
Abstract
Introduction:
Hip fracture is the leading orthopedic discharge diagnosis associated with 30-day readmission in terms of numbers. Because readmission to the hospital following a hip fracture is so common, it adds considerably to the costs on an already overburdened health care system.
Methods:
Patients aged 65 and older admitted to a 261-bed university-affiliated level 3 trauma center between April 30, 2005, and September 30, 2010, with a unilateral, native, nonpathologic low-energy proximal femur fracture were identified from a fracture registry and included for analysis. Readmissions within 30 days of hospital discharge, costs, and outcomes were collected and studied.
Results:
Of 1081 patients, 129 (11.9%) were readmitted within 30 days. The average hospital length of stay for readmissions was 8.7 ± 18.8 days, which was significantly longer than the initial stay (4.6 ± 2.3 days) (P = .03). Nineteen percent (24 patients ∼19%) died during readmission versus 2.8% during the index admission. These patients accumulated an average hospital charge of US$16 308 ± US$6400 during their initial hospitalization for compared with charges for their readmissions of US$14 191 ± US$25 035 (P = .36).
Discussion:
Readmission was usually associated with serious medical or surgical complications of the original hospitalization.
Conclusions:
Readmission after hip fracture is costly and harmful. Charges were similar between the original fracture admission and the readmission. Patients were readmitted most frequently for medical diagnoses following their original hospital stay. Some of these readmissions may have been avoidable.
Introduction
The US Healthcare costs are assuming an increasing level of importance. Medicare expenditures for inpatient care are expected to increase from US$129.1 billion in 2008 to US$234.9 billion in 2019. 1 Approximately 19.6% of Medicare recipients are rehospitalized within 30 days following discharge from an acute care setting. 1,2 In 2010, the Patient Protection and Affordable Care Act (PPACA; P.L.-11-148) was signed into law in the United States. This law included provisions to reduce hospital readmissions. 1 Readmissions are very costly and considered to be “low hanging fruit” for cost-reduction efforts. 3 Hospital readmission is a complex problem with multiple etiologies, and there are no simple strategies to reduce their incidence. 2 Despite the complexity, readmission is seen as an important performance and accountability measure for hospitals. 4
Hospital readmission following hip fracture is a frequent and serious sentinel event that may be avoidable and may indicate a gap in care. 1,3 There is considerable regional variation in readmission rates according to recently published data. 1,3 Hip fracture is the leading orthopedic discharge diagnosis associated with 30-day readmission in terms of numbers. 3 Because readmission to the hospital following a hip fracture is so common, it adds considerably to the costs on an already overburdened health care system. 2,5,6 Readmission rates following hip fracture have increased slightly from 14.3% in 2004 to 14.5% in 2009. 3 Hip fracture has been shown to be the third most costly diagnosis in Medicare recipients aged 65 and older accounting for 4.6% share of total spending. 7
Most hip fractures occur in patients aged 65 years and older, which is the most rapidly growing segment of the population in the United States. 8 –10 An estimated 330 000 hip fractures occur yearly in the Unites States. 11 The number of hip fractures is predicted to increase by 51% by 2025. 12 With increasing number of patients treated and discharged, the associated economic impact of hospital readmission is also growing. This manuscript will analyze the costs of the initial inpatient admission, readmission, and 30-day hospital readmission rates of 1081 patients with a native nonpathologic, low-energy hip fracture treated at a single level 3 trauma center over a 65-month period. The causes of readmission and the outcomes of the readmitted patients will also be examined.
The objective of this study is to evaluate the costs, frequencies, and reasons for readmission after hip fracture. A secondary purpose of the study would be to compare the costs of readmission to the costs of the original admission.
Methods
Study Population
All patients aged 65 and older admitted to a 261-bed university-affiliated level 3 trauma center between April 30, 2005, and September 30, 2010, with a unilateral, native, nonpathologic low-energy proximal femur fracture were identified from a fracture registry and included for analysis. Patients with periprosthetic fractures, pathologic fractures, bilateral injuries, and high-energy mechanisms were excluded. All patients had retrospective chart reviews completed by a member of the research team as part of a hospital quality management initiative. Data were collected by a study nurse from patients directly and from their medical records and included demographic information, comorbidities, surgical management, in-hospital complications as well as any readmission within 30 days of original discharge. Readmissions within the original health care system, which includes 2 hospitals, were confirmed with the hospital’s admission tracking computer system. Six patients were readmitted to other regional hospitals. These patients were contacted by telephone for information regarding their readmission. Because data on costs of care could not be obtained, these patients were excluded from financial analysis. We also analyzed charges for care rather than actual costs because charges are typically reported by governmental reports.
Statistical analyses were performed on SPSS v20 software with statistical significance being reached on the 2-tailed student t test when P < .05. Univariate and multivariate logistical regression analyses were performed on characteristics of readmitted patients.
This study was approved by the university research subjects review board.
Results
Basic Group Characteristics.

Abbreviation: SD, standard deviation.
Of the surgical readmissions, 12 (9.3%) involved an injury that was caused by falling after hospital discharge. Of these 12 patients, 3 patients sustained a periprosthetic femoral fracture, 3 had a contralateral hip fracture, 2 dislocated their hemiarthroplasties, and 4 sustained nonhip fractures. Five patients developed surgical site infections. There were 3 patients with failed fixation—1 sliding hip screw cutout, 1 failed fixation of a femoral neck fracture (with cannulated screws), and 1 failed hemiarthroplasty that required reoperation. One patient was admitted with a hematoma. Eight (6.2%) patients ultimately underwent a reoperation.
Pneumonia represented the most common medical reason for readmission (27 patients, 20.9%). The next most common reasons were congestive heart failure (CHF) and atrial fibrillation (7 patients each, 5.4%). Mental status changes, renal complications (dehydration, acute renal failure, and hyponatremia), and other cardiac conditions (myocardial infarction) were other diagnoses associated with readmission.
Causes of Readmission.

aDeemed potentially avoidable readmissions. Died indicates patient died during the readmission stay.
Nineteen percent (24 patients) died during their readmission versus 2.8% during the index admission (see Table 2 for causes of death). When analyzing the 1-year mortality those patients readmitted within 30 days had a 1-year mortality rate of 56.2% versus 21.8% for those patients not readmitted (P < .0001).
Characteristics of readmitted patients.a
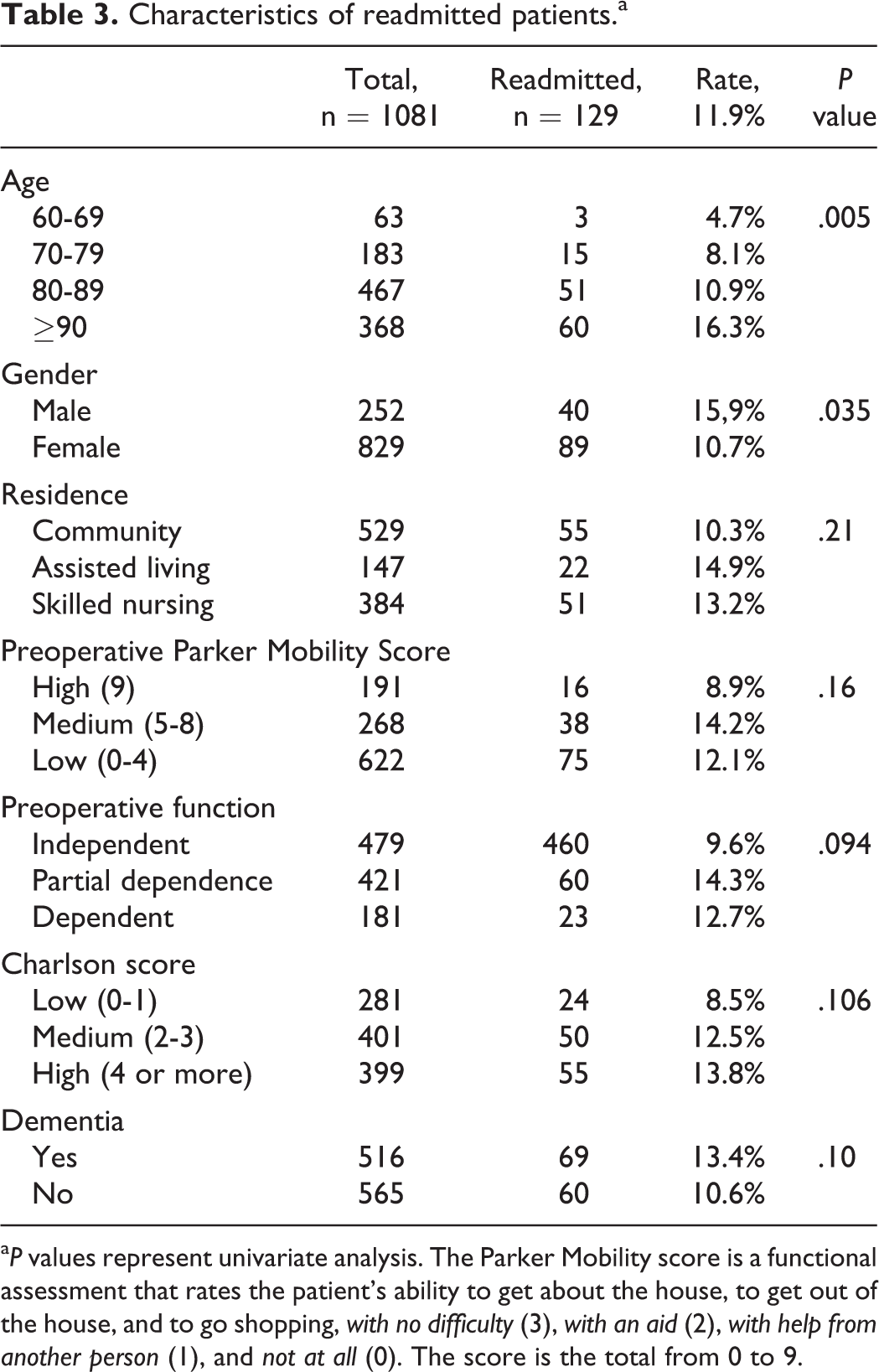
a P values represent univariate analysis. The Parker Mobility score is a functional assessment that rates the patient’s ability to get about the house, to get out of the house, and to go shopping, with no difficulty (3), with an aid (2), with help from another person (1), and not at all (0). The score is the total from 0 to 9.
Multivariate Analysis for Independent Predictors of Readmission.

Abbreviation: GERD, Gastroesophageal reflux disease.
aDenotes statistical significance (P < .05)
Hospital Charges by Diagnosis.a

Abbreviation: COPD, chronic obstructive pulmonary disease; SD, standard deviation.
aCharges were similar between groups.
Timing of Readmission by Diagnosis.a

aNumber of patients readmitted in each time period. Most readmissions occur within the first 14 days after hospital discharge.
Discussion
This is the first study looking at patient-level clinical and financial data on patients with hip fracture from the United States. Readmission to the hospital after hip fracture proved to be costly in our series. Readmission is often associated with serious medical and surgical complications of the original hospitalization, 1 –3,5,6 and this was true in this study. Not all hospital readmissions are preventable and many are certainly necessary. However, here we identified some reasons for readmissions that are indicators or poor quality and are potentially preventable (Table 2). In this study, 19% of readmissions were thought to have been preventable. These preventable causes can serve as targets for future quality improvement efforts.
Under PPACA, the Centers for Medicare and Medicaid Services (CMS) will begin to hold hospitals accountable for their medical readmission rates starting with 4 specific diagnoses. 4 This will be accomplished with public reporting of individual hospital readmission rates and decreased hospital reimbursement from CMS. 4
It is clear that government policy is capable of altering practice habits of clinicians through financial incentives or penalties. 13 Reducing payments and ultimately reducing monetary resource allocation toward the most costly medical conditions does not necessarily result in similar outcomes. 14
Patients with hip fracture may increase financial burden on the health care system before they have sustained a fracture. Kilgore et al recently studied 60 354 Medicare patients with hip fractures and found 88% of increased health care expenditure is directly associated with the fracture. 15 Furthermore, in the months leading up to their fracture, these patients consumed significantly more health care resources than matched controls. 15 Expenditures on every body system studied (ie, cardiovascular, pulmonary, endocrine, neurologic, genitourinary, etc) increased significantly after their hip fracture. This suggests that the patient who sustains a hip fracture is experiencing a general decline in health prior to his or her fracture. 15 Such patients may be targeted for prevention of hip fracture. More critical research into this topic may yield models that could potentially predict a patient’s risk of hip fracture, which may allow for preventive measures to be developed. Preventing hip fractures would likely lead to more significant cost reductions.
There is little guidance on how to reduce readmission after hip fracture. One study of 606 patients for 180 days after hip fracture found an readmission rate of 8.3%. 16 The rate varied by discharge destination—with inpatient rehabilitation (4.5%) and home (5.1%) having the lowest rates. Multivariate analysis in this study further supported that inpatient rehabilitation decreased readmission rates, while patients with longer LOSs had higher odds of readmission. 16 Buecking et al reviewed 402 patients with hip fracture (80% living at home alone or with family) and found a 12% readmission rate. 17 The majority (79%) were not related to their fracture, with respiratory failure (25%), cardiovascular morbidity (15%), and infectious disease (10%) being the most common reasons for readmission, all similar to our data in this study. 17 Multivariate analysis suggested that males and specifically femoral neck fractures had an increased risk of readmission. 17 Gender and fracture type are not modifiable risk of readmission. Discharge to inpatient rehabilitation, especially those with more comorbidities, may be a potential route for improving readmission rates. Admission requirements that must be met for Medicare inpatient rehabilitation are extensive. 16
French et al described a 30-day readmission rate of 18.3% using claims data from 41 331 US veterans aged ≥65 years with a hip fracture. 6 The readmitted patients in that study had a 1-year mortality rate of 48.5% compared with a 24.9% mortality rate in veterans who were not readmitted. 6 Bookvar et al described a prospective analysis of 562 patients with hip fracture aged ≥50 years. 5 They noted a 1-month readmission rate of 14.2%. Of these readmissions, 11% were readmitted for surgical causes and 89% were readmitted for medical reasons. These findings were very similar to our findings. They also describe a worsened prognosis for readmitted patients. Readmitted patients in their series were found to have an increased risk of mortality, impaired gait, and placement in a nursing home 6 months following fracture. 5 Jencks et al published a 30-day readmission rate of 17.9% after major hip or femur surgery and cited pneumonia and CHF as being the 2 most frequent causes of readmission. 2
The recently published Dartmouth Atlas report on readmissions highlights the considerable variation seen in readmission rates seen among both community and academic medical centers. 3 The specific causes for this variation are not clear. There has been no improvement in readmission rates over the past decade, 14.3% in 2004 and 14.5% in 2009. 3 For New York State hospitals, the rate in 2004 was 14.5% and increased to 15.3% in 2009. 3 Many causes for readmission have been described including communication issues, problems with medication reconciliation, lack of satisfactory follow-up care, and defects in the original inpatient care. 3,18 Other causes for readmissions may include shorter LOSs, increased age of the patients, and increased burden of comorbidity carried by these patients. Some have argued that many medical hospital readmissions are likely preventable in nature. 3 Typically, the inpatient care team only addresses the inpatient care phase 19 with no interventions extending past the inpatient stay.
The authors believe that some of our readmissions are likely of a preventable nature including some cases of constipation, cutout of implants, and congestive failure. 20 There are likely some cases that could be avoided with improved communication with receiving providers at the time of the discharge handoff. 21 There have been several successful methods published for reduction in readmissions following medical hospitalization including early follow-up care with the primary care physician, the Coleman discharge coaching model, and the Naylor model. 21 –23 There have been no published methods shown to successfully reduce readmission following hip fracture. Additional efforts at improving the discharge process, communication, and postdischarge follow-up may improve the readmission rates.
Limitations of this Study
There are several important limitations of this study. This is a single-center study conducted in a hip fracture program with a strong history for quality improvement, comanaged care, and utilizing standardized protocols. The sample size of 1081 with 129 readmissions is certainly not large enough to generalize these results. Larger, multicenter studies may be useful to determine whether these results can be generalized to other centers.
Another limitation is the retrospective nature of the data collection which may not fully capture all readmissions or adverse events. As a countermeasure, we have tried to capture all the 30-day readmissions by reviewing medical records and calling the patients, families, or caregivers following discharge. The patients included in this study may not accurately represent the populations seen at many centers. Half of our patient population were admitted from a nursing home or assisted (residential care) living home, whereas most published studies describe 80% to 90% of patients with hip fracture admitted from a home living setting. We were also unable to access a detailed data sample for 6 of the patients readmitted to regional hospitals. This is a limitation inherent to the US health care system where medical and economic data are typically not shared between regional hospitals.
Conclusion
Readmission after hip fracture is costly and harmful. Charges were similar between the original fracture admission and the readmission. Patients were readmitted most frequently for medical complications following their original hospital stay. The most common reasons for readmission include pneumonia, CHF, new fractures, intestinal obstructions, and infections. Of the patients, 19% died during their readmission, and the average readmission LOS was 8.7 days. Readmitted patients generated similar average hospital charges during readmission (US$14 191) compared to their initial hospitalization (US$16 308). Future research efforts should focus on techniques to reduce readmission rates after hip fracture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.