
Abstract
Introduction:
This systematic literature review evaluates (1) frailty in older adults as a risk factor for short-term adverse events and suboptimal clinical outcomes after total joint arthroplasty and (2) interventions to improve arthroplasty outcomes in these frail patients.
Methods:
PubMed, EMBASE, Cochrane Register of Controlled Trials, SCOPUS, AgeLine, and Web of Science were searched from database inception to November 22, 2017; gray literature and references were also searched. Studies including adults ≥65 years of age undergoing hip or knee arthroplasty and measuring preoperative frailty and postoperative adverse events or clinical outcomes within 90 days of surgery were included. Two investigators independently screened all abstracts and extracted data; disagreements were adjudicated by a third reviewer. Risk of bias was assessed using the Newcastle–Ottawa scale for cohort studies and the Cochrane Risk of Bias tool for randomized controlled trials. Study quality was assessed using a 5-point scale modified from the Oxford Centre for Evidence-Based Medicine tool.
Results:
Of 1913 abstracts identified, 82 full texts were reviewed, and 13 met inclusion criteria: 5 prospective cohort studies, 6 retrospective cohort studies, and 2 randomized controlled trials covering 382 763 total patients. These studies used 13 frailty instruments and assessed 32 distinct outcomes. Substantial heterogeneity precluded valid meta-analysis; results were qualitatively summarized by study design, frailty instrument, and outcome type. Of the 11 cohort studies, 10 found significant associations between frailty and poor postoperative outcomes. Trials of preoperative frailty-modifying interventions found no association between interventions and improved outcomes.
Discussion:
Standardizing frailty measurement would improve generalizability, permitting the assessment of associations with patient-reported and functional outcome measures, as well as the efficacy of interventions to improve outcomes, in frail patients undergoing arthroplasty.
Conclusions:
Frailty is associated with higher rates of short-term adverse events and worse clinical outcomes after elective hip and knee arthroplasty.
Introduction
Total joint arthroplasties (TJAs), including both knee and hip operations, are among the most common elective surgeries in older adults, but outcomes of these surgeries among the physiologically frail are not well known. Between 2010 and 2050, the global population over 65 years of age is estimated to increase by 188% and over 85 years by 351%. 1 By 2030 in the United States, primary total hip arthroplasties (THAs) are expected to exceed 572 000 and primary total knee arthroplasties (TKAs) 3 480 000 annually. 2 Although TJA is generally safe, 3,4 cost-effective, 5 and improves quality of life, 6 it is not without risk of serious adverse events (AEs) such as pulmonary embolus and death. 7 Additionally, despite advances in surgical technique, prosthesis design, and perioperative care, 7% to 23% of THA and 10% to 34% of TKA patients experience chronic postoperative pain that impairs quality of life. 8 ,9 Given the population burden and the associated societal costs, a better understanding of the relationship between physiological frailty and poor clinical outcomes after TJA is needed to guide patient care.
Frailty has been defined as “a clinically recognizable state of increased vulnerability, resulting from aging-associated decline in reserve and function.” 10 In other surgical populations, frailty has been found to predict postoperative AEs and poor clinical outcomes better than chronological age. 11 -18 Interventions targeting frail patients have the potential to improve AEs and clinical outcomes after TJA. There are no systematic reviews or meta-analyses of papers published on this topic to date. We, therefore, performed a systematic literature review to evaluate (1) existing data on frailty as a risk factor for AEs and suboptimal clinical outcomes after elective TJA in older adults and (2) interventions to improve TJA outcomes in these frail patients.
Methods
Review Design
This systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA, see Appendix 9). 19,20 The protocol was registered on the PROSPERO database (ID number 42016050652). See Appendix 1 for modifications to the original protocol.
Search Strategy and Selection Criteria
PubMed, EMBASE, Cochrane Central Register of Controlled Trials, SCOPUS, AgeLine, and Web of Science were searched, without language restriction, for original research articles evaluating any frailty measures in older adults undergoing TJA, from database inception to November 22, 2017. Searches included combinations of the following search terms: frail elderly, frail, dependence, vulnerable, decline, ADL (activities of daily living) disability, deterioration, or deficit accumulation; and aged, elderly, older, or geriatric; and hip replacement, knee replacement, hip arthroplasty, or knee arthroplasty. Gray literature sources were identified using the Grey Literature Report, Google and Google Scholar searches, and targeted governmental and organization websites. 21 Reference lists of included articles were hand searched for additional sources. In addition, the first and last authors of all included articles were hand searched in PubMed for additional articles. Two experienced research librarians gave critical input into designing the search strategies. See Appendices 2 and 3 for search details.
Eligible studies included patients aged 65 years or older, assessed patients’ preoperative frailty, and reported postoperative AEs or clinical outcomes within 90 days of TJA. Frailty assessments based on preoperative patient characteristics from self-report data, performance measures, and database algorithms were considered. Studies evaluating unicompartmental TKA, hip resurfacing, revision, and bilateral surgeries were included; arthroscopy and meniscectomy were excluded. Studies including only hip fracture surgery were excluded; however, studies evaluating a composite group of both elective THA and THA for hip fracture were eligible for review. We assessed the following outcomes: AEs such as postoperative myocardial infarction, clinical outcomes such as cognitive status and pain, and health-care costs and utilization (eg, readmissions, transfers to intensive care). Articles were excluded if the study design was other than randomized controlled trial (RCT), cohort, or case–control. When multiple articles reported on overlapping cohorts, the study with the largest sample size was included. Published abstracts, conference papers, and unpublished papers were eligible.
Study Selection and Data Extraction
Two investigators (A.M.S. and L.A.M.) independently screened titles and abstracts and then screened full texts of articles selected for review. Study de-duplication and management were performed using Covidence software. 22 One investigator (A.M.S.) extracted data on study design, patient characteristics, frailty measurement, outcomes, and associations between frailty and outcomes. A second investigator (L.A.M.) verified data extraction. Authors were contacted to obtain missing data. Disagreements at any stage were resolved by consensus or adjudicated by a third investigator (N.H.).
Data Analysis
Substantial variation in frailty assessment and outcome types (see Tables 1 -3) across the studies precluded valid combination of individual studies into a quantitative meta-analysis. The evidence was qualitatively summarized by study design, frailty measurement, and outcome type.
Characteristics of Included Studies.

Abbreviations: RCT, randomized controlled trial; SD, standard deviation; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Frailty Instruments and Domains Assessed.a

aX indicates measured by the instrument.
Outcome Measures.a

Abbreviations: GCP, Good Clinical Practice; HOOS, Hip Disability and Osteoarthritis Outcome Score; ICU, intensive care unit; NSQIP, National Surgical Quality Improvement Program.
aO indicates measured by the study; X indicates significant association with a frailty measure.
Evaluation of Risk of Bias and Quality Assessment
Two investigators (A.M.S. and L.A.M.) independently evaluated the risk of bias of each study using the Cochrane Risk of Bias tool for RCTs and a modified Newcastle–Ottawa Scale for nonrandomized studies. 23,24 In place of the third Newcastle–Ottawa question called “ascertainment of exposure,” a question about frailty assessment was substituted. Credit was awarded for this question if the study used a performance measure, self-report instrument, or database algorithm that was validated in a geriatric population. Two investigators (A.M.S. and L.A.M.) independently evaluated the quality of evidence for each study using a 5-point scale modified from the Oxford Centre for Evidence-Based Medicine (see Appendix 7). 25 Disagreements at any stage were resolved by consensus or adjudicated by a third investigator (N.H.). The aim of this review was to inclusively report on all studies evaluating frailty and outcomes in TJA patients; therefore, no studies were excluded on the basis of risk of bias or quality.
Results
Search Outcome
Database searching yielded 3323 records (PubMed 862, EMBASE 936, SCOPUS 970, Cochrane 120, AgeLine 189, Web of Science 246). Gray literature searching resulted in 56 additional records. Missing data were requested from the authors of 10 publications; all provided additional information. Following de-duplication, we screened the titles and abstracts of the remaining 1913 articles and excluded 1831. The full texts of the remaining 82 were reviewed, and 13 were included in the qualitative synthesis. See Figure 1 for PRISMA diagram.
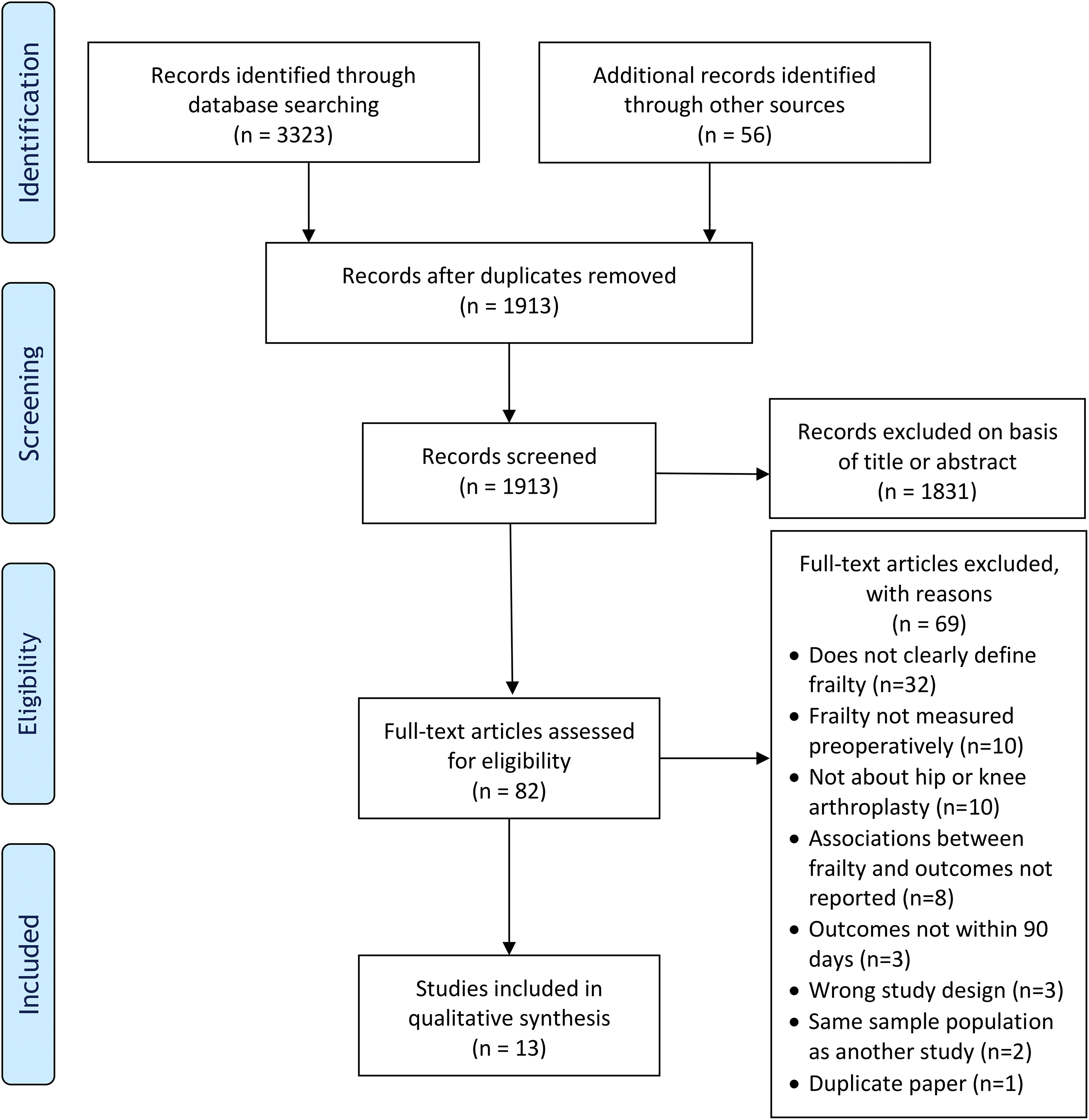
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Diagram.
Study and Patient Characteristics
Table 1 and Appendix 4 summarize the 13 studies that met the eligibility criteria: 5 prospective cohort studies, 6 retrospective cohort studies, and 2 RCTs. Of the 13 studies, 10 included only older adults above a certain age threshold, and the other 3 studies included adults of all ages. All studies had a mean age of greater than 60 years. In the studies reporting gender, more than half of the participants were female (range: 55.6%-93%). Seven studies included only THA patients, 1 included only TKA patients, and 5 included both THA and TKA patients. Nine studies included only elective surgeries, and 4 did not specify whether they limited their cases to elective procedures.
Frailty Measures
Thirteen different frailty instruments—10 in-person assessments and 3 calculations using previously collected data—were used in the studies reviewed here. Four of these were used in more than 1 study (see Table 2). Of the 13 studies, 2 controlled for comorbidities (using Charlson or Charnley scores) and another 5 incorporated comorbidities as a part of their frailty assessment. The remaining studies—which included both interventional trials—did not report on the interplay of frailty and comorbidity.
Postoperative Outcomes
Among the 13 studies, 32 different outcome measures were reported, including AEs, process issues, and clinical outcomes. Table 3 lists the specific outcomes measured and their associations with frailty measures. In particular, significant associations were found between frailty and death, pulmonary embolism, myocardial infarction, and reoperation within 30 days.
Summary of Evidence by Study Type
Cohort studies
Of the 11 cohort studies, 10 found associations between frailty measures and postoperative AEs or clinical outcomes. Gordon et al 26 and Woodard et al 27 both found moderate correlations between the Edmonton Frail Scale 28 and length of hospital stay in TJA patients (Gordon: Spearman ρ = .425, P < .01; Woodard: Spearman ρ = .368, P = .28). In THA patients, Oosting et al 29 found worse Risk Assessment and Predictor Tool (RAPT) scores 30 were significantly associated with delayed inpatient recovery of function (defined as taking 4 days or more to walk independently based on the Modified Iowa Levels of Assistance Scale); an RAPT score of 6 to 9 had an odds ratio (OR) of 4.39 (95% confidence interval [CI], 1.18-16.30), and an RAPT score of 0 to 5 had an OR of 6.46 (95% CI, 1.48-28.16). The same investigators also found that a slower 10-m walk test was significantly associated with delayed inpatient recovery (OR, 4.19; 95% CI, 1.22-14.40). 31,32 Postler et al 33 found that a higher Barthel score, measured on the day of admission, was associated with a significantly shorter inpatient stay for THA patients, but they did not quantify this relationship. McIsaac et al 34 showed that frailty, as measured by the Johns Hopkins Adjusted Clinical Groups frailty-defining diagnoses indicator, 35 was significantly associated with higher rates of intensive care unit admission (OR, 2.52; 95% CI, 2.21-2.89), discharge to institutional care (OR, 2.09; 95% CI, 1.93-2.25), 30-day readmission (OR, 1.33; 95% CI, 1.07-1.66), and 30-day mortality (hazard ratio, 3.03; 95% CI, 2.62-3.51); longer length of stay (incidence rate ratio [IRR], 1.62; 95% CI, 1.59-1.65); and greater total health-care costs at 30 days (IRR, 1.16; 95% CI, 1.15-1.17), 90 days (IRR, 1.35; 95% CI, 1.33-1.37), and 1 year (IRR, 1.53; 95% CI, 1.51-1.56) in TJA patients. Graham et al 36 showed a significant association between increasing scores on the Electronic Frailty Index 37 and mortality (P < .0001). The remaining 4 papers all showed significant associations between the modified Frailty Index 38 and postoperative outcomes. Shin et al 39 showed significant associations with Clavien-Dindo grade IV complications 40 within 30 days of THA (OR, 5.140; 95% CI, 1.400-18.871) and TKA (OR, 4.183; 95% CI, 1.464-11.948). Bellamy et al 41 showed significant associations with mortality (OR, 2.45; 95% CI, 2.08-2.88), readmissions (OR, 14.72; 95% CI, 6.95-31.18), complications (OR, 3.63; 95% CI, 1.64-8.05), and reoperations within 30 days of THA (OR, 8.78; 95% CI, 3.67-20.98). Ondeck et al 42 showed significant associations with extended length of stay (area under the curve [AUC], 0.618; 95% CI, 0.607-0.630), discharge to facility (AUC, 0.605; 95% CI, 0.600-0.609), and Centers for Medicare and Medicaid Services procedure-specific complication measures (CMS-PSCMs) within 30 days of THA. Group 1 CMS-PSCMs included acute myocardial infarction, pneumonia, and sepsis/septicemia/shock (AUC, 0.657; 95% CI, 0.638-0.677); group 2 included surgical site bleeding, pulmonary embolism, and death (AUC, 0.576; 95% CI, 0.537-0.616); and group 3 included mechanical complications and periprosthetic joint/wound infection (AUC, 0.556; 95% CI, 0.537-0.575). Runner et al 43 showed associations with mortality (OR, 2.10; 95% CI, 1.73-2.55), readmissions (OR, 8.71; 95% CI, 2.11-35.98), complications (OR, 1.58; 95% CI, 1.15-2.16), and reoperations within 30 days of TKA (OR, 3.32; 95% CI, 1.36-8.11).
One of 11 cohort studies did not find a significant association between a frailty measure and postoperative AEs or clinical outcomes. Mandl et al 44 used a composite frailty scale derived from select items from the Fried 45 and Robinson 46 frailty scales. They did not find significant associations between frailty and short-term AEs; they did not quantify these relationships beyond the lack of statistical significance.
Randomized controlled trials
A research team in the Netherlands conducted 2 pilot RCTs evaluating the feasibility and effectiveness of preoperative physical therapy for frail older patients planning elective THA. Hoogeboom et al 47 enrolled patients scoring ≥2 on the Clinical Frailty Scale. 38 Patients either trained twice weekly at a physiotherapy department for 3 to 6 weeks before surgery or received standard of preoperative care. They found no difference in length of stay (P = .288) or time to functional recovery based on the Iowa Levels of Assistance Scale (P = .963). 31,32 Since they were only able to recruit 34% and retain 91% of potentially eligible patients, they questioned the feasibility of a larger RCT. Oosting et al 48 randomized patients scoring ≥2 on the Identification of Seniors at Risk 49 to receive home-based physical therapy twice a week for 3 to 6 weeks before surgery, or care as usual. They reported that there were no significant differences in in-hospital complication rate, length of stay, or functional recovery based on an Iowa Levels of Assistance Scale <6 on day 4, but did not quantify the relationships. Measures of pain and function did not differ significantly between the intervention and usual care groups. The design of this study, with home-based physical therapy in place of clinic-based physical therapy, improved upon that of the Hoogeboom study; with home-based physical therapy, the recruitment rate was 70% and the adherence rate was 99%.
Risk of Bias and Quality of Included Studies
Cohort studies ranged from 6 to 9 stars on the Newcastle–Ottawa Scale (range, 0-9; lower score indicates greater risk of bias). Common sources of bias included not controlling for age and gender in models and not reporting whether all participants were accounted for in follow-up. Both RCTs had high risk of bias based on the Cochrane Risk of Bias tool due to insufficiently blinding participants and assessors, small sample sizes, and poor recruitment (7 domains; each scored as low or high risk of bias). Risk of bias assessments can be found in Appendices 6 and 7. All studies scored a 2 or 3 on the quality rating scale, since they were cohort studies and small pilot RCTs. Study quality assessments can be found in Appendix 8.
Discussion
This systematic review confirms and extends prior findings of negative consequences of physiological frailty in the postoperative period, showing that frail older adults undergoing elective TJA have higher rates of postoperative AEs and poorer short-term clinical outcomes than their nonfrail peers. Only 1 of 11 reviewed studies failed to report an association between frailty and poor short-term outcomes after TJA; this was an interim analysis of an ongoing study and so may have been underpowered. 44 These findings are particularly relevant for older adults choosing elective surgery to improve quality of life. Elective procedures are only performed on patients who are deemed medically well enough to be surgical candidates. The finding that frailty is associated with poor outcomes, even in this relatively healthy population, underscores the fact that frailty measures a domain not captured by standard preoperative medical review.
This systematic review focuses on outcomes that occurred within 90 days postsurgery. While short-term outcomes are important, TJAs are meant to be durable interventions to improve long-term pain and function. It will, therefore, be important to identify long-term, patient-centered, clinically relevant postoperative outcomes associated with frailty. Preoperative frailty may be associated with long-term postoperative health-related quality of life domains, such as depression, anxiety, and self-efficacy, which could modulate objective pain and function improvements of TJA. In addition, frailty may be associated with other important domains, such as satisfaction with surgery and willingness to have the surgery again, if needed. Considering that as many as 1 in 4 TKA patients and 1 in 5 THA patients do not experience any clinically meaningful change in pain level after surgery, it is intriguing to speculate that frailty may impact long-term pain and function. 9,50,51
Since frailty predicts worse outcomes after TJA, future research should focus on feasible and effective interventions to decrease frailty preoperatively. Almost all arthroplasties are elective, and thus, there is a window of opportunity when an intervention could be administered, with no risk to the patient of delaying the procedure. Attempts have been made to intervene preoperatively to improve TJA outcomes, most commonly with physical therapy; however, most studies have not specifically focused on frail patients. A 2015 systematic review by Wang et al found patients who received prehabilitation prior to TJA experienced a slight improvement in postoperative pain and function, but the effect was too small and short term to be clinically important. 52 The study did not stratify based on frailty and may have missed a potentially positive effect for this specific population.
The RCTs included in this systematic review suggest that home-based, rather than hospital-based, physical therapy prior to THA (so-called “prehabilitation”) is the preferred approach; however, they did not find any significant differences in outcomes between those who received physical therapy versus those who received usual care. These small, underpowered pilot studies provide important preliminary data, which should be used to inform the design of future trials, but do not provide definitive guidance regarding the utility of preoperative intervention in frail arthroplasty patients. It will be important to design adequately powered studies of carefully phenotyped THA and TKA patients to ensure optimization of outcomes in this vulnerable population.
Multimodal interventions, which include educational, social, nutritional, or other interventions in addition to physical therapy, may potentially be more effective for frail patients undergoing TJA. Nonorthopedic surgical specialties have successfully implemented multimodal interventions prior to surgery. 53,54 In a 2014 overview of frailty, Chen and colleagues suggest multimodal interventions could “prevent, delay, reverse, or reduce the severity of frailty” or “prevent or reduce adverse health outcomes in those whose frailty is not reversible.” 55 Implementing a multimodal intervention among frail TJA patients would require careful phenotyping of patients preoperatively, to allow appropriate targeting of those with modifiable frailty traits and provide additional support of those with fixed frailty-defining deficits. A small pilot trial examining the feasibility of a multimodal intervention for frail patients undergoing TJA is currently in the process of recruiting. 56 Results and lessons learned from small pilot trials will be crucial to inform the design and implementation of larger randomized interventional trials.
Future trials should strive to evaluate THA and TKA patients separately, since these populations differ significantly. In particular, TKA patients are generally younger, have higher body mass index, and are more likely to be female, 57 which is likely why frailty interventions to date have focused on THA. There is, however, a clear need to better understand the effect of frailty on TKA outcomes as well. Preliminary data from Hospital for Special Surgery indicate that at least 8% of TKA patients are frail. 44 Given current projections, this would correspond with >278 000 frail TKA cases annually in the United States by 2030. 2 These absolute numbers are likely to increase dramatically as TKA volume is projected to increase even more than THA volume over the coming decades. 2
Standardizing and operationalizing the definition and measurement of frailty would benefit future scholarship about frailty in particular and geriatric care in general. Currently, there is no gold standard for measuring frailty; a 2016 review of frailty assessment tools identified 79 distinct instruments, and recent articles frequently propose new definitions and assessment tools. 1 We found that the 13 included studies used 13 different frailty measures. Among the instruments used to assess frailty or components of frailty, the Barthel index, which includes measures of disability, was used in 2 studies. However, frailty is considered to be a reversible predisability and does not necessarily lead to disability, suggesting that the Barthel index may not be the most appropriate metric for its evaluation. 58,59 Establishing a common, consistent framework for operationalizing frailty would not only separate frailty from related concepts such as disability and comorbidities but would allow for better cross comparison between diseases and populations. Although progress has been made to standardize the measurement of frailty, 60 -63 consensus has not yet been achieved.
Strengths of this review include rigorous adherence to best practices for systematic reviews, including registering in PROSPERO and following the PRISMA guidelines. To minimize publication bias, we reviewed multiple databases, including EMBASE and Web of Science, which index conference proceedings and abstracts regardless of publication status in peer-reviewed journals, and extensive hand searches were performed, including gray literature searches. In addition, investigators were contacted personally to obtain missing data.
Limitations include the heterogeneity among studies with respect to study design, frailty measurement instruments, outcomes, and overall quality of the included studies. It is also possible that variation in the way that frailty literature was indexed resulted in some missed references. To minimize this potential limitation, 2 experienced research librarians gave critical input into designing the search strategy. Future systematic reviews can use the MeSH term frailty, which was introduced in 2018, in addition to the keyword frail or frailty and the legacy index term frail elderly.
Conclusion
To our knowledge, this is the first systematic review showing frailty is a significant predictor of poor outcomes after TJA in older adults. The sparse data from interventional trials in frail TJA patients suggest this is an area for additional research. Furthermore, identifying effective and feasible interventions to improve preoperative frailty in this rapidly growing patient population could have a significant impact on both quality of life and associated societal costs, particularly in the coming era of bundled payments and value-based reimbursement. 64
Supplemental Material
Supplemental Material, Supplement_Revised_Clean_20181102 - The Impact of Frailty on Short-Term Outcomes After Elective Hip and Knee Arthroplasty in Older Adults: A Systematic Review
Supplemental Material, Supplement_Revised_Clean_20181102 for The Impact of Frailty on Short-Term Outcomes After Elective Hip and Knee Arthroplasty in Older Adults: A Systematic Review by Abigail M. Schmucker, Nathaniel Hupert and Lisa A. Mandl in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Acknowledgments
The authors thank librarians Rie Goto from Hospital for Special Surgery and Michelle Demetres from Weill Cornell Medicine who provided invaluable technical support. The authors are also grateful to the authors of cited studies who generously provided supplemental materials in response to our inquiries.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.