
Abstract
Background:
Early identification of hip fracture (HF) patients bearing an increased risk for a contralateral occurrence would allow providing preventive measures timely.
Objectives:
To summarize the available evidence describing risk scores, prognostic instruments, or (groups of) parameters predicting contralateral HFs at the time point of the first fracture.
Results:
Searches identified 3560 records, and 47 studies were included in this review. There was a large spectrum of study designs, patient populations, and follow-up periods. Among 11 studies reporting on a set of parameters, female gender was assessed most commonly (7 times), followed by age (5) and parameters of general health, vision, and stroke (each 4 times). We were unable to depict stringent patterns of risk parameters to be used for decision making in clinical practice.
Conclusions:
The findings of this article call for a conjoint effort to achieve an expert consensus regarding a critical set of parameters for a risk instrument identifying patients bearing an increased risk for contralateral HFs early.
Introduction
Contralateral hip fractures (HFs), particularly among elderly patients, are common and associated with poor prognosis. 1 Identifying patients at the time point of the first fracture bearing a substantially increased risk for contralateral HFs would allow planning therapeutic measures on the occasion of the fixation of the first fracture. Besides pharmacologic interventions, surgical treatments should then be considered. 2
However, such an invasive approach would only be justified if this group of patients could be selected and described accurately. Unfortunately, the literature reporting the parameters pointing at an increased risk is scattered and not easy to access. 2 Clinical experience teaches us that a previous HF is one of the strongest predictors for the next one. But, additional factors may further influence the risk for the next HF. Ideally, a simple algorithm that allows assessing the individual risk for a contralateral HF immediately prior to fixation surgery of the acquainted one should be available.
Using up-to-date systematic review methods, this article identifies and assesses the available evidence and provides an inventory of parameters found to be associated with an increased risk for contralateral HFs.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline, 3 and the protocol was registered at PROSPERO (CRD42014008972).
Eligibility
We aimed to find articles assessing at least 1 risk parameter at the time of the first fracture and its association with contralateral HFs. Studies were excluded if the type of first or second fracture was not clearly defined, risk factors for first HFs or mortality were investigated exclusively, or incidence of second HFs revealed only. We further excluded studies comparing first to second HFs in the same patient group, as these would not support finding a patient group at risk for second HFs. 4 –6 One study was not available for full-text review and therefore excluded. 7
Identification of Reports
Systematic searches were performed from inception in (pre-) MEDLINE and Scopus. The date of the last search was April 2014. The MEDLINE search is available in Appendix A.
Study Selection
After abstract and title scan, we included studies with German or English language full-text and those mentioning second HFs (also referred to as “contralateral,” “non-simultaneous,” “bilateral,” or “subsequent” “proximal femur” or “proximal femoral” fractures) in elderly patients. Studies with focus on pathological (cancer related or secondary to bisphosphonate treatment), periprosthetic, ipsilateral, or simultaneous bilateral fractures were excluded. Case studies and those referring to HFs as risk factor for other events were also excluded. In 2 studies, abstracts were not available. Therefore, we proceeded to full-text scanning directly. However, both studies did not meet our inclusion criteria.
Data Collection
After eliminating 18 duplicates, both search approaches together revealed 76 articles qualifying for full-text scanning. The main inclusion criteria after full-text review were the presence of at least 1 risk factor or 1 parameter that was compared between patients with and without second HF.
Data Extraction and Summary
Forty-seven articles fulfilled our inclusion criteria and were classified into 3 groups. “Group A” comprises studies revealing a set of risk factors for second HFs. This systematic review targeted at this specific group of articles. Studies of “group B” described to what extent risk parameters differed between groups of patients with a first HF and a second HF. Finally, some studies reported incidence ratios of second HFs in relation to a general population risk for first HF, mainly with standardized incidence rate ratios. Those studies were summarized in “group C.”
Other studies in contrary had looked for previous HF in a cohort of HF patients or investigated risk factors years after the first HF. Some were not defining the time of investigation in detail or allocated patients twice in 1 and 2 HF groups. Randomized controlled studies, matched control group, and intervention cohort studies do not reflect populations at risk and were therefore also not evaluated in group A.
We abstracted parameters that were assessed with similar methods to facilitate comparisons. For example, “functional status and ambulation” was measured by “time on feet < 4 h/d,” “using arms to stand,” “walking speed (m/s),” “using walking aids,” “difficulties standing up/walking up stairs,” and another 11 parameters for group A.
A statistical summary of the exiting evidence was attempted but impossible due to the large variation between individual studies in terms of patients selection, design, and statistical analysis.
Results
Study Selection
Searches identified 3560 records, of which, after applying the reported selection criteria, 47 articles qualified for inclusion in this review. The detailed selection process is shown in Figure 1.

Flow chart of the study selection.
In group A, we classified 11 studies 1,8 –17 (for details, see Table 1), group B contains 5 studies 18 –22 (see Table 2), and 31 reports went into group C 23 –51 (for details, see Table A1).
Summary of Studies of Group A.

Abbreviations: CI, confidence interval; HF, hip fracture; IQR, interquartile range; NG, not given; py, patient-years; SD, standard deviation.
Summary of Studies of Group B.
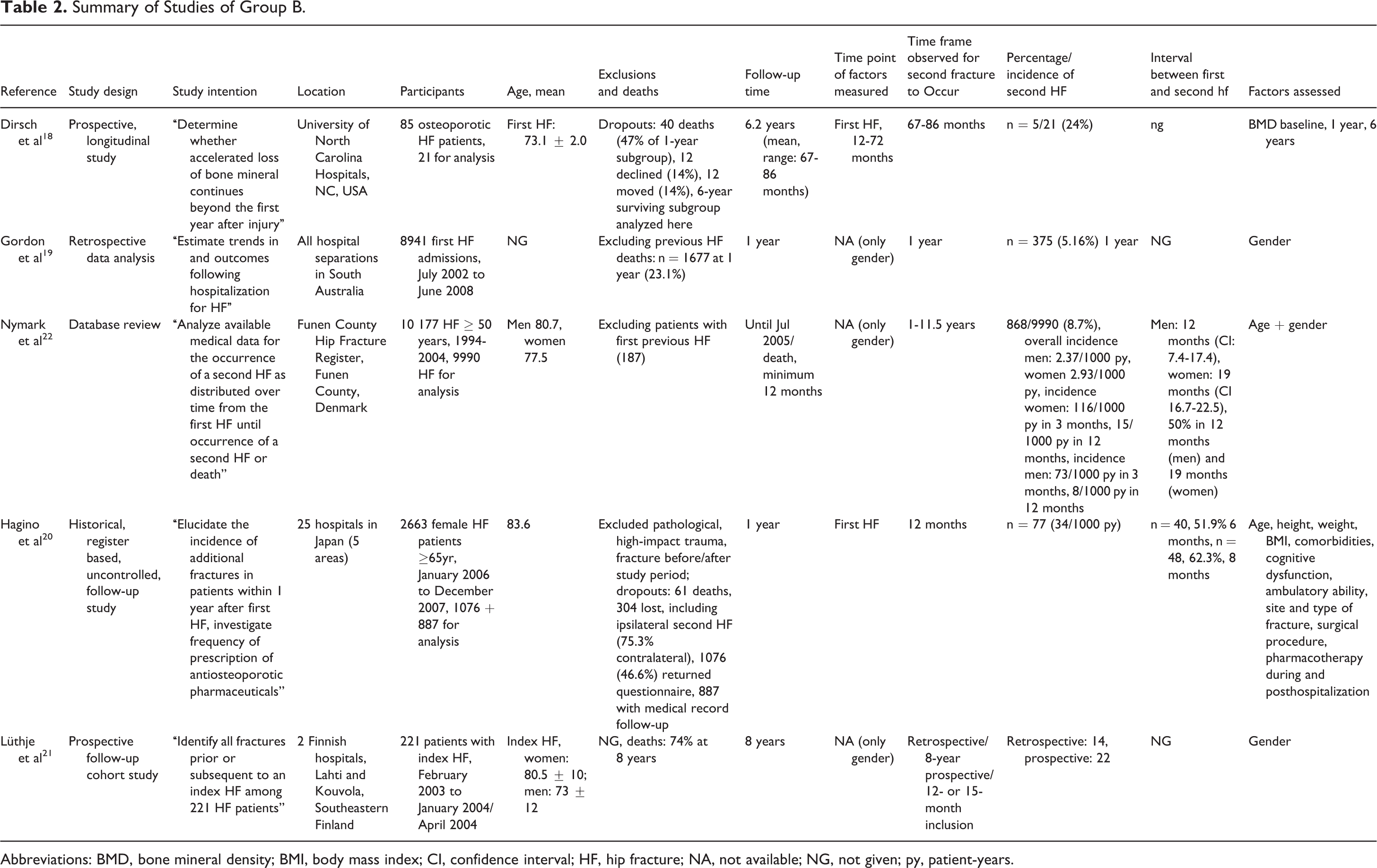
Abbreviations: BMD, bone mineral density; BMI, body mass index; CI, confidence interval; HF, hip fracture; NA, not available; NG, not given; py, patient-years.
Study Characteristics
In group A, 6 of the 11 studies had a prospective patient enrollment, 1,9,12,13,16,17 one was a nationwide population-based historical cohort, 1 and 4 assessed clinical data retrospectively. 8,13 –15 Among the 5 studies of group B, 2 had a prospective patient enrollment. 18,21 The observation period across all studies ranged from 6 months to 25 years. In group C, 8 studies assessed HFs retrospectively. Patient enrollment was unclear in 1 study and prospective in all the remaining. Six studies assessed HF risk in contrast to the fracture risk of the general population. Six other studies investigated modifiers of HF risk in the context of randomized controlled studies.
Incidence of Contralateral HFs
Incidence reporting across studies varied considerably and ranged from 2.3% patient-year 10,11 to 4.3% patient-year. 14 Prevalence of contralateral HFs could not be compared due to the large difference in observation periods. Among studies reporting the cumulative incidences at 1 year, the values ranged from 2.3% to 9.0%. 1,12
Frequency of Assessed Risk Factors
The 11 studies of group A underwent a detailed analysis of the definition and description of risk parameters assessed. Overall, 50 parameters were studied. The top 5 parameters where articles agreed were female gender (7 times reported), followed by age (5 reports) and parameters of general health, poor visual status, and stroke (each 4 times). Other important parameters (with 3 counts each) were the body mass index (BMI), presence of dementia, and institutionalization.
In those 4 articles that reported the results of multivariate analyses, the largest model contained 4 parameters (age, gender, BMI, and functional status). The capacity of single parameters or models to identify patients with an increased risk of second HFs ranged substantially. A detailed description of risk factor groups, individual risk factors assessed, and corresponding association measures are shown in Table 3.
Risk Factors Assessed in Articles of Group A.

Abbreviations: a, adjusted; ARR, absolute risk reduction; b, bivariate; BMD, bone mass density; BMI, body mass index; c, crude; COPD, chronic obstructive pulmonary disease; CRR, crude rate ratio; m, multivariate; HF, hip fracture; HR, hazard ratio; OR, odds ratio; RA, rheumatoid arthritis; RR, relative risk; u, univariate; yr, year.
Discussion
Main Findings
This systematic review found a substantial amount of studies investigating risk parameters for contralateral HFs in various populations and health care contexts without being able to depict a stringent set of parameters associated with a higher risk of contralateral HFs, which can be used in clinical practice. Moreover, association measures for single parameters varied considerably across studies.
Results in Context With the Existing Literature
We are unaware of any review proving a comprehensive inventory of studies assessing the role of various clinical characteristics as risk factors for second HFs. We are aware of one eminent large study by Ryg and coworkers that, although having a somewhat other focus, provide data from survival analyses allowing estimations of contralateral HFs over time. 1 Ryg and colleagues set out to study the incidence of contralateral HFs and its associated mortality risk. Moreover, they assessed whether specific comorbidity patterns were modifiers of that risk. They found a high incidence of second fractures within the first 5 years and a cumulative risk for fractures of up to 23% in that time period. Female gender, any previous fracture, diagnosis of alcoholism (based on the prescription of disulfiram or a corresponding diagnosis in the national Hospital Discharge Register or the Psychiatric Central Register), and living alone were parameters associated with a higher risk of mortality.
Strength and Limitations
To our knowledge, this is the first systematic inventory of prognostic parameters for contralateral HFs. The overview allows depicting patient patterns bearing an increased risk in a straightforward fashion. However, despite applying rigorous review methods, we were unable to go beyond a presentation of the available evidence. The evidence is very heterogeneous in terms of patient inclusions, design, and analysis to perform a methodologically sound meta-analysis. This is a common problem in descriptive prognostic research and meta-analyses thereof. 53,54 Due to the lack of articles developing or validating prediction models, we therefore had to limit ourselves to the presentation of single parameters or parameter groups and their association with contralateral HFs. Due to the data at hand, we had to ignore the possible correlation and interaction between individual risk parameters, making the comparison between individual studies challenging.
Implications for Practice
From our findings, no direct implications for clinical practice can be drawn because we were unable to identify studies reporting on diagnostic tools available at the moment of the first HFs, allowing to identify a subgroup of geriatric HF patients with a substantially increased risk of sustaining a short-term contralateral HF. Thus, postoperative pharmacological and physiotherapeutical treatment remain the most important cornerstones of secondary fracture prevention. 55 For patients who are unable to receive or adhere to adequate medical treatment like very old patients, those with low compliance, or contraindications, the treatment armamentarium remains limited at present.
However, this review identified some level of agreement regarding the relevance of female gender, patients’ age, the general health level, poor visual status, and stroke. Also, the BMI, presence of dementia, and institutionalization were commonly reported. In the absence of a carefully developed and also validated risk tool, these findings may give some indication in respect of an individual patient’s risk level.
Implications for Research and Conclusions
The findings of this article call for a conjoint effort to achieve an expert consensus for a critical set of parameters that, used in combination, could be used in a risk instrument for early identification and treatment of patients bearing an increased risk for contralateral HFs. This agreed set of risk parameters with a strong association with contralateral HFs should then be empirically tested in terms of discrimination and calibration within a sufficiently sized cohort of patients. The minimum set of parameters with the strongest predictive capacity should then undergo careful validation in new cohorts, ideally in different geographical regions, as differences in the baseline risk found in different countries may require adaptation of the risk instrument. At the same time, the effectiveness of an up-to-date medical treatment must be taken into consideration.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.