermore, it must be considered that microcurrents also, despite all the limitations of the evidence in question, would appear to be a valid tool for pain control and nerve regeneration.8,32,33 Microcurrent therapy is generally better tolerated than other forms of current,8,32 which makes them ideal for the creation of a non-invasive multimodal treatment system, such as the proposed N-IMTE.
We focused on the schematic and extensively detailed non-invasive application of a strictly peripheral multimodal electrotherapy, obtaining excellent and significant results in terms of pain and perceived disability. Furthermore, the results observed on posture, although not significant, are still characterized by a positive trend of improvement, confirming that techniques such as the N-IMTE are capable of simultaneously remodulating, albeit with different magnitudes and timing, both the painful and motor components of radiculopathies. The motor system and the perception of pain seems to be interrelated, to the point that the alteration of sensorimotor mechanisms, regulated by autonomic feedback, often underlies the genesis of chronic pain. 34
In any case, the limited number of cases allows only preliminary conclusions to be drawn on the proposed protocol. This case series allows us to confirm the therapeutic potential of the proposed N-IMTE approach, laying the foundations for more in-depth studies on the topic. Future studies should include a controlled experimental setting, more accurate evaluation methods (including electrodiagnostic and imaging methods 35 ), and a larger number of subjects, to define evidence regarding the indications for using the proposed protocol. In particular, it will be important to consider the possibility of making a comparison between the proposed N-IMTE treatment and typical RLP treatments, such as pharmacological or motor-rehabilitative treatments, also evaluating the possibility of studying how N-IMTE could interact with the aforementioned classic treatments from a complementary and integrative medicine perspective.
Conclusions
We conclude that the observed N-IMTE modality represents an interesting and safe therapeutic option in the control of symptoms associated with RLP.
This study represents an important starting point in defining new protocols for the application of transcutaneous and non-invasive forms of combined electrotherapies. The good results and the absence of adverse reactions observed in this case series would seem to suggest continuing the clinical application of the proposed N-IMTE protocol, possibly investigating it further with more in-depth and better structured studies to clarify the definitive level of evidence for its application.
Footnotes
Acknowledgements
Heartfelt thanks go to Dr. Matteo Marangi for assisting in the diagnosis and treatment indications for patients and to Mr. Maurizio Gioda, therapist and electrotherapy expert, whose theoretical and practical insights were important in conceptualizing this study.
Ethical considerations
Due to the protocol not constituting an experimental practice and the lack of specific national laws stating the need for the submission of retrospective and/or non-pharmacological observational studies to an ethics committee, ethical approval was waived. However, to ensure high ethical and procedural standards for studies conducted inside the institution, the Ce.Fi.R.R relies on the ISO 9001:2015 accreditation for the implementation of observational clinical studies in the rehabilitation field (ACCREDIA Certificate No. IT15/0304).
Consent to participate
Written informed consent was obtained from patients for publishing their anonymized information in this article.
Author contributions
GB, MPDR, VG, and MP designed and organized the study. MS administered the assessment tools and performed the treatments. GB, LP, MS, CDM, and PEG wrote the first draft of the manuscript. All authors reviewed, edited, and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All demographic and evaluative data collected during the study are presented in the article in an anonymous form for privacy reasons (see Tables 3 and ![]() ).
).